IJCRR - 13(20), October, 2021
Pages: 107-112
Date of Publication: 24-Oct-2021
Print Article
Download XML Download PDF
Correlation of High-density Lipoprotein (HDLc) with Acute Phase Reactants in COVID-19 Patients: An Observational Study in a Tertiary Care Hospital West Bengal
Author: Samadder Sangita, Datta Priyanka, Chakraborty Sandip, Ghosh Chinmoy
Category: Healthcare
Abstract:Introduction: Dyslipidemia plays an important role in the pathogenesis and evolution of critical illness, but limited information exists regarding the lipid metabolism of severe coronavirus disease 2019 (COVID-19) patients in India. Patients with COVID-19 feature hyper inflammation, suffer multiple organ dysfunctions, though if these patients develop dyslipidemia or not are unknown. Aim & Objective: We aimed to investigate if there is any correlation between high-density lipoprotein cholesterol (HDL-c) with serum C-reactive protein (CRP), D-Dimer, and serum ferritin in COVID-19 patients of West Bengal. Methodology: Sixty two patients with COVID-19 detected by RT-PCR admitted in General Medicine isolation ward and COVID block between 19th October and 10th December 2020 of a tertiary care teaching hospital was selected by semi-purposive sampling. Results: There were 40.3% patients in mild, 30.6% in moderate and 29% in the severe category. An increased level of D-dimer 1.4 IQR (0.64,3.27) \?g/ml was found in patients with severe disease compared with mild group. Serum ferritin in the severe COVID-19 group was higher than in the mild COVID-19 group (485.6 ng/ml IQR(227.7-798.2)] vs 150.3ng/ml IQR(56.4-249.7). Compared with mild patients, severe COVID-19 patients presented with low HDL-C [median, 48 vs 38.3 P = 0.04] which suggested that low HDL-C may be correlated with the severity of COVID-19 patients. Conclusion: We concluded that low HDLc was associated with the inflammatory response. The hypolipidemia in COVID-19 patients would raise an urgent awareness to clinical physicians in the frontline against this global pandemic.
Keywords: COVID-19, CRP, D Dimer, Ferritin, HDL-C, Acute phase reactant, ARDS, RT-PCR, Heam oxygenase, SpO2
Full Text:
Introduction :
Coronavirus disease-2019 (COVID-19) is an emerging infectious disease that has been declared a global public health emergency by the World Health Organization (WHO).1 the global COVID-19 pandemic caused by severe acute respiratory syndrome coronavirus(SARS-CoV-2) has severely affected India. 2 Most of patients with COVID-19 have mild illness or maybe asymptomatic, about 5-10% of patients develop severe pneumonia, acute respiratory distress syndrome (ARDS), multi-organ failure eventually die.2 Why some individuals become critically ill, while others do not with COVID 19 infection, remains an unsolved puzzle. The majority of patients with COVID-19 were mild in the first few days, few progressed rapidly to acute respiratory failure, metabolic acidosis, septic shock, ARDS.
Early identification of risk factors for critical patients could facilitate appropriate supportive care and that may reduce mortality.3 A study with 138 laboratory-confirmed cases with COVID-19 showed the changes of the neutrophil count, lymphocyte count, and D-dimer levels. 4 Inflammations -related indicators were found higher in patients with COVID-19, like erythrocyte sedimentation rate (ESR), interleukin-6 and C-reactive protein (CRP)
Laboratory markers and radiological changes, Comorbidities have been proposed for risk stratification.5,6 There is evidence that elevated serum C-reactive protein (CRP), procalcitonin (PCT), D-dimer, and hyperferritinemia are found in critical patients. These findings suggest there might be a role of cytokine storm in COVID-19 pathophysiology.7Dyslipidemia associated with SARS has been reported, although rarely. There was a report showing a lower level of total cholesterol (TC) in SARS patients as compared with healthy subjects.8 The report indicate that patients with coronavirus-related diseases may develop dyslipidemia but have been underrated.
Laboratory biomarkers can identify the severity of COVID-19. That’s is needed as resource allocation must be carefully planned, especially in the context of respiratory support, critical patient management.
In this study, we measured HDLc, serum C-reactive protein (CRP), D-dimer, and serum ferritin ) in COVID-19 patients. We aimed to investigate if there is any correlation between high-density lipoprotein cholesterol (HDL-c) with acute phase recant like serum C-reactive protein (CRP), D-dimer, and serum ferritin ) in COVID-19 patients
Materials and methods
Study design and participants
The present work was a single-centre, hospital-based study, conducted at Nil Ratan Sircar Medical College and Hospital, Kolkata which is a tertiary care teaching hospital, done between 19th October to 10th December 2020. The project was approved by the Institutional Ethical Committee. During the study, the status of the hospital changed from Level 2 (eligible to treat symptomatic patients with suspicion of COVID-19, but after confirmation of the diagnosis, the patients are to be transferred to Designated COVID Care Centre) to Level 4 (eligible to treat seriously symptomatic patients suffering from COVID-19). Patients admitted to the general Medicine isolation ward of N.R.S Medical College and Hospital and subsequently diagnosed as COVID-19 by reverse transcriptase-polymerase chain reaction (RT-PCR) from the oral and nasopharyngeal swab, and patients admitted directly to COVID block after diagnosis were selected by semi-purposive sampling. Total of 62 patients were included in this study. A “confirmed case” was defined as “A person with laboratory confirmation of COVID-19 infection by reverse transcriptase-polymerase chain reaction(RT-PCR), irrespective of clinical signs and symptoms”. Written, informed consent was taken from all of the patients.
The blood for detecting serum lipid concentration, blood samples were collected from each subject after at least 12 h of overnight fasting. For avoiding the interference of treatment to serum lipid concentration samples were drawn at admission, before starting definitive treatment and were tested at our central laboratory and department of Biochemistry. “Mild disease” was defined as fever with malaise or mild cough, but no shortness of breath. “Moderate disease” was defined in adults as the presence of dyspnoea with a respiratory rate of more than 24/min or SpO2 between 90 and 94% in room air, pneumonia not fulfilling the criteria of “severe” disease or presence of altered liver or renal function tests. Severe disease was defined as the presence of severe dyspnoea with a respiratory rate of more than 30/min or SpO2 less than 90% in room air, presence of ARDS, severe sepsis or septic shock.9,10
Serum Ferritin was tested in ADVIA Centaur XP immunoassay systems by chemiluminescent detection. D-dimer was tested in Stago-STA Compact Max Coagulometer from citrated plasma. CRP was tested by the immunoturbidimetry method. Serum HDL were measured in the Transasia instrument.
INCLUSION CRITERIA
1. Confirmed cases of COVID 19 (RT-PCR) patients admitted in General Medicine isolation ward, and COVID block 1 of NRS Medical College and Hospital, Kolkata
2. Aged 18 years or older
EXCLUSION CRITERIA:
-
Patients who had received glucocorticoids before coming to our hospital
-
HIV infected patients
-
Diagnosed patients with acute or chronic liver disease
-
Known Diabetic patients and on anti-diabetic medications
This study was approved by the institutional ethics board of our institute.
The clinical classifications are (1) mild, patients with minor symptoms and imaging showed no pneumonia.
(2) Moderate, patients with fever, symptoms of chest infection and imaging shows pneumonia.
(3) severe, patients have any of these a) respiratory distress, respiratory rate ≥ 30 beats/min; b) in resting condition, SpO2 ≤ 93%; c) arterial blood oxygen partial pressure/oxygen concentration ≤ 300 mmHg (1 mmHg = 0.133 kPa); d) pulmonary imaging shows lesion progressed more than 50% within 24–48 h.
(4) Critical patients, one of the following conditions: a) respiratory failure occurs and requires mechanical ventilation; b) Shock c) ICU admission is required for combined organ failure.
In this study, the patients with mild or moderate symptoms were included and the patients with severe or critical symptoms were classified as severe/critical group. The assessment of disease severity and laboratory tests were performed at the same time on the day of inpatient admission before treatment
STATISTICAL ANALYSIS
Data were entered in Microsoft Excel spreadsheet Continuous variables were expressed as median (interquartile range, Bivariate correlation analysis (Pearson correlation) was performed for analyzing the correlation of serum lipid concentration and other laboratory parameters. p< 0.05 was considered statistically significant.
Statistical analyses were performed using the SPSS 17. Institutional ethical clearance number : NMC : 6087, 16.10.2020
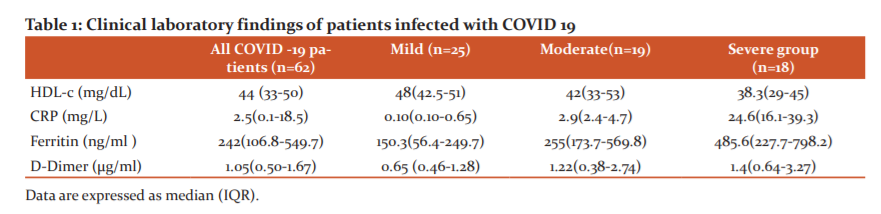
RESULTS: Among sixty-two patients, there was 33 male 29 female. There were 25 patients (40.3%) in the mild group, 19 patients (30.6%) in the moderate group and 18 patients (29%) in the severe group. The median age was 59.0 years (IQR 45.0–70.0). The most common symptoms at disease onset were fever (78.6%) and cough followed by shortness of breath. We observed substantial differences in the clinical and laboratory findings between the groups of patients. Table 1 shows Clinical laboratory findings of patients infected with SARS-COVID 19.
From the table, we can see patients with severe disease were significantly more likely to exhibit dysregulated coagulation function. An increased level of D-dimer 1.4 IQR (0.64,3.27) μg/ml was found in patients with severe disease compared with the mild group. HDL-c levels decreased significantly in severe cases as compared with levels in mild cases (p = 0.004). Compared to both moderate and severe patients, showed a significant increase in serum concentrations of C-reactive protein during hospitalization. Patients with severe disease courses had a far elevated level of CRP than mild or moderate patients. Our study reported patients with severe symptoms had a CRP concentration of 24.6 IQR(16.1-39.3)mg/L and patients with mild symptoms CRP concentration of 0.10 IQR(0.10-0.65) mg/L. In our study with 62 COVID-19 patients, it was found that individuals with moderate and severe COVID-19 exhibited increased serum ferritin level, being serum ferritin in the severe COVID-19 group significantly higher p<0.001 than in the mild COVID-19 group (485.6 ng/ml IQR(227.7-798.2)] vs 150.3ng/ml IQR(56.4-249.7)respectively.
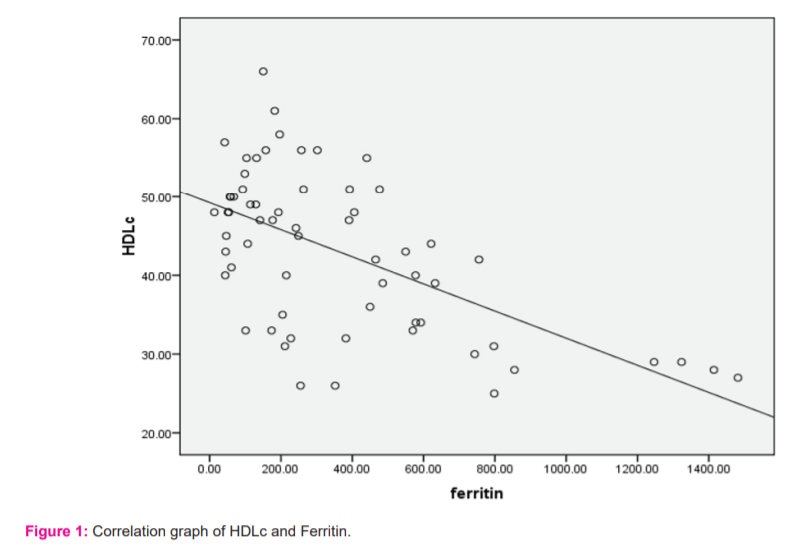
Compared with mild patients, severe COVID-19 patients presented lower levels of HDL-C [median, 48 vs 38.3 p= 0.04] which suggested that low HDL-C may be correlated with the severity of COVID-19patients. Therefore, the effect of HDL-C level on COVID-19 was further analyzed.
From fig 1 we can see There was a negative correlation between serum HDL-C and serum ferritin r = -0.6. Figure 1 shows how HDLc decreases with increasing ferritin.
Discussion
Despite world efforts to decrease COVID-19 cases since 2019, single-day confirmed cases are on the increase till now.11 Moreover, until currently no specific drug presently obtainable for COVID-19. Vaccines trials are going on all over the world. The progression to severe illness results in high rates of mortality (40%) in patients. 12Timely intervention and control of disease progression are important for the prevention and control of COVID-19. Though the clinical and epidemiological features of this disease have been reported. 13,14,15 Few studies have focused on the risk factors for the development of severe disease in patients with COVID-19, particularly supported laboratory knowledge.
Many potential hypotheses may justify the dynamic changes during COVID-19. Firstly, the Liver plays an important role in lipid metabolism, and liver dysfunction caused by SARS-CoV2 infection. It was reported that 14%-53% of patients with COVID-19 had hepatic dysfunction, especially in those severe and critical patients. 16
High-density lipoproteins (HDLs) are a family of particles characterized by their ability to transport cholesterol from extrahepatic tissues to the liver for metabolism. The primary role of HDLs is anti-atherosclerosis. 17 however several recent studies have found multiple characteristics of HDLs, including anti-infection, anti-inflammatory, anti-apoptotic or antioxidant functions. 18,19Furthermore HDLs is believed to play a protecting role in several infectious diseases. It had been discovered that patients with low levels of HDLs showed an increased risk of infection and a worse outcome. 20,21,22 Therefore, it had been assumed that HDL levels may be associated with the prognosis of COVID-19 patients.
The synthesis of apolipoproteins and lipoproteins would be affected by the hepatic dysfunction of patients with severe COVID19. Secondly, an acute inflammation caused by SARS-CoV-2 might alter lipid metabolism as well. In our study, we found that HDL-C were closely related to C Reactive Protein, which could partially justify the hypolipidemia was associated with the inflammatory response in severe COVID-19 patients.
Finally, a very recent study has shown that a rare missense variant in the cholesteryl ester transfer protein gene (CETP, rs1800777-A) was associated with a marked reduction in HDL-C levels and adverse clinical outcomes during sepsis. COVID-19 patients who carry the A allele may have lower HDL levels and worse prognoses compared with non-carriers.23Therefore, the genetic variation of CETP gene is a key regulator of HDL-C levels and clinical prognosis during sepsis. At present, the genetic variation of CETP gene in patients with COVID-19 has not been reported, and it should be a promising research direction in the treatment and evaluation of prognosis among patients with COVID19. Since COVID-19 is a global pandemic with a high mortality rate.
Since COVID-19 is a global pandemic with a high mortality rate, it will be helpful to determine several early markers to predict the disease severity and prognosis of COVID-19. The elevated level of CRP could be a valuable marker to predict the possibility of aggravation of non-severe COVID-19 patients, which may help health care workers to identify those patients at an early stage for early treatment.24
Ferritin is one of the mediators of immune dysregulation, mostly in extreme hyperferritinemia, via direct immune-suppressive and pro-inflammatory effects, it contributes to the cytokine storm. Fatal outcomes of COVID-19 are seen after the cytokine storm syndrome. Individuals with diabetes shows increased serum ferritin levels, these patients have a higher probability to get serious complications from COVID-19. Evidence supporting the hypothesis that ferritin levels might be a crucial factor influencing the severity of COVID-19 Chen et al. analyzed the clinical characteristics of 99 patients, in which 63 of them had high serum ferritin. Elevated ferritin levels were found also in autopsies of 12 patients whose cause of death was SARS-CoV-2 infection. 25 Therefore we can conclude elevated ferritin is linked with disease severity.
The breakdown product of damaged haem stimulates signals for the synthesis of new haem. Heam, steroids and heam oxygenase -1 (HO-1 or HSP32) induce hepatic aminolevulinic acid synthase (ALAS1) activity, the rate-limiting step of heam synthesis. Haem is degraded by HO (gene Hmox1/Hmox2), producing ferrous iron, biliverdin and carbon monoxide, resulting in increased plasma ferritin and bilirubin. These markers are significantly elevated in COVID-19 patients with poor prognoses.26Haem breakdown by HO produces endogenous carbon monoxide, which has a higher affinity for binding with haemoglobin compared to oxygen. This might result in a decreased oxygen saturation capacity. Chances of having deep vein thrombosis increase significantly with elevated carbon monoxide concentrations, increasing the risk of pulmonary emboli and acute coronary syndrome.27,28 Hyperinsulinaemia is one of the components in the pathogenesis of obesity, CVD, T2DM, hypertension, increased haem oxidation, haem breakdown, endogenous carbon monoxide production and resultant increased thrombi risk. D-dimer was found to be markedly elevated in patients with COVID-19 it is a direct marker for fibrinolytic and coagulation activity.29,30 Patients with COVID-19 who have a high risk of venous thromboembolisms suffer poorer outcomes Hu et al. observed that HDL level was significantly lower in the patients with COVID-19 primary infection than secondary infection patients similar to our study.31
Fan et al. analysed the serum lipid levels of 21 patients before they were infected by COVID-19 and during their entire courses of the disease. They observed that the Low-density lipoprotein and High-density lipoprotein levels in all patients showed significant decreases at the time of admission as compared to the levels before infection. 32
From our study we got HDL levels showed a significant decrease in COVID 19 patients.
Conclusion: From our study we conclude, low HDLc is associated with inflammatory response and disease severity of COVID-19. Whether HDL-based therapies have potential therapeutic effects on patients with severe COVID-19 deserves further exploration. Laboratory findings in patients with severe COVID-19 had elevated inflammatory markers, including CRP, ferritin, which has been associated with critical illness could be an early predictor of severity.
Declarations
Study Limitations
Our study had few limitations. Firstly, this study was an observational study with a relatively small sample size, a large cohort study would be required to further confirm our conclusion. Secondly, asymptomatic patients and those with mild symptoms were not be enrolled, thus the conclusions drew by the study might not apply to asymptomatic patients. Thirdly, a large number of factors could affect the lipid metabolism in COVID-19, the specific mechanism about dyslipidemia could not be concluded, and would be required further powerful investigation.
Acknowledgements
We would like to express our greatest gratitude to the people who have helped and supported us throughout our project. We are grateful to the Principal and Dean of Nil Ratan Sircar Medical College, Kolkata for providing the facilities for conducting the study.
Funding source: Institute Academic Fund
Competing Interests
There are no conflicts of interests
Individual contribution: Dr. Ghosh Chinmoy and Dr Datta Priyanka experimented. Dr Samadder Sangita and Dr Datta Priyanka wrote the manuscript with support from Dr Chakraborty Sandip. Dr. Ghosh Chinmoy helped supervise the project. Dr Chakraborty Sandip and Dr Samadder Sangita conceived the original idea. Dr Chakraborty Sandip supervised the project.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Bhandari S, Bhargava A, Sharma S, Keshwani P, Sharma R, Banerjee S . Clinical profile of COVID-19 infected patients admitted in a tertiary care hospital in North India. J Assoc Phys India.2020; 68:13–17
2. Chen N, Zhou M, Dong X. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020; 395: 507–513.
3. Gupta N, Praharaj I, Bhatnagar T, Thangaraj JWV, Giri S, Chauhan H et al. ICMR COVID Team (2020) Severe acute respiratory illness surveillance for coronavirus disease 2019, India. Indian J Med Res. 151:236–240
4. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, Wang B, Xiang H, Cheng Z, Xiong Y, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020
5. Pranata R, Huang I, Lim MA,. Impact of cerebrovascular and cardiovascular diseases on mortality and severity of COVID-19 – a systematic review, meta-analysis, and meta-regression. J Stroke Cerebrovasc Dis 2020; 29: 104949.
6. Huang I, Pranata R. Lymphopenia in severe coronavirus disease-2019 (COVID-19): systematic review and meta-analysis. J Intensive Care. 2020; 8: 36.
7. Mehta P, McAuley DF, Brown M. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020; 395: 1033–1034
8. Cao X, Yin R, Albrecht H, Fan D, Tan W. Cholesterol: a new game player accelerating vasculopathy caused by SARS-CoV-2? Am J Physiol Endocrinol Metab. 2020;319:E197–e202.
9. “Management protocol for COVID-19, second edition”, Government of West Bengal, Department of Health and Family Welfare. [Internet].Available from: www.wbhealth.gov.in
10. “Clinical Management Protocol: COVID-19” Government of India, Ministry of Health and Family Welfare, Director General of Health Services, (EMR division)Version 3. 13.06.2020[Internet]. Available from: www.mohfw.gov.in
11. Shereen M.A., Khan S., Kazmi A. COVID-19 infection: Origin, transmission, and characteristics of human coronaviruses. J Adv Res. 2020; 24:91–98.
12. Wiersinga W.J., Rhodes A., Cheng A.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. J Am Med Ass. 2020
13. Tu H., Tu S., Gao S., Shao A., Sheng J. Current epidemiological and clinical features of COVID-19; a global perspective from China J Infect. 2020;81(1):1–9.
14. Zheng Y., Xu H., Yang M. Epidemiological characteristics and clinical features of 32 critical and 67 noncritical cases of COVID-19 in Chengdu. J Clin Virol. 2020;127
15. Shen Y., Zheng F., Sun D. Epidemiology and clinical course of COVID-19 in Shanghai, China. Emerg. Microbes Infect. 2020;9(1):1537–1545.
16. Jothimani D, Venugopal R, Abedin MF, Kaliamoorthy I, Rela M: COVID-19 and Liver. J HEPATOL 2020.
17. Wei X, Zeng W, Su J, Wan H, Yu X, Cao X, et al. Hypolipidemia is associated with the severity of COVID-19. J Clin Lipidol. 2020;14:297–304.
18. Gaw A. HDL-C and triglyceride levels: relationship to coronary heart disease and treatment with statins. Cardiovasc Drugs Ther. 2003;17:53–62.
19. Tran-Dinh A, Diallo D, Delbosc S, Varela-Perez LM, Dang QB, Lapergue B, et al. HDL and endothelial protection. Br J Pharmacol. 2013;169:493–511.
20.Tanaka S, Couret D, Tran-Dinh A, Duranteau J, Montravers P, Schwendeman A, et al. High-density lipoproteins during sepsis: from bench to bedside. Crit Care. 2020;24:134.
21.Santos-Gallego CG, Badimon JJ, Rosenson RS. Beginning to understand high-density lipoproteins. Endocrinol Metab Clin N Am. 2014;43:913–47.
22.Madsen CM, Varbo A, Tybjaerg-Hansen A, Frikke-Schmidt R, Nordestgaard BG. U-shaped relationship of HDL and risk of infectious disease: two prospective population-based cohort studies. Eur Heart J. 2018;39:1181–90.
23. Trinder M, Genga KR, Kong HJ, Blauw LL: Cholesteryl Ester Transfer Protein Inuences High-Density Lipoprotein Levels and Survival in Sepsis. Am J Respir Crit Care Med. 2019, 199(7):854-862
24. Young BE, Ong SWX, Kalimuddin S,. Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore.JAMA. 2020;323(15):1488-1494.
25. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020; 395(10223):507–13.
26.Bonetti G, Manelli F, Patroni A,. Laboratory predictors of death from coronavirus disease 2019 (COVID?19) in the area of Valcamonica, Italy. Clin Chem Lab Med. 2020; 58(7): 1100– 1105
27. Al?Samkari H, Karp Leaf RS, Dzik WH,. COVID?19 and coagulation: bleeding and thrombotic manifestations of SARS?CoV?2 infection. Blood. 2020; 136: 489? 500
28.Lippi G, Plebani M (2020) The critical role of laboratory medicine during coronavirus disease 2019 (COVID-19) and other viral outbreaks. Clin Chem Lab Med. 58(7):1063–1069
29. Mehra MR, Desai SS, Kuy S, Henry TD, Patel AN (2020) Cardiovascular disease, drug therapy, and mortality in COVID-19. N Engl J Med. 382:e1
30. Fox SE, Akmatbekov A, Harbert JL, Li G, Brown JQ, Vander Heide RS. Pulmonary and Cardiac Pathology in Covid-19: The First Autopsy Series from New Orleans. medRxiv. 2020.04.06-20050575
31. Hu X., Chen D., Wu L., He G., Ye W. Low serum cholesterol level among patients with COVID-19 infection in Wenzhou, China. Clin Chim Acta. 2020;10:105–110
32. Fan J., Wang H., Ye G., Cao X., Xu X., Tan W. Letter to the Editor: low-density lipoprotein is a potential predictor of poor prognosis in patients with coronavirus disease 2019. Metabolism. 2020;107:154243
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





