IJCRR - 13(20), October, 2021
Pages: 20-23
Date of Publication: 24-Oct-2021
Print Article
Download XML Download PDF
Analysis of Relationship between the Curve of Spee and Various Skeletodental Parameters in Different Malocclusion Groups
Author: Madhav Manjunath, Korayem Mohammed, Khajuria Kumar Amit, Yadav Mohit
Category: Healthcare
Abstract:Introduction: The spee curve was measured from the most distal section of the second molar to the incisal edge in this study. When the incisors are included in the interpolation, the curve becomes broader, flatter, and more variable. Aim: To analyse the relationship between the curve of spee and various skeletodental parameters in different malocclusion groups. Method: 120 untreated patients' lateral cephalograms, study models, and frontal pictures were included in the study, and they were divided into five malocclusion groups. The research models were used to quantify COS depth, overjet, overbite, and arch depth. On frontal photographs, the facial index was calculated, while lateral cephalograms were used to examine other skeletaldental parameters (mandibular anterior dental height, mandibular posterior dental height, IMPA, mandibular plane angle, J-ratio, lower facial height, UFH/LFH, mandibular body length, and ramus height). Results: The COS depth was greatest in class II division 2 group and lowest in the class III malocclusion group. COS depth and overjet had a statistically significant positive link in class I, class II division 1, and class II subdivision, whereas COS depth and overbite had a statistically significant positive association in class II division 2 and class III. Conclusion: Overjet and IMPA were major contributors to the increasing curve of Spee in class II division 1, class I, whereas overbite and facial index were major contributors to the curve of Spee in class II division 2.
Keywords: IMPA, COS, Malocclusion, Overjet, Skeletodental, Overbite
Full Text:
Introduction: Exaggerated curve of spee is a typical malocclusion seen in dental malocclusions with a deep vertical overbite, posterior extrusion, and incisor proclination.1 Increased curvature of spee has been linked to a brachycephalic facial pattern2 and short mandibular bodies.3
According to Osborn, the curve of spee is formed by a combination of elements such as orofacial structure growth, tooth eruption, neuromuscular system development, and craniofacial variance.4 In orthodontic practice, levelling the curve of spee is a common operation, and the more noticeable the curve is, the more space is necessary to flatten the dentition. As a result, determining the depth of the curve of spee is crucial to the orthodontic diagnostic and treatment protocol.5
The spee curve was measured from the most distal section of the second molar to the incisal edge in this study. When the incisors are included in the interpolation, the curve becomes broader, flatter, and more variable.6 The goal of this study was to see if the presence of a Spee curve could be related to facial metrical characteristics, as well as to see whether there was a correlation between the depth of a Spee curve and other skeletodental traits.
Materials and Methodology: The present cross-sectional study was conducted in the Department of Orthodontics and Dentofacial Orthopaedics, Care Dental College, Guntur, Andhra Pradesh. The pre-treatment records (lateral cephalograms, study models and frontal photographs) of 120 subjects within the age range of 14-26 years were included in the study.
Based on the ANB angle, the 120 subjects selected were classified into three groups: Group I (skeletal class I malocclusion), Group II (skeletal class II malocclusion) and Group III (skeletal class III malocclusion). Group II, was further subdivided into Groups IIa, IIb and IIc, based on Angle’s classification of malocclusion (CDC/IEC/2020/020).
I. Analysis of Orthodontic study models:
Digital images were taken with a standardized photographic set-up and a DSLR camera to gain precision in measuring the depth of curve of Spee and arch depth. Photographs of the models' right, left, and occlusal surfaces were taken after they were put on the model platform. These images were then imported into Adobe Photoshop 7.0 for COS and arch depth measurements.
A. Curve of spee measurement: A horizontal line was drawn using the ruler tool, touching the incisal margins anteriorly and extending posteriorly to the distal cusp of the last erupted molar. The distance between the deepest cusp and another vertical line drawn perpendicular to the preceding line was measured. On the left side, a similar treatment was performed.
B. Arch depth Measurement: Photographs were cropped at 1:1 magnification, and then a horizontal line was drawn tangential to the mesial surface of one side's first molars and extending to the mesial surface of the contralateral side's first molar. Another vertical line was drawn perpendicular to this line at the level of incisal edges midway between central incisors, and the distance of this vertical line was quantified as arch depth.
II. Photographic measurements:
An extraoral frontal photograph at rest was taken to determine the facial form.
1. Softtissue nasion (N’)
2. Soft tissue Gnathion (Gn’)
3. Zygomatic prominence (Zy’)
Facial index (N?-Gn?/ Zy?-Zy?): It is taken as the ratio of the length of face to its maximal width between the zygomatic prominencies.
III. Cephalomteric Measurements:
SNA, SNB, Anterior mandibular dental height, Posterior mandibular dental height, Incisor mandibular plane angle (IMPA), Mandibular plane angle (SN-MP), Jarabak’s ratio (S-Go/N-Me), Lower facial height (LFH=ANS-Me), UFH/LFH (N-ANS/ANS-Me), Mandibular body length (Go – Pog) and Ramus height (Ar- Go).
Statistical analysis: Analysis was done using SPSS software, version 24. Test applied were Anova along with Tukey HSD Post Hoc test, Pearson correlation and multiple regression analysis.
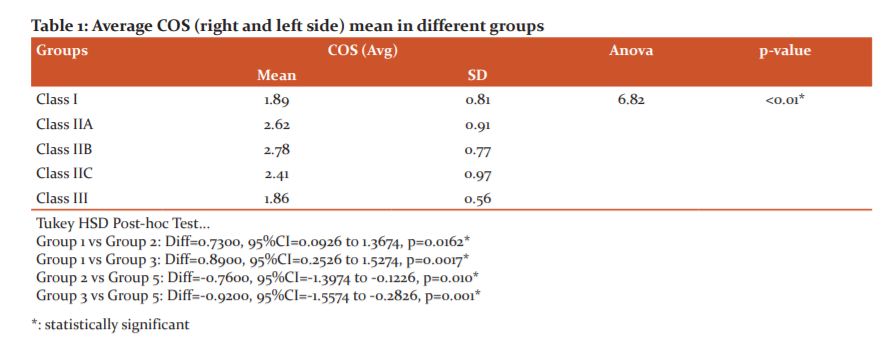
Results: The mean and standard deviation of the depth of COS for each group were analyzed and it showed no clinically significant difference between right and left sides, so the mean value was taken into consideration.
The depth of curve of Spee was maximum in class II div.2 subjects (group IIb) and least in class III subjects (group III). Depth was observed in this order: class II div. 2> class II div. 1>class II sub div.> class I >class III with statistically significant difference (p= 0.01*) as shown in table 1.
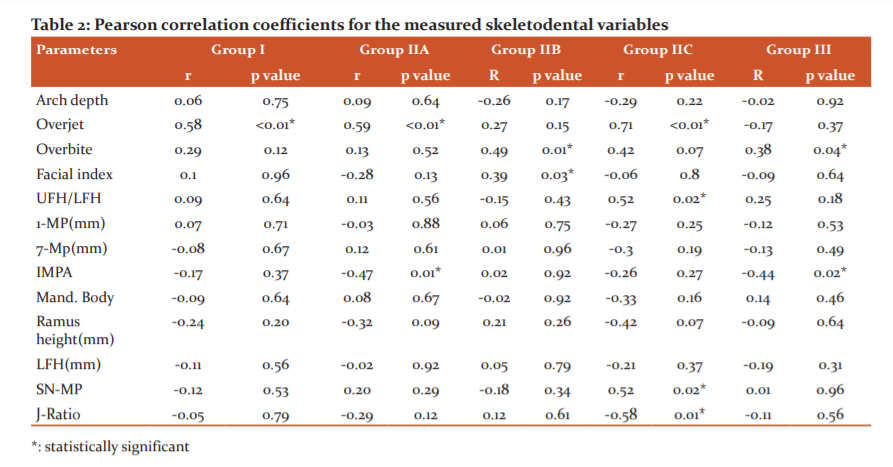
There was a positive correlation between the depth of curve of spee and overjet in groups I, IIa, and IIc but there was no correlation in groups II b and group III. The overbite was positively correlated with the depth of curve of spee in groups IIb and group III as shown in table 2.
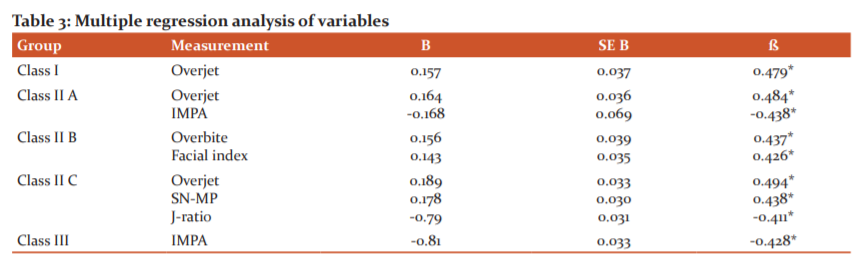
Multiple regression analysis showed that Overjet had a significant contribution to depth of cos in class IIc, class IIa and class I. Overbite had the contribution to depth of cos in class II div.2 malocclusions (β= 0.437) only. IMPA had the contribution to depth of cos in class II div.1 group and class II (Table 3).
Discussion: The assessment of the relationship of the curve of spee with multiple factors may help know the aetiology of the development of the curve of spee and treatment planning to rectify it. Hence, our present study was aimed to assess and correlate the relationship of curve of spee (COS) with dentoskeletal morphology to understand the influence of multiple factors that lead to its development.
According to Carter and McNamara, when the COS was measured on pretreatment dental casts, there was no variation in depth between male and female individuals.7 This was also reported by Farella and colleagues, hence no attempt was made to divide the sample by gender in this investigation.8
In the present study depth of the curve of spee was more in class II div.2 subjects (group 3), followed by class II div .1 subjects ( group 2) > class II subdiv. subjects (group 4)>class I subjects (group1) and least depth was seen in class III subjects (group 5). However, it did not show a statistically significant difference between class II div. 1 and div.2 subjects. This is supported by a study done by Veli and colleagues who also reported no significant difference in depth of curve of spee between class II div.1 and class II div.2 subjects.9
The depth of the spee curve grows greatly as the overjet10 grows, and the results of our investigation corroborated these findings. The results of this investigation revealed that when the overjet increases, the depth of the curve of spee in the mandibular arch rises. Veli and colleagues found a statistically significant relationship between the spee curve and the overjet.9 When overbite was compared to COS in different malocclusion groups, there was a statistically significant link. In class II div, Pearson correlation coefficient and multiple regression revealed a positive link between overbite and cos. Class II and III are the two groups. According to Burstone, deep bite therapy may include maxillary anterior tooth intrusion, mandibular anterior tooth intrusion, maxillary and mandibular posterior tooth extrusion, or any combination of these procedures.10
The facial index was connected to a deeper COS in class II div.2 malocclusions, but it did not exhibit a significant link with the curve of spee in other malocclusions, according to Pearson coefficient test findings. COS is more prominent in people with short faces and deep bites, according to Farella et al., who found that those with short faces and deep bites have higher COS.8
IMPA contributed to the curve of spee depth in class II div. 2 and class III malocclusion groups, according to multiple regression analysis. According to Balridge, a flattening of Spee's curve promotes an increase in arch circumference and decreased incisor proclination.11
Overall, the results of this study imply that the stomatognathic system compensates for dentoskeletal variation by altering the form of the spee curve, albeit only to a limited amount. One of the goals of orthodontic treatment is to level the curve of the spee, and to do so, the value of the curve of spee depth should be considered and quantified in space management procedures to avoid incisor flaring and, as a result, to ensure aesthetics, treatment stability, and function.
Conclusions: The depth of cos was greatest in class II div.2 groups followed by class II div1, class II subdiv., class I and class III with the least amount of depth. In class I malocclusion, overjet was positively correlated with COS. In class II div.2 malocclusion, overbite and facial index were related to COS. In class II sub div. malocclusion, overjet and mandibular plane angle were contributing factors for COS whereas Jarabak’s ratio was negatively related to it. In class III, IMPA was the major factor for the depth of COS.
Conflict of Interest: None
Source of Funding: None
Acknowledgement: None
Authors Contribution
Madhav M: Manuscript preparation, Data Collection
Korayem M: Statistical analysis
Khajuria AK: Manuscript editing
Yadav M: Data Collection
References:
1. Strange RH. A textbook of orthodontia. 3rd edition. Philadelphia: Lea and febiger, 1950.
2. Barager FA, Osborn JW. Efficiency as a predictor of human jaw design in the saggital plane. J Biomech. 1987;20(5);447-57.
3. Ash M. Wheeler’s dental anatomy, physiology and occlusion. 7th ed. Philadelphia: SWB Saunders, 1993.
4. Osborn JW. Orientation of the masseter muscle and the COS about crushing forces on the molar teeth of primates. Am J Phy Anthropol. 1993;92:99-106.
5. Braun S, Hnat WP, Johnson BE. The curve of Spee revisited. Am J Orthod Dentofacial Orthop 1996;110:206-10.
6. Hitchcock HP. The curve of Spee in stone age man. Am J Orthod. 1983;84:248-53.
7. Carter GA, McNamara JA. Longitudinal dental arch changes in adults. Am J Orthod Dentofacial Orthop.1998;114:88-99.
8. Farella M, Michelotti A, Van Ejiden TM, Martina R. The curve of Spee and craniofacial morphology: a multiple regression analysis. Euro J Oral Sci. 2002;110(4):277-81.
9. Veli I, Ozturk MA, Uysal T. Curve of Spee and its relationship to the vertical eruption of teeth among different malocclusion groups. Am J Orthod Dentofacial Orthop. 2015;147:305-12.
10. Burstone CP. Deep overbite correction by the intrusion. Am J Orthod 1977;72:1-22.
11. Balbridge DW. Levelling of the curve of spee and its effect on mandibular arch length. JPO 1969;3:26-41
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





