IJCRR - 13(20), October, 2021
Pages: 36-39
Date of Publication: 24-Oct-2021
Print Article
Download XML Download PDF
Functional Outcome of Distal End Radius Fractures Treated Conservatively in a Tertiary Care Centre
Author: Sujei Sukumaran, Dennis Antony
Category: Healthcare
Abstract:Introduction: Distal radius fractures are one of the most common injuries that Orthopaedic surgeons face during their trauma practice. But it remains a dilemma to many surgeons whether to operate on patients with this kind of fracture. Objectives: Our study aimed to evaluate the functional outcome and postoperative complications of fractures of the distal end of the radius in the elderly managed conservatively in a tertiary care centre. Materials and Methods: A prospective study of cases of the distal end of radius fractures meeting the inclusion criteria admitted in Thrissur Government Medical College between 1-01-2018 to 1-06- 2019 was carried out. Fractures were classified according to the Frykman system and closed manipulative reduction attempted. After a minimum follows of 6 months the anatomical and functional outcomes were standardised using Lind storms anatomical and functional scoring system. Results: A series of 55 cases with the distal end of radius fracture were studied comprising of 24 males and 31 females. The largest contribution came from the age group of 60 to 65 years (50%). Slip and fall at home on hand was the commonest cause of injury (62.5%). Type I Frykman made the largest contribution with 22 cases. A total of 6 cases were found to develop complications including joint stiffness, paresthesia and malunion. The excellent anatomical reduction was achieved in 39 cases and good results in 9 cases. Functionally, 33 cases had an excellent outcome and 13 had a good result. Conclusion: This single-centre population series demonstrated good to excellent results in a majority of the patients after closed manipulative reduction of the distal radius, with outcomes and complications compared to other studies in the literature.
Keywords: Closed manipulative reduction, Distal end radius fracture, Functional outcome, Lind storms anatomical scoring system, Lind storms functional scoring system, Single cohort study
Full Text:
INTRODUCTION
Lower end of radius fractures is arguably one of the most common fractures of the upper extremity, encountered in clinical practice and constitute almost 17 % of all fractures and 75% of all forearm fractures.1 This fracture shows a bimodal distribution with increased incidence in the young and in the elderly.2 Pathologically distal radial extraarticular fractures are relatively stable injuries that can prove quite challenging if not managed properly. Intraarticular fractures of the distal radius, comprise a distinct and complex subgroup of wrist injuries. Disfiguring and disabling residual deformities following comminuted distal radius fractures are common to this day.
Classifying the distal radius fractures to delineate the best treatment protocols has been a monumental task as evidenced by the numerous classification systems put forth by various studies through the centuries and their relative acceptance.
The commonly used classification is the Frykman classification which depends on the extent of involvement of the articular surface of the distal radiocarpal joint (DRCJ) and distal radio-ulnar (DRUJ) joints. 3
Type I: Transverse metaphyseal fracture includes both Colles and Smith fractures as angulation is not a feature
Type II: Type I + ulnar styloid fracture
Type III: Fracture involves the radiocarpal joint
Type IV: Type III + ulnar styloid fracture
Type V: Transverse fracture involves distal radioulnar joint
Type VI: Type V + ulnar styloid fracture
Type VII: Comminuted fracture with involvement of both the radiocarpal and radioulnar joints
Type VIII: Type VII + ulnar styloid fracture
The other commonly used classification systems are
-
Gartland and WerleyClassification
-
FernandezClassification
-
MeloneClassification
-
AOClassification
Current literature equally weighs the treatment principles of closed and surgical management. Most surgeons prefer the conservative approach to distal radius fractures in elderly patients through complicated fractures with articular incongruency is still a topic of debate. The consensus is that dorsally displaced fractures are managed conservatively or with percutaneous approaches; while volar displaced fractures are treated by open surgery. In this paper, we present results of 55 cases of distal radius fractures in patients above 60 years of age treated with closed manipulative reduction and below elbow POP immobilization. The purpose of this study is to evaluate the outcome of conservative treatment in the management of distal end radius fractures in elderly patients.
MATERIALS & METHODS
This is a single cohort study done among 55 elderly patients with distal end radius fractures treated by closed manipulative reduction and Plaster of Paris (POP)immobilization at Govt. Medical College, Thrissur from 01-07-2018 to 01-07-2019.
Patients above 60 years of age with distal radius fracture treated conservatively by closed manipulative reduction and below elbow slab attending the orthopaedics Department, Govt. Medical College Thrissur was included in the study.
Exclusion criteria included patients not consenting, compound fractures and severely comminuted intraarticular fractures.
The ethical clearance for the study was obtained vide Order No. B6-8772/2016/MCTCR (8) dated 28.6.2018. Thereafter, the data were obtained for all study patients as per the proforma after getting informed written consent. Age, sex, nature of trauma, site of the fracture, any associated injuries, any pain, swelling, and loss of functions were noted. On examination, any tenderness, deformity, swelling, distal vascularity, neurological deficit and associated other injuries were also noted. X rays of both AP and Lateral views were taken. After proper history taking, clinical examination, radiological workup, patients were taken up for closed manipulative reduction and below elbow POP slab application. Post reduction, distal vascularity and neurological status re-assessed. A post-procedure check X-ray was taken to assess acceptable reduction.
Patients were advised to active finger movement and limb elevation. Patients have been instructed symptoms of compartment syndrome and warned to consult an orthopaedician if symptoms develop. They were discharged on the same day itself. After 1-week, the POP slab was inspected and converted to POP above-elbow cast without losing reduction. Patients were followed in our Outpatient Department at the end of 1st week, 6th week, 3 months, and 6 months.
RESULTS
55 Cases of distal end radius fractures in elderly patients treated conservatively with closed reduction and POP immobilization were studied and analysed using Lindstrom’s functional grading criteria.4 Among 55 cases, 31(56.4%) patients were females and 24(43.6%) were males.
In our study, the age of patients ranged from a minimum of 60 years to 80 years. The maximum number of patients belong to the 60-65 years group. The mean age is 67.9 years. Considering the side of involvement, 37 (67%) Fractures were on the right side and 18(33%) fractures were on the left side.
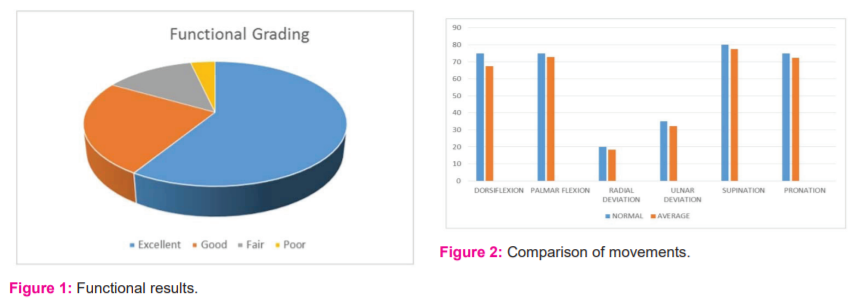
Out of 55 cases, there was no residual disability in 31 cases, 12 cases showed minimal and 10 cases showed moderate disability and 2 showed severe disability. Grip strength was not lost in 30 cases whereas 18 cases showed slight loss and 8 cases showed moderate loss and 1 showed a severe loss. Grip strength was lost in cases complicated by infection or joint stiffness. There was no residual deformity in 33 cases while 12 cases had minimal, 8 had moderate and 2 cases had a gross deformity (Table 1 & 2). 59% of the patients reported excellent functional results (Figure 1).
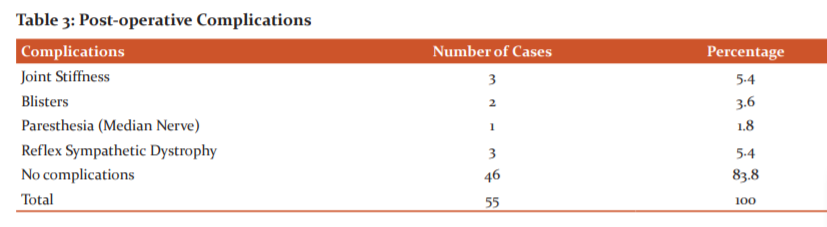
Of the 55 patients in the study who were managed conservatively, only 9 developed one or other complications ranging from mild (blisters) to paresthesia of median nerve and reflex sympathetic dystrophy. 2 cases developed blisters which were promptly treated and healed well. Both of these cases went on to develop joint stiffness and a lower functional scoring. One of the cases developed paresthesia along with median nerve distribution. 3 cases developed reflex sympathetic dystrophy. (Table 3)
DISCUSSION
This study was done among 55 patients meeting inclusion and exclusion criteria over 12 months. Functional outcomes were measured by using Lindstrom criteria.4 The results of the study were compared with a similar study conducted by other authors.
Restoration of wrist function to pre-injury levels and limitation of pain at the lowest possible cost is the clinical goals.5 To optimize function and to reduce future degenerative disease with a subsequent disability, achievement of as near anatomic position as possible is required.5,6,7,8
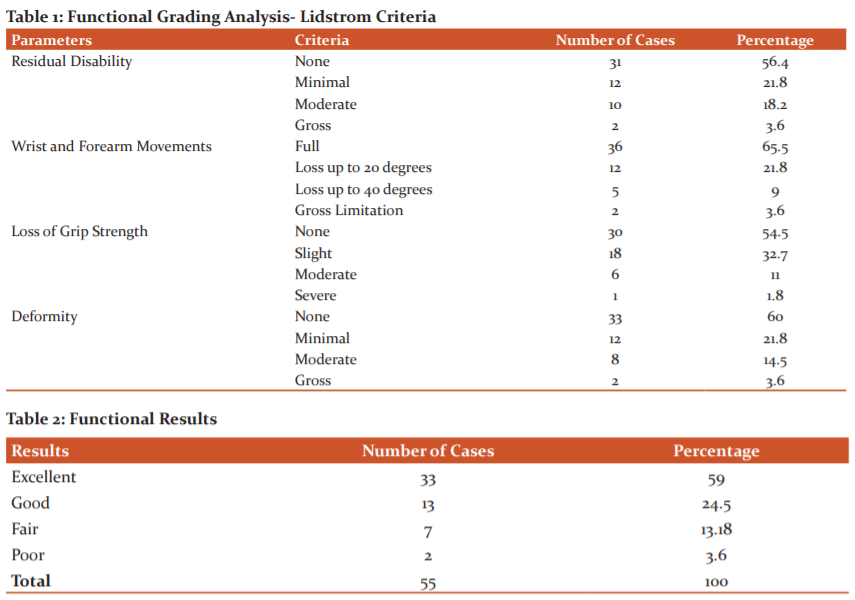
Nakata R.Y, Chand Yogesh in their series of 22 patients compared the movements of the affected side with that of the opposite side and found it be as follows - palmar flexion 60°, dorsiflexion 60°, ulnar deviation 25, radial deviation 15°, pronation 63° and supination 65°.9
The results of movements and grip strength of our series were comparable to the majority of the above series, the average results in our series were palmar flexion 72.8°, dorsiflexion 67.5°, radial deviation-18.3°, ulnar deviation- 32.3°,pronation-72.4°and supination of 77.6°(Figure 2).
Our present study also showed an excellent grip in about 54.54 % of our cases, and good grip strength in 32.7 % of the cases and fair in 10.9% of cases. Poor grip strength was observed only
in 1.8% cases.
Gupta K.et al. in their study comparing open reduction & internal fixation with the closed manipulative reduction in volar displaced distal radial fractures obtained satisfactory results in 86% cases and fair results in 14% cases.10 This is comparable to our study where 83.5% satisfactory result was obtained.
CONCLUSION
This single centre population series demonstrated good to excellent results in the majority of patients after closed manipulative reduction of the distal radius, with outcomes comparable to other studies in the literature.
This study also corroborates the finding of other well-designed studies showing the association between radiographic, anatomical and functional outcomes in the patient population with distal end radius fractures as an improved functional outcome was noted in those cases where excellent anatomical reduction could be achieved.
The myriad of classification systems and management protocols also leads us to the conclusion that a full consensus about distal radius fracture classification and management will probably never be possible. This is because surgeons will always have their personal preferences and experience-based strategies to tackle this issue.
Even in this age where implants and aggressive operative treatment is warranted in many of the fracture patterns, distal end radius fractures in the elderly are one amongst the few in which properly closed reduction and cast application have retained their importance to date, the main reason being that the less demanding population are satisfied with minor deformities if they have reasonably good functional status. Time and again the new generation has to accept the classical teachings of our great teachers of the past.
Acknowledgement: The authors are indebted to the patients who participated in this study. The authors also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript.
Source of Funding: Nil
Conflict of Interest: None
Authors’ Contribution: Sujei Sukumaran is responsible for framing the protocol, data collection and writing of first and final drafts. Dennis Antony was responsible for the concept, management and care of study participants, statistical analysis and proofreading of the drafts.
References:
-
Colles A. On the fracture of the carpal extremity of the radius. Edinb MedSurg 1814; 10:182-6
-
Ilyas AM, Jupiter JB. Distal radius fractures: Classification of treatment and indications for surgery. Orthop Clin North Am2007;38(2):167-173.
-
Frykman, G. Fracture of the distal radius including sequelae–shoulder- hand-finger syndrome, disturbance in the distal radio-ulnar joint and impairment of nerve function. A clinical and experimental study. Acta Orthop Scand: Suppl 1997; 108:103+.
-
Lindstrom A. Fractures of the distal end of the radius: A clinical and statistical study of results. Acta Orthop Scand Suppl. 1959;4:1-118.
-
Gofton W, Liew A. Distal radius fractures: nonoperative and percutaneous pinning treatment options. Orthop Clin North Am 2008;38(2):175-185
-
Abramo A, Kopylov P, Tagil M. Evaluation of a treatment protocol in distal radius fractures: A prospective study in 581 patients using DASH as an outcome. Acta Orthop 2008;79(3):376-385.
-
Nijs S, Broos PL. Fractures of the distal radius: a contemporary approach.ActaChirBelg2004;104(4):401-412.
-
Short WH, Palmer AK, Werner FW, Murphy DJ. A biomechanical study of distal radial fractures. J Hand Surg Am1987;12(4):529-534.
-
Nakata RY, Chand Y, Matika JD: External fixation for wrist fractures: a biomechanical and clinical study Jr. Hand Surgery, 1986; 10 (A): 845-851
-
Gupta K, Gaonkar N, Sudhir K, Patel N, Koli V, Date S et al. To Compare Functional Outcome, Complications & Results of Open Reduction & Internal Fixation with Closed Reduction & External Fixation in Volar Displaced Distal Radial Fractures. J of Evidence-Based Med & Healthcare. 2015;2(9):1155-1167.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





