IJCRR - 13(20), October, 2021
Pages: 155-161
Date of Publication: 24-Oct-2021
Print Article
Download XML Download PDF
Association of ABO Blood Group with Oral Cancer and Precancer - A Case-control Study
Author: Isha Gaurav, Vela Desai, Karamdeep Singh, Satinder Singh, Sukhmani Sanghera, Anmol Kaur, Alisha Madan
Category: Healthcare
Abstract:Background: Oral cancer is creating an alarming situation globally. It is the commonest cancer in India, accounting for 50\?70% of total cancer mortality. Oral cancer is amenable to primary and secondary prevention. The relationship between ABO blood groups and carcinogenesis or progression of human tumors has been reported by many investigators. Aim: To evaluate the association of ABO Blood Group System with Potentially Malignant Oral Lesions and Oral Cancer and also assess other risk factors associated with age, sex and tobacco habit. Material and Method: The research was a case-control study including 200 subjects selected using the random sampling technique into 4 groups, two control and two experimental 100 each. Details regarding demographics and oral habits were noted followed by blood group testing and comparison of blood groups and Rh status of all 4 groups. For statistical analysis, a Chi-square test was used to assess the relationship between ABO blood groups and oral precancer and cancer. The probability level was fixed at ≤0.05. Results: A significant association between the blood group A and the defined diseases could be determined. Common age group for Oral cancer was found to be 51-60 years with male preponderance. Oral Submucous Fibrosis was the most prevalent precancerous disorder with smokeless tobacco being the chief etiological factor. Conclusion: ABO blood group may have a role in the causation of oral precancer and cancer, and this novel finding provides a hint that ABO blood group may be used as a possible indicator although we cannot rule out the presence of residual confounding by other predisposing factors for oral cancer. Nonetheless, further investigations that include more diverse study populations are warranted.
Keywords: ABO blood group, Oral Precancer, Oral Cancer, OSMF, Risk factors, Biomarker
Full Text:
Introduction
Oral cancer (OC) is the commonest cancer in India, accounting for 50–70% of total cancer mortality and accounts for the highest incidence among Asian countries.1
Global descriptions of international patterns and trends in oral cancer are informative in providing insight into the shifting epidemiologic patterns and the potential prevention of these tumours.2
Oral cancer is amenable to primary and secondary prevention.3 Intense efforts towards early detection and prevention are required. A decision to introduce population-based screening should be taken into account which requires development of an affordable, acceptable, easy to use, reliable and easily identifiable biomarker to combat with the cost of screening.
It is known that oral cancer is caused by the interaction between environmental factors and genetic variations. Tobacco chewing is generally considered as the primary local etiological factor for oral cancer with smoking and alcohol acting as co-factors.4
Recent studies have revealed the possibility of ABO blood group antigens role in development of cancer.
ABO blood group is one of genetic factors that has been hypothesized in the aetiology of various chronic diseases. The association between ABO blood group and risk of cancer has been known for more than 60 years but received little attention. The author in the year 1953 were the first to notice the correlation between gastric cancer and blood group A.5 Since then, the relationship between ABO blood groups and carcinogenesis or progression of human tumors has been reported by many investigations.6 In India, studies have shown that individuals with blood group A have a predisposition for oral cancer. Association between ABO blood group and the risk of cancer might vary among different races or ethnicities.7 We decided to further prove the hypothesis on a defined population of East central Rajasthan and also included potentially malignant disorders that serve as precursors of oral cancer in the study. By performing this simple test and counselling the susceptible genera might reduce a load of oral cancer in our population.
Aim
The present study aimed to evaluate if any of the ABO blood groups are associated with increased risk of precancer and cancer and also assess other risk factors associated with age, sex and tobacco habit.
Material and Methods
The study was conducted in Jaipur Dental College and RUHS College of Dental Sciences, Jaipur, Rajasthan. The study aimed to assess the consideration of the blood group as a risk factor in the occurrence of precancer and cancer. The study was based on the assumption that blood group type is a risk factor in the causation of cancer in various parts of the body and there was an urge to further research if the assumption holds for oral cancer and potentially malignant disorders.
200 subjects were included in the study, randomly selected from patients attending the OPD of Jaipur Dental College and RUHS College of Dental Sciences in 4 groups - two control and two experimental 200 each. The 4 groups of data collection in the study were as follows:
• 50 healthy individuals
• 50 healthy individuals with tobacco habit but no lesion
• 50 individuals with potentially malignant lesions
• 50 individuals with oral cancer
The subjects were drawn from the general population visiting OPD during a specified period.
The sample selection criteria were as follows.
Inclusion Criterion
• Subjects who gave informed consent.
• Subjects matching the diagnostic criteria for various potentially malignant lesions.
• Subjects with oral cancer that were histopathologically confirmed.
Exclusion Criterion
• Subjects with no histopathological confirmation for oral cancer.
• Subjects with the genetic disorder.
• Subjects with any sort of bleeding disorder or on oral anticoagulants.
• Subjects with a critical illness.
• Subjects not willing to be part of the study.
All the study subjects were personally interviewed regarding their socio-demographic profile, medical history, oral hygiene, dietary history, tobacco habit history using a structured Performa. Tobacco history including type (chewing, smoking or both), frequency, and duration was recorded.
After acquiring all the relevant information regarding the demographic profile of the subjects, a thorough oral examination was done.
Patients belonging to the healthy group were then subjected to the ABO blood grouping procedure. Patients having oral lesions (Potentially malignant or oral cancer) were further evaluated. The four most frequently encountered potentially malignant disorders were considered in the study.
1. Leukoplakia
2. Oral Submucous Fibrosis
3. Oral Lichen Planus
4. Combination of any of these
Toluidine blue testing was done for all patients having oral lesions and patients suspected of malignancy were considered for biopsy.
This was followed by ABO blood group testing. Various blood typing techniques have been available which is different from each other in many prospectuses. . In this study we used the Slide Method due to its following advantages: The test completes in 5–10 min, is inexpensive and requires only a small volume of blood typing reagents.
Statistical Analysis
All the subjects data were recorded and entered in separate Excel sheets (Microsoft Excel, Microsoft Office 2010, USA). After that, the data were evaluated statistically using SPSS software (Statistical Package for Social Sciences). The Chi-Square tests with Fisher’s definitive test were used to compare and reach the conclusion for the results of this study.
Results
The study sample had 4 groups – Healthy, Habit without lesion, precancer and oral cancer. Age and sex were matched for the Healthy group.
Table 1 and Graph 1 shows the age-wise distribution of the sample. The 4 subject groups were sorted into 7 age groups wiz. 21-30 years, 31-40 years,41-50 years,51-60 years and 61-70 years. In the healthy group, the subjects were selected equally in each age group in a count of 10 totalling 50. Most subjects in the habit without lesion group belonged to the 21-30 age group. Likewise, subjects in precancer and oral cancer belonged to 41-50 and 51-60 respectively.
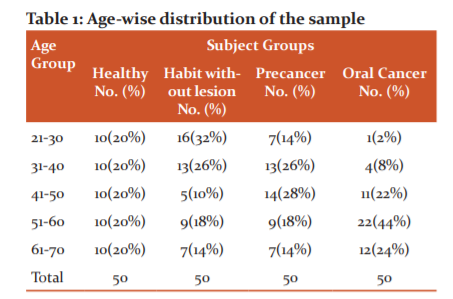
Table 2 demonstrates the no. of males and females in the 4 groups. Males were found to be more in the habit without lesion group, precancer group and cancer group.
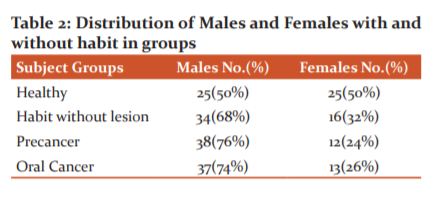
Table 3 depicts the frequency of various precancerous lesions in the study group. OSMF was the most frequently encountered precancerous lesion followed by Leukoplakia, OLP and a combination of these lesions.
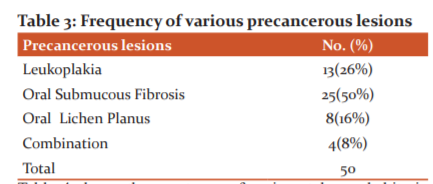
Table 4 shows the constancy of various tobacco habits in subjects groups and it was seen that smoking was more prevalent in the habit with no habit lesion group whereas smokeless tobacco was more prevalent in the precancer and oral cancer groups
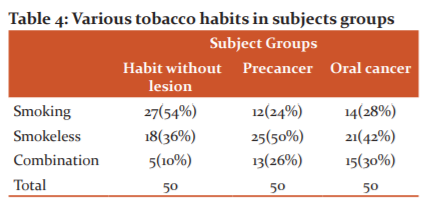
Table 5 summarizes the variance of blood groups in the sample. The frequencies of blood types A, B, AB and O were B(56%)>O(36%)>A(4%)=AB(4%) among healthy participants while those for habit without lesion group were O(38%)>B(34%)>A(20%)>AB(8%). These were compared to precancer and oral cancer group showing A(38%)>B(34%)>AB(20%)>O(8%) for Precancer and A(50%)>B(30%)>O(18%)>AB(2%) for Oral cancer. Chi-Square test (table 6) with significance level set as .05 demonstrated a significant difference with blood group A preponderance for both Precancer and Oral Cancer.
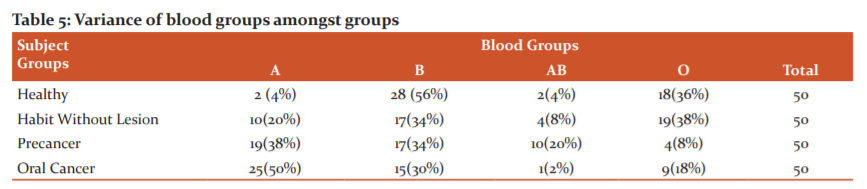
Table 6 Chi-square analysis for the association of Blood groups in various groups

Discussion
India has one-third of oral cancer cases in the world.8 40% of cancers of the body in India are oral cancers. Cancer in its all forms accounts for about 12% of deaths throughout the world and is thus considered a killer disease.9
The prime reason for this high mortality and morbidity is attributed to the delay in diagnosis and prompt treatment. Relentless research in the field of oncology has led to the advent of novel procedures for the early detection of oral cancers.10
While most of the efforts usually focus on therapy and outcomes, the need for risk factors evaluation, screening for early detection cannot be overlooked.11
Oral cancer to a large extent is a self-induced disease. To plan preventive measures, it is important to understand the risk factors associated with the disease.12
The two main factors which influence most diseases are genetic and epigenetic.13
Epigenetic factors like cigarette smoking, tobacco chewing, body mass index, diet, poor oral hygiene vary with lifestyle. The ABO blood group is a genetically determined variable and therefore is not a modifiable risk factor.
ABO blood group is an easily accessible factor in a patient’s genetic make-up.14 The relationship of blood groups with incidence, clinicopathologic parameter, and prognosis has been studied in many cancers, such as gastric, breast, skin, oesophagus, cardiac, lung, laryngeal, hypopharyngeal, salivary gland, gynecologic, colorectal, pancreatic, bone, urinary bladder, renal, testicular, uveal melanoma, and prostate. In some tumours, alteration of ABO antigens is associated with malignant transformation. Apart from cancers, ABO blood groups have also been associated with disease entities, such as pulmonary tuberculosis, leprosy, syphilis, malaria, coronary artery disease, diabetes mellitus, vitiligo, infertility, schizophrenia, goitre, glucose-6-phosphate dehydrogenase deficiency, gout, and hepatic dysfunctions.15
In the present study blood group, B was found to be the maximum among the healthy group owing to the generalized prevalence of the B blood group in the population of Rajasthan followed by blood Group O, A and AB. Also, Rh-negative subjects were low in the overall control and study group.
This is by a study done by Behra and Joshi (2013)16 in Rajasthan revealing that the commonest ABO blood group is B(36.4%), followed by O (31.7%), A(22.2%) and AB(9.4%) respectively. Rh Positive are 91.75% and Rh-negative is 8.25%.
In our study, the frequency of blood group "A" was predominant in both Precancer and Oral cancer groups.
One of the authors has cocluded that there is increased risk of cancer of the stpomach in the patients having Blood Group A as compared to those who were having blood group O.5
Although studies relating ABO, Precancer and Oral cancer have shown variable results.
Bryne et al.18 demonstrated no significant results; Jaleel BF et al.9, S Bhateja and G Arora15, Saxena S et al.19, Venu K et al.20, Shishodia NP et al.21 showed a preponderance of blood group A; Mortazavi H et al.22, Jyoti Byakodi JR and Pushpanjali K23 2014, Nikam P et al.24, Ramesh G et al.25, Rao S and Abraham TT 11 concluded blood group B to be responsible for increased risk for oral cancer; Singh K et al.26, Kakava K et al.27 found blood group O to be the culprit; Jalili L et al.28, Gupta DK et al.29, manifested the predominance of blood group AB.
There is a lot of literature showing the association of various blood groups with ceratin specified type of cancer, however different authors have a different opinions in this regard. The difference in the research could be due to the assessment of the small size of the sample, wider variation of ABO frequencies occurring over relatively limited areas even in populations considered ethnically homogeneous30,31
The antigen of ABO blood groups has been expressed on the outermost surface of the human tissues such as epithelium sensory neurons, platelets, and the vascular endothelium.32
Certain authors have suggested that the ABO blood group antigens should be termed ABH histo-blood group antigens to emphasize that they are primarily tissue antigens.33,34 ABH antigens appear earlier in evolution in ectodermal or endodermal tissue than in mesenchymal hematopoietic tissue and cells, including RBCs.33
ABO blood group system extends beyond transfusion medicine and several reports have suggested an important involvement in the development of cardiovascular, oncological and other diseases
The underlying mechanism for the possible relationship between blood type and cancer has not been clearly defined to date. Some investigators have proposed that the ABO gene products themselves have a direct role in tumorigenesis.35 The ABO blood group genes are mapped to 9q region where genetic alterations are common in most cancers.36
Alternatively, others have proposed the idea that altered ABO glycosyltransferase or glycosylation pattern itself could be causative.35,37,38
Two genome-wide association studies have shown significant associations between the ABO locus and serum levels of both TNF-α and intercellular adhesion molecule-1, consistent with the association of inflammation and cancer. A secretory phenotype theory has also been suggested, which is more common in O blood type.35
Although the main objective of the present study was to unravel the relationship between ABO blood groups and Precancer and Oral cancer, we also considered the demographics of subjects under study. The number of subjects in the age category of 21-30 years was proportionately higher (32%)in the habit without lesion group. According to recent data by Grover S et al39, summarizing the findings of Global Adult Tobacco Survey -2 (GATS-2), in India, the overall mean age of initiation of tobacco use was 19.3 years.
Adolescence and early adulthood, i.e., 15 to 24 years, are considered to be in the most susceptible phase of life for initiation of tobacco use in India.40,41
Precancer and Oral cancer were more prevalent in age groups 41-50 years and 51-60 years respectively. Oral cancer incidence increases with age and a vast majority of cases reported are diagnosed between 50 to 60 years.41 This can be attributed to the indiscriminate usage of tobacco and tobacco-related products, over a prolonged period, leading to genetic damage.
Data on age-adjusted rates (AARs) of incidence of oral cancer presented by Sharma S et al.42 showed mouth cancer in the central region of India was maximum in the 70- to 75-year age group and that in northeast and west regions of India in 60- to 69-year age group. According to many researchers, most age groups showing precancer noted was 30 to 50years.43,44
Additionally, with sex-matched in the healthy group, subjects in the rest three groups were more likely to be males as compared to females. The same observation has been made by other authors also.45,46
This difference could be related to the difference in habit frequency between male and female individuals, diet, or other physiological factors. According to GATS, tobacco use in India has been higher among males than females.42,47,48 The present study exhibited a strong correlation between the presence of the chewing habit in all the precancerous lesions and oral cancer as compared to subjects in the habit without lesion group where smoking was more prevalent. A relatively lesser impact of smoking may be due to the indirect and relatively shorter duration of contact with tobacco in the oral cavity in comparison to the habit of tobacco chewing. It is possible that smoking and alcohol are greater risk factors in the presence of other habits such as chewing tobacco/pan masala but do not seriously affect the risk of oral lesions by themselves.46
Smokeless tobacco products use has been considered as the main component for the higher prevalence in South East Asia.41
41 India has one of the highest tobacco users in the world both in number and relative share.49 Smokeless tobacco is also highly addictive and causes cancer of the head and neck, oesophagus and pancreas, besides many oral diseases.50
It was observed that the most common precancerous lesion was Oral submucous fibrosis (50%) followed by leukoplakia (26%), lichen planus (16%) and combination lesion (8%). Similar findings were found in other related studies by Kumar S et al.48 and Singh N et al.51.
Several surveys have shown an increase in the incidence of OSMF attributed to the use of smokeless tobacco chiefly gutkha and paan masala, especially among youngsters.45 However Faiz et al.52 found Leukoplakia to be more prevalent than OSMF. The incidence of the death rate due to cancer has shown a sharp acceleration in the last 2 decades. Oral cancer is a lethal disease thus every way by which it can be curbed should be pondered. Advancements are required in techniques that can sort out individuals who tend to get cancer in presence of other risk factors and also differentiate patients with precancerous lesions who have a high risk of developing cancer so that occurrence of cancer can be averted.
Conclusion
Association of Blood group A
The authors of this study declared “No Conflict of interest”
Acknowledgement: Nil
Funding Information: Nil
Author Contribution:
Isha Gaurav: Proposed the Aim and Objective of the study, Planned the Protocol, Assessment of the results, Collection of the data, Submission of the paper
Vela Desai: Overall Supervision of the study, Critical Evaluation
Karamdeep Singh: Collection of the data, Laboratory Procedures
Satinder Singh: Statistical Analysis, table and Figures
Sukhmani Sanghera: Data Assessment, Written the manuscript
Anmol Kaur: Assistance in Sample collection, data collection, assistance in managing patients, writing
Alisha Madan: Reviewing the manuscript.
References:
-
Ram H, Sarkar J, Kumar H, Konwar R, Bhatt MLB ,Mohammad S. Oral Cancer: Risk Factors and Molecular Pathogenesis J Maxillofac Oral Surg 2011;10(2):132–137.
-
Miranda-Filho A, Bray F. Global patterns and trends in cancers of the lip, tongue and mouth. Oral Oncol 2020;102:104551.
-
Mathew B, Sankaranarayanan R, Sunilkumar KB, Kuruvila B, Pisani P. Reproducibility and Validity of Oral Visual Inspection by Trained Health Workers in the Detection of Oral Precancer and Cancer. British Journal of Cancer 1997;76(3):390–94.
-
Sreekumar VN. Global Scenario of Research in Oral Cancer J. Maxillofac. Oral Surg 2019;18(3):354–359.
-
Aird I, Bentall H.H., Roberts JAF. A relationship between cancer of the stomach and the ABO blood groups. Br Med J 1953;1(1):799-801.
-
Ben Q, Wang K, Yuan Y, Li Z. Pancreatic cancer incidence and outcome concerning ABO blood groups among Han Chinese patients: a case-control study. Int J Cancer 2011;128(5):1179-86.
-
Hirschfeld L, Hirszfeld H. Serological differences between the blood of different races. Lancet 1919;197:675-679.
-
Gupta P C, Ray CS, Sinha D N, Singh P K. Smokeless Tobacco: A Major Public Health Problem in the SEA Region: A Review. IJPH 2011;55(3):199–209.
-
Jaleel BF, Nagarajappa R. Relationship between ABO blood groups and oral cancer. Indian J Dent Res. 2012;23(1):7-10.
-
Jurel SK, Gupta DS, Singh RD, Singh M, Srivastava S. Genes and oral cancer. Indian J Hum Genet. 2014;20(1):4-9.
-
Rao MSS, Abraham TT. A retrospective study of blood groups in head and neck malignancies. J. Evid. Based Med Healthc. 2018;5(10):908-912.
-
Warnakulasuriya, S. Causes of oral cancer – an appraisal of controversies. Br Dent J. 2009;207:471–475.
-
Kumar M, Nanavati R, Modi TG, Dobariya C. Oral cancer: Etiology and risk factors: A review. J Cancer Res Ther. 2016;12(2):458-63.
-
Akhtar K, Mehdi G, Sherwani R, Sofi L. Relationship Between Various Cancers And ABO Blood Groups – A Northern India Experience. Int J Path. 2010;13(1)17-18.
-
Bhateja S, Arora G. ABO blood groups and oral premalignancies: A clinical study in selected Indian population. Indian J Cancer. 2014;51(3):219-221.
-
Behra R, Joshi YR. Distribution Of ABO Blood Group And Rh(D) Factor In Western Rajasthan. National J Med Research. 2013;3:1-3.
-
Dabelsten E, Pindborg JJ. Loss of epithelial blood group substance in oral carcinoma. Acta Path Microbial Scand. 1973;81:435-44.
-
Bryne M, Eide GE, Lilleng R, Langmark F, Thrane PS, Dabelsteen E. A multivariate study of the prognosis of oral squamous cell carcinomas. Are blood group and haemoglobin new prognostic factors? Cancer. 1991;68(9):1994-8.
-
Saxena S, Gupta KK, Meena P. Association of ABO Blood Groups about Oral Cavity Cancers in Western Rajasthan. IJCMR 2016;3(9);13-17.
-
Reddy VKG, Moon NJ, Sharma V, Guruprasad, Reddy EK, Chandralkala S.Is there an association between oral submucous fibrosis and ABO blood grouping? J Can Res Ther 2016;12(1):126
-
Shishodia NP, Anekar J, Raj AC, Jhugroo C, Divakar DD, Alshehri SZ, Alkalib Mana Ali M. Insight on the relationship of ABO blood grouping associated with oral premalignant lesions, conditions and inherited oral cancer syndromes. J Exp Ther Oncol. 2019;13(1):59-63.
-
Mortazavi H, Hajian S, Fadavi E, Sabour S, Baharvand M, Bakhtiari S. ABO blood groups in oral cancer: a first case-control study in a defined group of Iranian patients. Asian Pac J Cancer Prev. 2014;15(3):1415-8.
-
Byakodi J R, K Pushpanjali. Association Between ABO Rh Blood Groups and Oral Potentially Malignant Disorders. Adv Can Res and Ther. 2014;1(1):1-4.
-
Ramesh G, Katiyar A, Raj A, Kumar A, Nagarajappa R, Pandey A. Assessment of the relationship of ABO blood groups among tobacco-induced oral cancer patients of Kanpur Population, Uttar Pradesh. J Exp Ther Oncol 2017;12(2):129-135.
-
Singh K, Kote S, Patti B, Singla A, Singh S, Kundu H, Jain S. Relative Risk of Various Head and Neck Cancers among Different Blood Groups: An Analytical Study. J Clin Diagn Res 2014;8(4): ZC25-8.
-
Kakava K, Karelas I, Koutrafouris I, Damianidis S, Stampouloglou P, Papadakis G, Xenos A, Kania F, Saraf P, Tasopoulos G, Petridis N. Relationship between ABO blood groups and head and neck cancer among Greek patients JBUON 2016;21(3):594-596.
-
Jalili L, Zarabadipour M, Azmoudeh F, Esfahani M, Tamiz P. ABO Blood Group Distribution In Patients With Oral Squamous Cell Carcinoma. Annals of Dental Specialty 2018;6(2):11-16.
-
Raaghavan VM, Bailoor DN, Jhansirani P. Incidence of ABO Blood groups in oral cancer in south Kanara district. J Indian Dent Assoc 1986;58:305-8.
-
Garratty G. Blood groups and disease: a historical perspective. Transfus Med Rev 2000;14:291–301.
-
Garratty G. Relationship of blood groups to disease: do blood group antigens have a biological role?Rev Med Inst Mex Seguro Soc 2005;43 (Supl 1):113-12134.
-
Liumbruno GM and Franchini M. Beyond immunohematology: the role of the ABO blood group in human diseases. Blood Transfus 2013;11(4):491–499.
-
Oriol R, LePendu J, Mollicone R. Genetics of ABO, H, Lewis, X and related antigens. Vox Sang 1986;51:161-71.
-
Clausen H, Hakomori S. ABH and related host blood group antigens; immunochemical differences in carrier isotypes and their distribution. Vox Sang 1989;56:1-20.
-
Weisbrod AB, Nilubol N, Weinstein LS, Simonds WF, Libutti SK, Jensen RT, Marx SJ, Kebebew E. Association of type-O blood with neuroendocrine tumours in multiple endocrine neoplasia type 1. J Clin Endocr Metab 2013;98:109–114.
-
Henderson J, Seagrott V and Goldacre M. Ovarian cancer and ABO blood groups. J Epidemiol Comm Health 1993;47:287-9.
-
Dabelsteen E, Gao S. ABO blood-group antigens in oral cancer. J Dent Res 2005;84(1):21-8.
-
Franchini M, Liumbruno GM, Lippi G. The prognostic value of ABO blood group in cancer patients. Blood Transfus 2016;14(5):434-40.
-
Grover S, Anand T, Kishore J, Tripathy JP and Sinha DN. Tobacco Use Among the Youth in India: Evidence From Global Adult Tobacco Survey-2 (2016-2017). Tobacco Use Insights 2020;13:1–7.
-
Gupta, PC. Tobacco control in India. Indian J Med Res 2006;123:579-582.
-
Mahmood N, Hanif M, Ahmed A, Jamal Q, Saqib, Khan A. Impact of age at diagnosis on clinicopathological outcomes of oral squamous cell carcinoma patients. Pak J Med Sci. 2018;34(3):595–599.
-
Sharma S, Satyanarayana L, Asthana S, Shivalingesh KK, Goutham BS and Ramachandra S. Oral cancer statistics in India based on first report of 29 population-based cancer registries. J Oral Maxillofac Pathol 2018;22(1):18–26.
-
Saraswathi TR, Ranganathan K, Shanmugam S, Sowmya R, Narasimhan PD, Gunaseelan R. Prevalence of oral lesions about habits: Cross-sectional study in South India. Indian J Dent Res 2006;17:121-5.
-
Pindborg JJ. Frequency of oral submucous fibrosis in North India. Bull World Health Organ 1965;32:748-50.
-
Nair U, Bartsch H and Nair J. Alert for an epidemic of oral cancer due to use of the betel quid substitutes gutkha and pan masala: a review of agents and causative mechanisms. Mutagenesis 2004;19(4):251-262.
-
Gupta S, Singh R, Gupta OP and Tripathi A. Prevalence of oral cancer and pre-cancerous lesions and the association with numerous risk factors in North India: A hospital-based study Natl J Maxillofac Surg. 2014;5(2):142–148.
-
Franchini M, Liumbruno GM, Lippi G. The prognostic value of ABO blood group in cancer patients. Blood Transfus. 2016;14(5):434-40.
-
Kumar S, Debnath N, Ismail MB, Kumar A, Kumar A, Badiyani BK, Dubey PK, Sukhtankar LV. Prevalence and Risk Factors for Oral Potentially Malignant Disorders in Indian Population. Adv Prev Med. 2015;2015:208519.
-
Akansha Singh and Laishram Ladusingh.Prevalence and Determinants of Tobacco Use in India: Evidence from Recent Global Adult Tobacco Survey Data PLoS One 2014;9(12): e114073.
-
Moore SR, Johnson NW, Pierre AM, Wilson DF. The epidemiology of mouth cancer- A review of global incidence. Oral Dis. 2000;6:65-74.
-
Singh N, Singh D, Mishra N, Sharma AK. Prevalence of Potentially Malignant Disorders in Dental OPD at Tertiary Care Centre. Int J Med Res. 2019;4(6):97-101.
-
FAIZ, Syed Mohd. The spectrum of premalignant oral lesions in rural North Indian population at a tertiary care hospital. Int J Oral Health Sci.. 2018;4(6):1452-1457.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





