IJCRR - 13(20), October, 2021
Pages: 149-154
Date of Publication: 24-Oct-2021
Print Article
Download XML Download PDF
Knowledge and Practices About COVID-19 Pandemic in Pakistan
Author: Sikander Ghayas Khan, Bareera Saeed, Malik Muhammad Qasim, Atif Ikram, Hassan Sohail, Maria Shahzadi, Laiba Zahid, Ambreen Sadaf
Category: Healthcare
Abstract:Introduction: Coronavirus (COVID-19) illness, which has been labelled a pandemic, was caused by the year 2019. It was labeled a worldwide emergency on January 30th, 2020. Objective: To assess the knowledge and practices about the covid-19 pandemic in Pakistan Material and Methods: From April 1, 2021, to May 6, 2021, a cross-sectional online survey was performed. Residents of Punjab and Baluchistan, Pakistan, who were 18 or older male and female could read and understand English and Urdu who had completed the entire questionnaire were the subjects of the study. A structured close-ended online questionnaire based on expert opinions and literature was used to collect data. Software Statistical Package for Social Sciences (SPSS) version 21.0 was used to analyse the data. Results: The maximum number of the participants 330 (88.2%) were aware of the existence of coronavirus disease and there is no relationship between the categorical variables of gender (p= .144; p> .000). The majority of females 78 (20.8%) always, 72 (19.2%) often washed their hands with soap for twenty minutes significantly higher than males 52 (13.8%) 64 (17.0%) that indicates p< .001. Similarly, the majority of females used ordinary mask 94 (25.0%) always, 46 (12.2 %) often as compared to males 56 (14.3%); always, 59 (15.7) often and the majority of participants 345 (85.0%) were practising the general SOPs and value of p
Keywords: COVID-19, Coronavirus disease, Pandemic, perception, Knowledge, Awareness, Pakistan
Full Text:
Introduction
After the horrid waves that have encircled the entire world the COVID-19 pandemic affects the lives of every human. Everyone's life was impacted in every way by a new mysterious epidemic, which sparked the global emergency "COVID-19" pandemic. This COVID-19 pandemic was caused by an equivalent infective agent. Such viruses have conjointly caused outbreaks antecedently together with severe metabolism syndrome (SARS)-CoV and therefore the Middle East metabolism syndrome (MERS)-CoV. Coronavirus (COVID-19) eruption first arisen from the municipality of the urban centre, Wuhan, China in 2019. It’s a terrible kind of like its previous strain SARS-CoV that was well-known to cause a plague in 2002.1 Another strain MERS-CoV was 1st known in the Asian nation in 2012. COVID-19 is 1st known in urban centre, China then it unfolds to multiple countries and become a major danger for the world. On twenty-sixth February 2020, the primary cause of coronavirus emerges in Pakistan. Pakistan had 5038 confirmed COVID-19 cases and 86 deaths as of 12 April 2020. The highest number of cases were encountered (N=2425), followed by Sindh (N=1318), Khyber Pakhtunkhwa (N=696), Baluchistan (N=228). (N=216), Gilgit Baltistan (N=118) and Azad Jammu, Kashmir (N=35). All religious congregations and services have been suspended, marriage/banquet facilities are closed and all festivities have been cancelled. The full lock-down in the country has been put in. It was estimated that there were 13,328 COVID-19 cases across the country on 27 March 2020 (10,018 active cases, 281 deaths and 3029 recoveries).2
The predominant symptoms of this infective agent are health problem area unit fever and cough, however there's a variety of symptoms like dry cough, headache, fatigue, headache, diarrhea, fluid production, sym?t?m?ti?, lym?h??yt??eni?, and dyspnea are some of the most common symptoms of COVID-19 infection, whereas some patients could also be well.3 Patients were made a diagnosis with a painful respiratory disease that was later known as VID-19 infection.Till the last week of January 2020 almost 1975 patients were infected with coivd-19 virus in china. The incidence and prevalence found increased to 7734 in just five days, from January 30th to January 31st. Show how quickly the infection appeared.4 On the other hand the first infected person of covid 19 as case in the United States was registered on the 22nd of January 2020. 5 To date, there are 4,178,156 well-reported cases all over the world and the highest confirmed cases were reported in Italy, the United State of America, Spain and the United Kingdom.6 The infection of COVID-19 than a comrade in the nursing period is about to five days when these symptoms appear. 7 It takes approximately 6-41 days from the onset of symptoms to death to form a community of fourteen days.8
However, this period differs depending on the treatment plan and the patient's age. 9 China take strong and bold steps to control the pandemic. The success of that for the most part depends upon the public’s response towards the management measures that are taken. 10 In the Republic of Korea, measures were taken as early as three Jan 2020 well before the first confirmed case. On twenty-six February, the govt. opened first drive-through testing facility. The Republic of Korea took a pro-active approach to mass testing and active self-isolation. 11 Whereas within the United States of America (USA), timely steps weren't taken because of that range the amount the number of infected cases within the USA rose drastically and have become the country with the best number of confirmed cases within the world. in keeping with World Health Organization (WHO), the USA has confirmed cases of one,215,571 and 67,146 deaths.12
The case studies of China, the Republic of Korea and America showed that diseases police investigation pattern is connected with the behaviour of Governments and therefore the response of the overall public. The literature suggests that lack of awareness and incomprehension among Health Care workers (HCWs) leads to delayed diagnostics, disease spread and poor infection management practices. A systematic study on COVID-19 patients found that the groups most vulnerable were those with asthma, diabetes, cardiovascular and breathing systems.12 chronic blockade-related pulmonary disorders are fivefold higher risk of serious COVID-19. Poor awareness of the disease in the population is involved with a rise in the spread of infection and death rates, in particular high-risk groups.13 Therefore, controlling morbidity and mortality by COVID-19 effectively and minimizing it involves the shift in the behaviour of the general population, in particular high-risk classes, informed by people's awareness and expectations. Poor awareness of the disease in the population is involved with a rise in the spread of infection and death rates, in particular high-risk groups. Therefore, control and minimizing the morbidity of and mortality from COVID-19 successfully involves changing the behaviour of the general public, especially the high-risk groups, influenced by people's awareness and practice.14
Now, to contain the COVID-19 eruption in Pakistan, public understanding of the illness should be evaluated effective strategy might be created considering the public’s awareness relating to COVID-19 during this current study, the researcher investigated the data, knowledge and practices among Punjab and Baluchistan Pakistan residents relating to COVID-19 throughout the eruption. Therefore it is of the utmost importance, that the general public has good knowledge about each measurement (physical separation, proper hand hygiene, use of a facial mask, and breathing etiquette). The study was therefore conducted to evaluate among Pakistanis COVID-19 awareness, attitudes and preventive practices.15
Materials and Methods
The study design was observational cross-sectional and a convenient sampling technique was used to draw the sample from the population. Data was collected from April 01, 2020, to May 06, 2020, through an online google form link. Data was collected from different segments of society included labour class, businessmen, office workers, and other professionals from Punjab and Baluchistan. The age range was 18 to 65 years. A total of 374 participants were included in the study. The research was carried out in compliance with the Institutional Analysis Ethics (Ref No: IRB-UOL-FAHS/812/2021)and the Declaration. The study's goals, nature, and process were all described in the consent type. The secrecy and obscurity were highly maintained. A questionnaire and google form link was developed based on a close ended questionnaire with three sections relates to demographic information, questions based on knowledge attitudes and practices related to coronavirus. The questionnaire was developed with the reference of related published international content and with the suggestions of experts. Data was collected with in-person and online data collection strategies. The online link was sent to different segments of the population through WhatsApp, email and social media as the researcher itself collected the data from those who had no online access. Descriptive statistics (frequency, percentages, means, and standard deviations) and chi-square test was used
Results
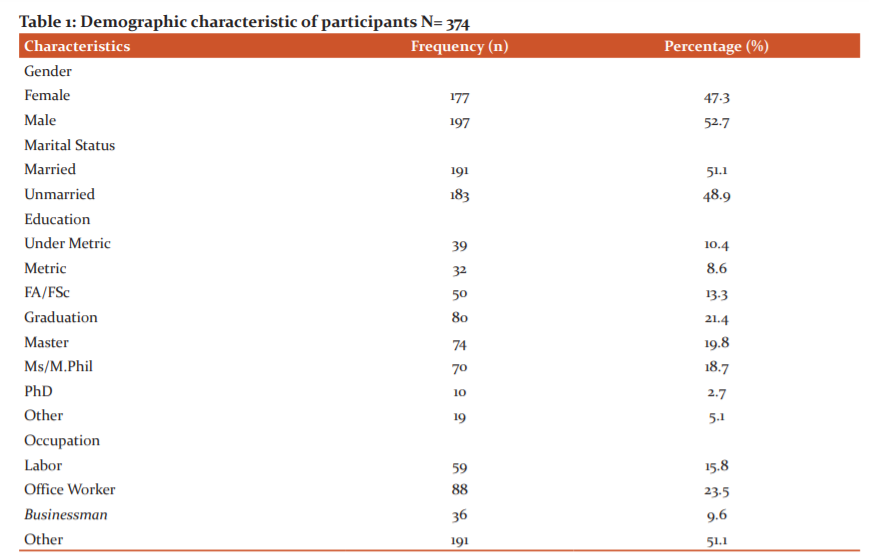
In this study, a total of 374 participants were included in the final analysis, of which 47.3% were female and 52.7% were male with an average age of 30.73±11.09 years (SD) ranging from 18 to 65 years.
Table 1 shows the socio-demographic information that was collected, including gender, age, education, occupation, marital status, and location of permanent residence. 51.1% of respondents were married, 48.9% were unmarried. The majority were respondents (21.3%), had a bachelor’s level of education (21.4%) were having master level and (19.8%) were having the postgraduate level of education. Participants included in this study were belongs to different occupations (23.5%) were office workers and (51.1%) were belongs to other domains of occupation.
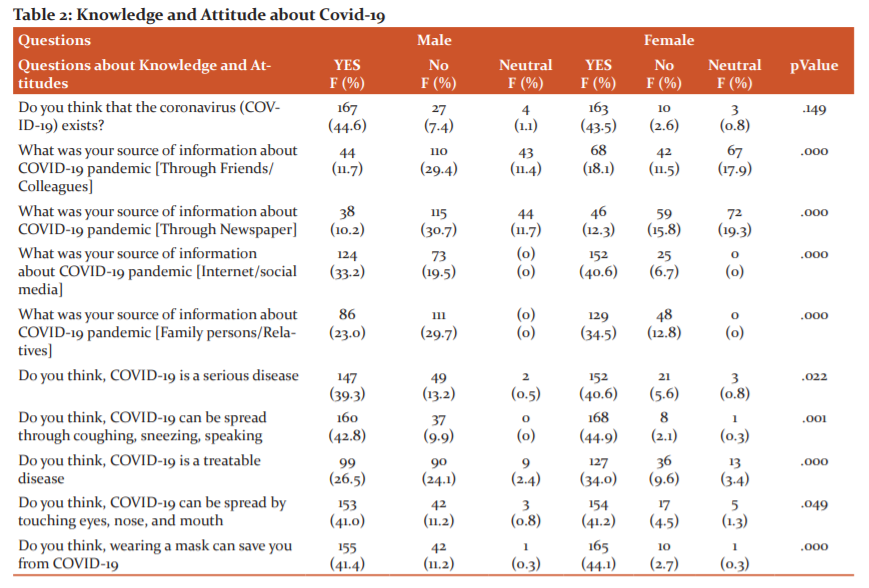
In the knowledge component, Table 2 depicts the findings. The maximum number of the male participants (167; 44.6%) than female ( 163; 43.5%) were aware regarding the existence of coronavirus disease and there is no relationship between the categorical variables of gender (p= .149), the majority of female participants acquired knowledge through social media (152; 40.6%) than male participants (124; 33.2%) the value of p = .000 that indicate significant relationship, almost (152; 40.6%, p=.022) female participants agreed to the fact that COVID-19 is a serious disease and can be transmitted and there is no significant association among male and female. The majority of female participants (168; 44.9%) had knowledge about factors of spreading and both genders had statistically significance (p=.001). The majority of Female Participants (127, 34.0%) considered statistically significantly (p=.000) that the covid 19 is a treatable disease. A gigantic amount of participants (female 154, 41.2%; male 153, 41.0% ), knew that COVID-19 infection can be by touching eyes, nose and mouth (p=.049). Almost all (female 165, 44.1%; male 155; 41.4%) of participants were having statistically significant knowledge about wearing the mask can protect from covid-19(p=.000).
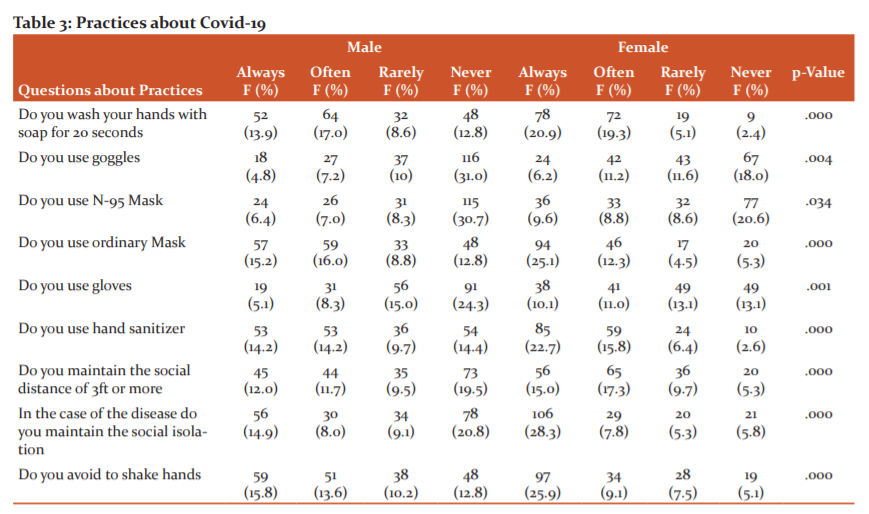
In table 3 for each question of practice, the Majority of females (20.9%; always, 19.3%; often) washed their hands with soap for twenty minutes significantly higher than males (13.9%, always; 17.0%; often) that indicates p< .000. Similarly, the majority of females used an ordinary mask (25.1%; always, 12.3% often) as compared to males (15.2%; always, 16.0%often) and p <.000 In the response of question to maintain the social distancing again females were significantly higher (15.0% always, 17.3% often) and value of p= .000 which indicates statistically significant. The majority of females (25.9% always, 9.1% often) avoided shaking hands and the value of p=.000.
Discussion
The results revealed that more than half of the participants were knowledgeable, while the rest were cautious. In comparison to conventional media such as newspapers, the web and social media are employed as the most prevalent sources of data. In Pakistan, the general public's preferred source of information regarding COVID-19 is social media (73.8 per cent). This can be explained by the fact that the majority of research participants were able to read, write, and use the internet. According to recent research done by the Pakistan Telecommunications Authority (PTA), 63 per cent of Pakistan's 76 million Internet users are under the age of 35.16
According to the findings, 88.2% of people (n = 330) had a true understanding of the environment, referrals, risk categories, and COVID-19 monitoring procedures. According to a research in Pakistan (64.8 per cent), Malaysian research17 (80.5 per cent), and Chinese research, this degree of outstanding knowledge is high (90 per cent).18 16 The majority of respondents acquired COVID-19-related material through social media, which explains a lot of the knowledge revealed during this study. However, this is frequently accompanied by a sense of irrationality, and so the use of social media to get information can explain the persistence of myths and disinformation in general culture.
The majority of female participants had good habits of taking cautious steps, according to the findings. This is typically the case, according to the findings of Zhong et al., who also said that the majority of participants (> 90%) used conservative measures.19 Government-sponsored efforts that identify the reasons, symptoms, and pathways might also be approximations of the high incidence of good manners used by just 50% of well-informed individuals, but these awareness initiatives are more focused on promoting preventative measures like facial expressions, social skipping, and hand hygiene practices.20
Continuous monitoring of the execution of preventative measures, a review of current initiatives, and therefore the renewal of such actions are all required to manage the epidemic. This study adds to the findings of earlier research in Pakistan by revealing the current status of awareness and practices measures taken.21 The study has several obvious shortcomings. First, because this is frequently an online survey design, the answer is heavily reliant on dependability and partially on the capacity to recall, making it less susceptible to memory bias. However, due to the community's policy of closure and termination, manual completion of the test was not possible. Second, because the sample size was insufficient, the bulk of respondents came from the province of Punjab and Baluchistan, limiting population availability across Pakistan.
Conclusion:
The participants from Punjab and Baluchistan have a better understanding of the COVID-19 and most of the participants are practising SOPs. However, more awareness is needed to improve the situation and stop the virus from spreading. These findings support the need for effective and targeted health education programmes that focus on COVID-19 information, resulting in a high level of positive attitudes and the adoption and maintenance of safe habits.
Acknowledgement:
I would like to say thank you to Professor Jamel for the English proofreading of this article.
Source of Funding:
This research was not funded.
Authors’ Contribution:
The idea of the study was Barrera Saeed and Muhammad Sikander Ghayas Khan, a Study designed by Muhammad Sikander Ghayas Khan, Write up, editing and data analysis done by Barrera Saeed, Data Collection from Baluchistan was done by Dr Malik Muhammad Qasim. Data Collection from Punjab done by Muhammad Sikander Ghayas Khan, Barrera Saeed, Hassan Sohail, Atif Ikram, Laiba Zahid, Ambreen Sadaf, Maria Shazadi, Barrera Saeed and Hassan Social entered the data on SPSS. Article Reviewed and final approval was made by Muhammad Sikander Ghayas Khan.
References:
1. Saunders-Hastings PR, Krewski D. Reviewing the history of pandemic influenza: understanding patterns of emergence and transmission. Pathogens. 2016;5(4):66.
2. Organization WH. Novel Coronavirus ( 2019-nCoV): situation report, 3. 2020.
3. McKibbin WJ, Fernando R. The global macroeconomic impacts of COVID-19: Seven scenarios. 2020.
4. Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int JEnviron Res PublicHealth. 2020;17(5):1729.
5. Van Bavel JJ, Boggio P, Capraro V, Cichocka A, Cikara M, Crockett M, et al. Using
social and behavioural science to support COVID-19 pandemic response. 2020.
6. Organization WH. Modes of transmission of the virus causing COVID-19: implications for IPC precaution recommendations: scientific brief, 27 March 2020: World Health Organization2020.
7. Surveillances V. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. China CDC Weekly. 2020;2(8):113-22.
8. Sun P, Lu X, Xu C, Sun W, Pan B. Understanding of COVID?19 based on current evidence. J Med Virol. 2020.
9. Wu JT, Leung K, Bushman M, Kishore N, Niehus R, de Salazar PM, et al. Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan, China. Nature Medicine. 2020:1-5.
10. Nesteruk I. Statistics based predictions of coronavirus 2019-nCoV spreading in mainland China. MedRxiv. 2020.
11. Chen X, Yu B. First two months of the 2019 Coronavirus Disease (COVID-19) epidemic in China: real-time surveillance and evaluation with a second derivative model. Global Health Research Policy. 2020;5(1):1-9.
12. Lin Q, Zhao S, Gao D, Lou Y, Yang S, Musa SS, et al. A conceptual model for the coronavirus disease 2019 (COVID-19) outbreak in Wuhan, China with individual reaction and governmental action. Int J Infect Dis. 2020;93:211-6.
13. Wang CJ, Ng CY, Brook RH. Response to COVID-19 in Taiwan: big data analytics, new technology, and proactive testing. Jama. 2020.
14. Cheng S-C, Chang Y-C, Chiang Y-LF, Chien Y-C, Cheng M, Yang C-H, et al. First case of Coronavirus Disease 2019 (COVID-19) pneumonia in Taiwan. J Formos Med Assoc. 2020.
15. Schwartz J, King C-C, Yen M-Y. Protecting health care workers during the COVID-19 coronavirus outbreak-Lessons from Taiwan's SARS response. Clin Infect Dis. 2020.
16. Organization WH. Coronavirus disease 2019 (COVID-19): situation report, 70. 2020.
17. Chiu A. Trump has no qualms about calling coronavirus the ‘Chinese Virus’. That's a dangerous attitude, experts say. The Washington Post. 2020;20.
18. Graham A, Cullen F, Pickett J, Jonson C, Haner M, Sloan M. Faith in Trump, Moral Foundations, and Social Distancing Defiance During the Coronavirus Pandemic. Moral Foundations, and Social Distancing Defiance During the Coronavirus Pandemic (April 22, 2020). 2020.
19. Jacoby SM. Return of the Repressed: Will the Coronavirus Bring a Great Transformation to America? Available at SSRN 3587048. 2020.
20. Burke RM. Active monitoring of persons exposed to patients with confirmed COVID-19—United States, January–February 2020. MMWR Morbidity and mortality weekly report. 2020;69.
21. Liu P, Beeler P, Chakrabarty RK. COVID-19 Progression Timeline and Effectiveness of Response-to-Spread Interventions across the United States. medRxiv. 2020
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





