IJCRR - 13(19), October, 2021
Pages: 155-158
Date of Publication: 11-Oct-2021
Print Article
Download XML Download PDF
Infected Dentigerous Cyst - A Case Report
Author: Ingle Vijaya, Kale Lata, Pawar Anuja, Sarwade Chaitali
Category: Healthcare
Abstract:Introduction: Most common site of dentigerous cyst is mandibular or maxillary third molar or a maxillary canine. The patient typically has no pain or discomfort, unless infected. In the present paper, we report the case of a dentigerous cyst associated with an impacted mandibular canine. This cyst was missed initially due to incomplete root canal treatment associated with the nonvital mandibular anterior tooth. The present case of a cystic lesion can create a dilemma between radicular and dentigerous cyst. Aim: we present a case of an infected dentigerous cyst associated with a non -vital mandibular anterior and over-retained primary canine. Case Report: Present case of a cystic lesion can create a dilemma between radicular and dentigerous cyst. A 23 -year old male patient reported to our dental institute with a chief complaint of pain in the lower front region of the jaw for 10 days. Discussion: In the present study, CBCT was helpful in the detection of the relation of impacted canine with the adjacent vital structure which was not appreciated by OPG. Histology showed the connective tissue with dense chronic inflammatory cell infiltrate, aspirated fluid contained red blood cells suggesting that periapical inflammation from non -vital mandibular anterior spread to dentigerous cyst and caused infected dentigerous cyst. Conclusion: One year follow-up was taken healing was seen, there was no evidence of any recurrence after 1 year.
Keywords: Dentigerous cyst, Radicular cyst, Horizontally impacted canine, Non-vital mandibular anterior and over-retained primary canine
Full Text:
Introduction-
A follicular cyst is a synonym for the dentigerous cyst. Dentigerous cysts are the second most common type of odontogenic cysts after radicular cyst and also the most common developmental cysts of jaws. The term was coined by Paget in 1853 and arises from crowns of impacted, embedded, or unerupted teeth. [1] A dentigerous cyst is usually attached at the cementoenamel junction. Dentigerous cyst is a developmental cyst but inflammation can be one of the etiology. The most commonly involved teeth are maxillary ad mandibular molar and maxillary canine. [2] The present case of a cystic lesion can create a dilemma between radicular and dentigerous cyst. we present a case of an infected dentigerous cyst associated with a non-vital mandibular anterior tooth and over-retained primary canine.
CASE REPORT-
A 23 -year old male patient reported to our dental institute with a chief complaint of pain in the lower front region of the jaw for 10 days. He was apparently alright 3 months back, then he noticed swelling in gums in the lower front region of the jaw. The swelling was insidious in onset. The swelling persisted and grew progressively to present size. He experienced throbbing pain and Continuous discomfort, so he visited the department of oral medicine & radiology. Detailed history revealed the traumatic injury in the lower anterior region of jaw 13 years back in the lower front region of the jaw at age of 10yrs. The pain recurred 6 months pain for which he underwent root canal treatment with lower anterior teeth, furthered he discontinued treatment resulting incomplete root canal treatment. There was not any remarkable medical history.
On clinical examination, Extraorally there was no facial asymmetry. The single right submandibular lymph node was palpable, tender and movable of size approx. 1x1 cm. No, other abnormalities were detected.
On intraoral examination, Solitary diffuse swelling is seen in the lower front region of the jaw of size approx. 2x1.5 cm, smooth surface extending from mesial aspect of 31 to mesial aspect of 83 horizontally and vertically from labial vestibule to attached gingiva of 31 to 83. The overlying mucosa appears normal. Labial vestibule obliteration seen. Over retained 83seen. The swelling was tender on palpation firm to bony hard. Fluctuation felt at a single area suggestive of the perforation also labially cortical plate expansion was felt on palpation. Tenderness on vertical percussion positive with 41,42,83 with Grade I mobility.Vitality test was performed 31,32,41,42, 83 were non vital. A provisional diagnosis of Radicular Cyst with 31,41,42,83 was given. Differential diagnosis of Periapical abscess, Dentigerous cyst, Adenomatoid odontogenic tumour (AOT was given.
INVESTIGATIONS
-
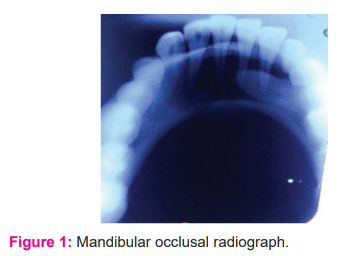
The patient was advised Intraoral periapical radiograph with Mandibular cross-sectional radiograph occlusal radiograph (FIG1), Orthopantamograph (fig2), CBCT(fig 3). Fine needle aspiration cytology revealed blood-tinged straw-coloured fluid. Radiographic finding with OPG was as follow Well defined lucent lesion is seen in the anterior region of the mandible with scalloped sclerotic borders. Cortical border touching one side root surface apically to CEJ with 43. The lesion is present from 44 crossing the midline and extending till 34. Horizontally impacted 43 present within the lesion. Over-retained 83 seen. The lesion is vertically extending from the middle 3rd of roots of teeth to the inferior border of the mandible. Thinning of cortical plates labially is evident, Eggshell crackling was felt.
Pathologic fracture seen at lower border of mandible anterior region.
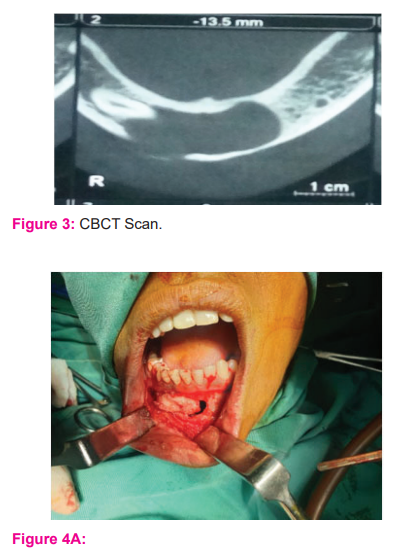
CBCT scan revealed lesion size 31.29x 16.80 x26.64 mm. Thinning of cortical plate labially is seen from 42 to 32. The lesion is involving the mandibular incisive nerve on the left side.Tooth 43 is displaced towards the inferior border of the mandible. The root apex of 43 is in contact with the mental canal on the right side. No evidence of root resorption with the lower anterior. Radiographic diagnosis of a dentigerous cyst with 43 was given. Differential diagnosis of Radicular cyst, Central giant cell granuloma, Adenomatoid odontogenic tumor was given.
Enucleation of a dentigerous cyst along with removal of the associated permanent tooth and primary canine was done. Under general anesthesia, in supine position lesion was exposed through vestibular incision, full-thickness mucoperiosteal flap was elevated. The complete lesion was excised with resection along with buccal cortical plate (fig4 A). Impacted canine was removed [fig4 B], extraction of primary canine was performed. Haemostasis was achieved. Closure done 3-0 vicryl.
On histopathological examination, the gross specimen was measuring approx. 1x 2 cm greyish coloured. H & E Stained section reveals cystic lumen lined by stratified squamous epithelium which shows arcading patterns surrounded by a fibrous capsule which is composed of bundles of collagen fibres, dense lymphocytic cell infiltration, few dilated capillaries. Also present in the stroma areas of dental follicle-like tissue. The final diagnosis is an infected dentigerous cyst with 43 was given.
DISCUSSION-
Dentigerous cysts are mostly involved with unerupted permanent teeth. It is usually discovered on routine radiographs but sometimes swelling may be present[3]. In this case, the patient had swelling and pain. According to Benn and Altini, a developmental dentigerous cyst might form a dental follicle and might become secondarily inflamed, a non -vital tooth can also be a source of infection to the permanent successor. They also mentioned that the source of secondary infection can be from a radicular cyst at the apex of non-vita teeth or another source that can lead to the formation of dentigerous cyst.[4]Depending on the time of formation on dentigerous cyst around the unerupted tooth, teeth may or may not show enamel hypoplasia. Enamel hypoplasia is seen when a dentigerous cyst commences at an early stage of development of the involved tooth whereas in cases where the cyst originating after the completion of tooth development, enamel hypoplasia is not a significant factor.[5][6]In this case, cyst originated after the completion of tooth development. Basal cell nevus syndrome, mucopolysaccharidosis and cleidocranial dysplasia show bilateral and multiple cysts have been reported.[7]The most common treatment for dentigerous cyst is marsupialization, Enucleation of a dentigerous cyst along with the removal of the associated permanent tooth if it is extensively displaced, or if the lesion is extensive.[8][9]Based on radiographic appearance, dentigerous cysts are classified into three varieties, Central type, when radiolucency encircles the crown of the unerupted tooth; Lateral type, which develops laterally along with the tooth and circumferential type, where cyst completely encircles the tooth. Radiographic examination of a dentigerous cyst appears as unilocular radiolucency of varying size, with sclerotic borders associated with the crown of an unerupted tooth. If follicular space on radiography is more than 5cm, an odontogenic dentigerous cyst can be suspected. Cases of ameloblastoma, epidermoid carcinomas, squamous cell carcinoma have been reported. [10][11][12] In the present study Cone beam computed tomography is helpful in the detection of the relation of impacted canine with the adjacent vital structure which was not appreciated by Orthopantamogram. Histology showed the connective tissue with dense chronic inflammatory cell infiltrate, aspirated fluid contained red blood cells suggesting that periapical inflammation from non -vital mandibular anterior spread to dentigerous cyst and caused infected dentigerous cyst.
Conclusion-
Early diagnosis and treatment of dentigerous odontogenic cyst lesions are very important to prevent future complications like conversion towards malignancy and thus help to prevent morbidity. Imaging like CBCT scan aids in diagnosis and treatment planning, knowledge of histopathologic features helps to confirm the diagnosis. One year follow up was taken healing was seen, there was no evidence of any recurrence after 1 year.(fig 5)
Acknowledgement -I would like to thank Oral and maxillofacial surgeon Dr. Vijay Girhe, Oral and medicine radiologist Dr. Prachi Girhe for their contribution to the case.
Conflict of interest & Source of funding -NIL
CONTRIBUTION- Author 1- has diagnosed the case, Radiographic investigations, follow-up, Manuscript preparation.
AUTHOR 2-Diagnosis case, TrManuscript corrections.
Author 3- Radiographic Investigations, Photography
Author 4-Follow upRadiographic Investigations



References:
-
Pereira T, Shetty S, Date A. Infected Dentigerous Cyst Associated with a Horizontal Impacted Ectopic Supernumerary Tooth Induced by Trauma to the Maxillary Incisors: A Rare Case Report. J Med Sci 2018;38(3):127?130
-
White SC &Pharoah MJ. Cysts.In: White SC &Pharoah MJ editors. Oral Radiology, Principles and Interpretation.First South Asia ed: REEELX India private limited publishers;2015.p.338.
-
Pai N, Sheena SS, Dubey PN, Poddar P. Infected dentigerous cyst in the maxilla: report of two cases. Indian J Dent Sci 2020;12:244-7.
-
Benn A, Altini M. Dentigerous cyst of inflammatory origin, a clinicopathologic study. Oral Surg Oral med Oral path Oral Radiol Endo.1996; 81:203-9
-
Patil et al. Infected Dentigerous Cyst and its Conservative Management: A Report of Two Cases. International J Clin Paediatric dentistry. 2019 Jan-Feb; 12(1): 68–72.
-
Browne RM, Smith AJ. Pathogenesis of odontogenic cysts. In: Investigative Pathology of the Odontogenic Cyst. CRC Press Boca Raton, 1991; p 88-109.
-
Rajendran R. Cyst and tumours of odontogenic origin. In: Rajendran R, Sivapathasundharam B, editors. Shafer’s Textbook of Oral Pathology. 5th ed. New Delhi: Elsevier Publishers; 2006. p. 360?1.
-
Kambalimath DH, Kambalimath HV, Agrawal SM, Singh M, Jain N, Anurag B, et al. Prevalence and distribution of odontogenic cyst in Indian population: A 10-year retrospective study. J Maxillofac Oral Surg 2014;13:10?5.
-
Shear M, Speight PM. Odontogenic keratocyst, in cysts of the oral and maxillofacial regions. Copenhagen: Blackwell Munksgaard. 2007. p. 59-75.
-
Sharma et al. Inflammatory Dentigerous Cyst: A Rare Entity. J Res Adv Dent 2014; 3:2s:4-7.
-
Waldron CA. cysts and tumours. In: Oral and Maxillofacial pathology, Neville BW, Damm DD, Allen CM, Bouquot JE, (eds), Philadelphia: W.B. Saunders, 1995, p 493- 540.
-
Yasuoka T, Yonemoto K, Kato Y, Tatematsu N. Squamous cell carcinoma arising in a dentigerous cyst. J Oral Maxillofac Surg 2000;58:900?5.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





