IJCRR - 13(20), October, 2021
Pages: 119-123
Date of Publication: 24-Oct-2021
Print Article
Download XML Download PDF
Efficacy of Direct Posterior Class I Restorations Instigating \"Stamp Technique\": A Case Series
Author: Ashwini Bhangale, Nilima Ramdas Thosar, Sphurti Pramod Bane, Simran Das
Category: Healthcare
Abstract:The stamping technique is a simple method in restoring the non cavitated carious teeth with intact occlusal anatomy, in less chair-side time with perfection. This method has been appreciated to be precise and accurate to restore functional occlusion. This case report describes the esthetic restoration of non-cavitated caries by using an index to replicate its original anatomy.
Keywords: Stamp Technique, Class I restoration, Composite resin, Replication, Flowable stamp, Conservative dentistry
Full Text:
Introduction
Dentistry is forever witnessing the shift in materials and techniques about restoring posterior teeth. The use of dental amalgam has become obsolete in Pediatric Dentistry. The introduction of composite by Bowen in 1962 occurred due to the search for an ideal esthetic restorative material.1 However, experience and finesse are required when physically shaping a direct composite restoration. In indirect restorations, the contact, contour and occlusion are maintained in the laboratory while it is difficult to do so in a direct restoration intraorally.2Also, failure to achieve functional occlusion can cause an increase in the risk of stomatognathic musculature dysfunction.3
‘Stamp technique’ is a direct composite restorative procedure that was presented by Dr Waseem Riaz. Teeth that are non-extensively cavitated with occlusal morphology undisrupted are a clear indication for this technique. A negative replica is prepared first, termed as an index with either putty impression or flowable composite. This index is positioned and pressed firmly over the final incremental restorative layer to reproduce the original occlusal topography and reduced the time required for postoperative finishing.4 This case report primarily aims to confirm the Stamp technique’s efficacy using both putty impression material and micro brush embedded flowable composite.
Case Report 1
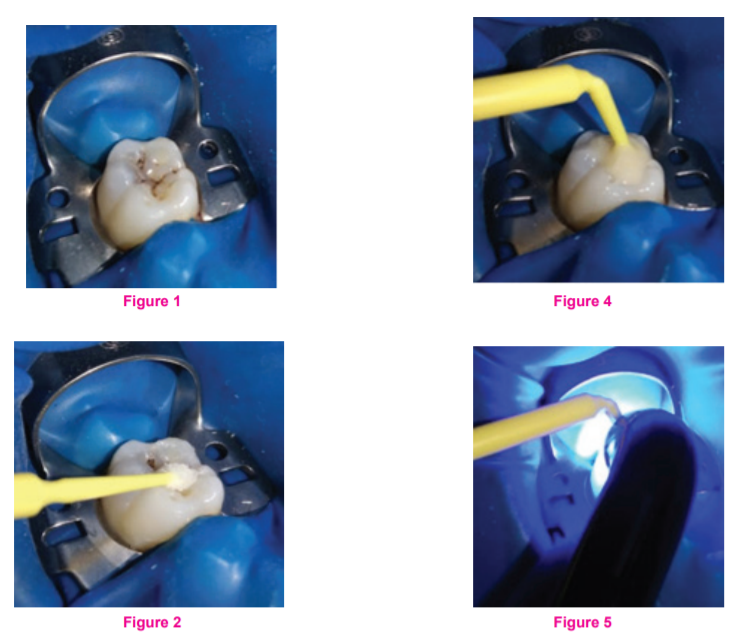
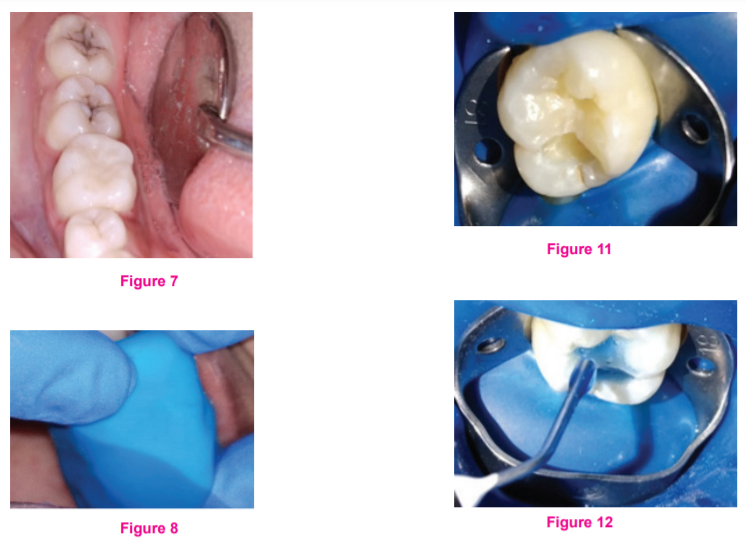
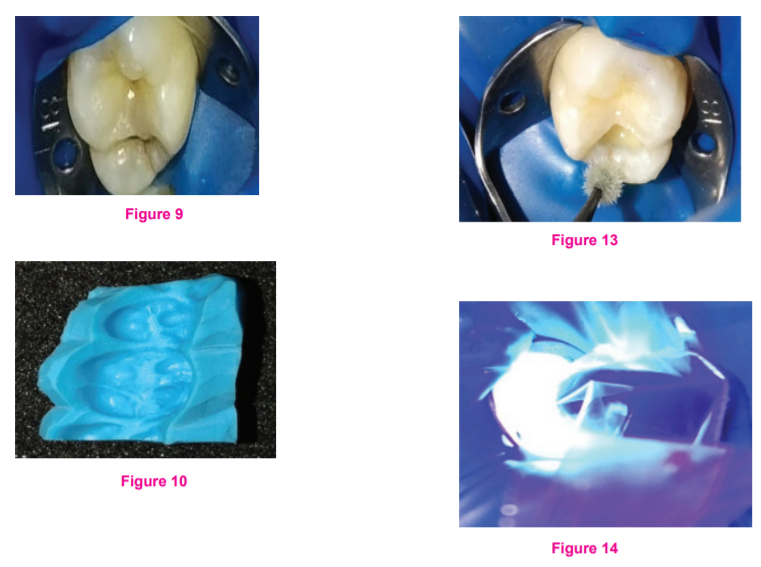
A 23-year-old female reported to the clinic with a chief complaint of blackish discolouration in the mandibular right first molar region accompanied by sensitivity to cold beverages’ consumption. In this case, the micro brush embedded flowable-composite technique was incorporated. Tooth isolation with a rubber dam was carried out to avoid contamination (Figure 1). The tooth of interest was then coated with a separating media (Figure 2). The flowable composite material was positioned sufficiently, covering the complete occlusal extent (Figure 3). A micro brush was decapitated for smooth conduct and implanted in the composite (Figure 4) and was then subjected to polymerization via light-curing (Figure 5). The attained index was detached from the tooth judiciously. Prophylaxis with pumice was done to remove the separating media. Cavity preparation was trailed by acid-etching with 37% orthophosphoric acid for 30 seconds (Figure 6) and rinsed off with water. The tooth was air-dried with an air spray and checked for the characteristic frosty appearance. The bonding agent was smeared with the applicator tip, and curing was done for 20 seconds (Figure 7). The restoration was accomplished in increments to support adequate and precise curing of the composite. Subsequently, the last incremental layer was placed; Teflon tape was sandwiched between the index and the composite layer, and the index was then gently placed over (Figure 8). The Teflon tape was removed carefully, and excessive material was wiped off without disrupting the stamped surface preceding the curing. The occlusion was checked with the bite paper, and restoration was subjected to final polishing on remarkably fewer marks (Figure 9, 10).
Case Report 2
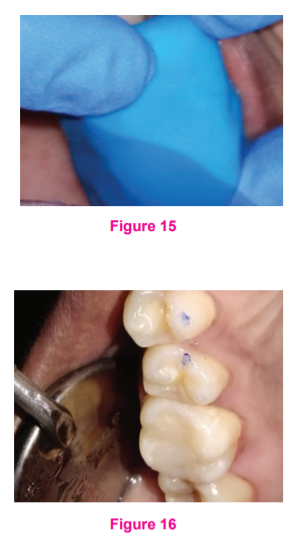
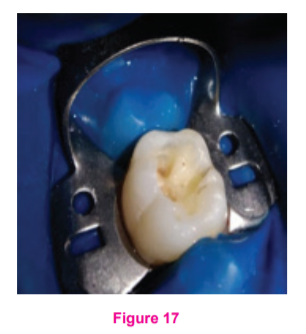
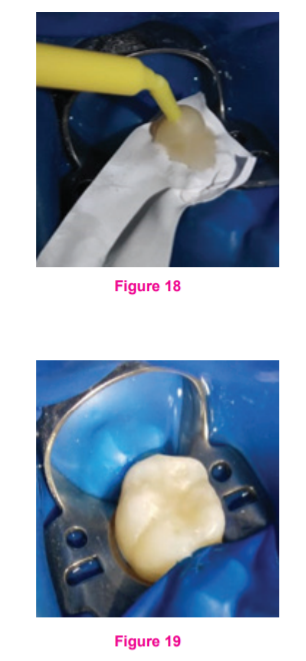
A 26-year-old male reported to the clinic with a chief complaint of sensitivity in the right maxillary right first molar region. The putty Stamp technique was used in this patient. The tooth of interest was then cleaned prophylactically with pumice to remove debris. First, the light body and heavy body putty impression material was mixed evenly and then placed over the tooth of interest (Figure11). After the material’s setting, it was removed, and the index was modified by trimming it to the cervical level for its better placement (Figure 12). Later the tooth was isolated with a rubber dam (Figure 13). The cavity preparation (Figure 14) was done and acid-etching with 37% orthophosphoric acid for 30 seconds, followed by thorough rinsing with water spray (Figure 15). The tooth was air-dried with an air spray and checked for its distinctive frosty appearance. The bonding agent was smeared with the applicator tip (Figure 16) and was Light-cured for 20 seconds (Figure 17). The restoration was accomplished in increments to support adequate and precise curing of the composite. The putty stamp was placed firmly on the last incremental layer, the excessive material was wiped out with the instruments, and restoration was cured (Figure 18). The final restoration was checked for its high points with a bite paper and polished with pumice (Figure 19).
Discussion
The pit and fissures are the prime retentive areas for the amassing of the substrate and hence is one of the culprits accountable for caries. The molars and premolars are more prone to the pit and fissure caries owing to their occlusal morphology. Molars are the first teeth to be affected by caries. Maxillary molars are more affected than the mandibular molars as suggested by Demirci M et al.5 Maxillary molars are difficult to restore in indirect vision and require experience to carve out the grooves, fissures, and oblique ridge to imitate the morphology. For composite restoration, isolation may be difficult to attain in mandibular molars in hyper-salivating patients. Pit fissure caries superficially appears to be limited to the enamel but as the cavity preparation is progressed to obtain an infection-free dentin a substantial amount of enamel has already been excavated. Restoring the cavity and an excellent cusp-fossa relationship, aesthetics, and overall harmony can be time-consuming. Hence, the Stamp technique has been utilized. Though many dental professionals may not use it, it is undoubtedly an appreciable technique that can be integrated.
As per the author’s experience with this technique, the apparent advantage is feasibility and condensed time-span required for the restoration and the post-restoration adjustment for achieving accordance between the occlusion and aesthetics with flowable composite as the Putty index. Additionally, the reduction of voids is achievable since the stamp is pressed upon the final layer, which aids in its drastic eradication while restoring.6 This technique may be comfortable however, the disadvantage can be that it demands accuracy of performance and the proper placement of the stamp for getting noticeable results which is the prime motive. This can be overcome merely with regular rehearsal. Alternative dental materials that can be utilized for the stamp are Bite-wax, Pit-fissure sealant, Gingival dam, and Clear Poly-methylmethacrylate. 7
Conclusion
The Stamp technique is a boon to aesthetic dentistry. It is efficient indirect composite restoration and can competently benefit in replicating the occlusal topography, which is difficult to achieve with manual carving. This technique could be carried out using varied materials that can adapt to the function of a Stamp.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of Interest: There are no conflicts of interest.
Source of funding: Nil

References:
-
Agrawal A, Manwar NU, Hegde SG, et al. Comparative Evaluation of Surface Hardness and Depth of Cure of Siloraneand Methacrylate-Based Posterior Composite Resins: An in Vitro Study. J Conserv Dent.2015;18(2):136–39.
-
Modi R, Gogiya R, Chandak M, Bhutda P.Stamp technique - a new perspective for composite resin restoration: A case report.IJCR. 2018;10(07):71406-71408.
-
Dawson EP. Evaluation, diagnosis and treatment of occlusal problems. 2nd Ed. C.V. Mosby Co. (Toronto); 1989
-
Murashkin A. Direct posterior composite restorations using stamp technique-conventional and modified: A case series. International Journal of Dentistry Research. 2017;2(1):3-7
-
Demirci M, Tuncer S, Yuceokur AA. Prevalence of caries on individual tooth surfaces and its distribution by age and gender in university clinic patients. Eur J Dent. 2010;4(3):270-279.
-
Pompeu JGF, Morais RC, Ferreira TO, et al. Occlusal Stamp Technique For Direct Resin Composite Restoration: A Clinical Case Report. Int J Recent Sci Res.2016; 7(7):12427-12430.
-
Mary G, Jayadevan A. Microbrush stamp technique to achieve occlusal topography for composite resin restorations – A technical report. J Sci Dent 2016;6.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





