IJCRR - 7(20), October, 2015
Pages: 06-08
Date of Publication: 20-Oct-2015
Print Article
Download XML Download PDF
STUDY OF CORONARY DOMINANCE IN THE POPULATION OF HYDERABAD KARNATAKA REGION
Author: Jaishree H., Ashwini H.
Category: Healthcare
Abstract:Aim: To determine the dominance pattern of coronary artery in adult human hearts of Hyderabad Karnataka region. Materials and Method: 76 human cadaveric hearts were studied and analyzed by dissection method to know the dominance pattern of coronary artery. Result: Out of 76 heart specimens, Right dominance was found in 63 cases (83%), left dominance in 11 cases (14.5%) and co dominance in 2 cases (2.5%). Conclusion: In our present study right coronary artery was dominant. Knowledge of dominant pattern is significant for determining the prognosis of coronary artery disease. Hence this study was done, which would be helpful to the physicians belonging to the Hyderabad Karnataka region.
Keywords: Coronary dominance, Coronary artery disease, Posterior interventricular artery
Full Text:
INTRODUCTION
The term dominant coronary artery was coined by Schlesinger to indicate the areas of heart supplied by right and left coronary artery.1 The distribution of coronary arteries does not follow uniform pattern in all the hearts. The pattern of blood supply is classified into three type’s i.e. Balanced, right dominance and left dominance.2 The increasing use of diagnostic and therapeutic interventional procedures necessitates a sound and basic knowledge of the coronary artery pattern. Coronary artery anomalies are gaining consideration as a cause of coronary heart disease in the diagnosis workup.3 As Coronary artery disease is one of the most common heart diseases and also the major cause of death in developing countries, this study would be helpful to physicians, radiologists and surgeons of Hyderabad Karnataka region to understand the pattern of coronary arterial dominance.
MATERIALS AND METHOD
The sample size used for this study is 76 heart specimens. The specimen of adult human hearts used for this study were obtained from routine dissection conducted for undergraduate students from the Department of Anatomy, Bidar Institute of Medical Sciences, Bidar and also from other nearby medical colleges of Karnataka. By cutting the ribs and sternum the thoracic cavity is opened. The great vessels were ligated. The parietal pericardium is incised and heart along with great vessels is taken out of the pericardial cavity. Each specimen is thoroughly washed to free it from the blood clots. All specimens are preserved in 10% formalin solution. The specimens were labelled numerically. The origin of right coronary artery from the ascending aorta is identified. The right coronary artery lies in between right auricle and right side of pulmonary trunk. Then the right coronary artery is dissected along its course running in the right atrioventricular groove and traced on the posterior surface of heart running in the coronary sulcus towards the crux of heart and noted for origin of PIVA (posterior interventricular artery). On the anterior surface of the heart, Origin of the left coronary artery arising from the ascending aorta is identified i.e. between the left auricle and the left side of the pulmonary trunk. The LCA (left coronary artery) was traced until its division on the superior end of anterior interventricular groove which branched into LAD (left anterior descending) and LCX (left circumflex) artery. The LCX artery is dissected along its course on the posterior surface of the heart and noted for origin of PIVA. The PIVA running in the posterior interventricular sulcus is identified. The PIVA is dissected along its course upto the termination. The origin, course of PIVA is noted.
RESULTS
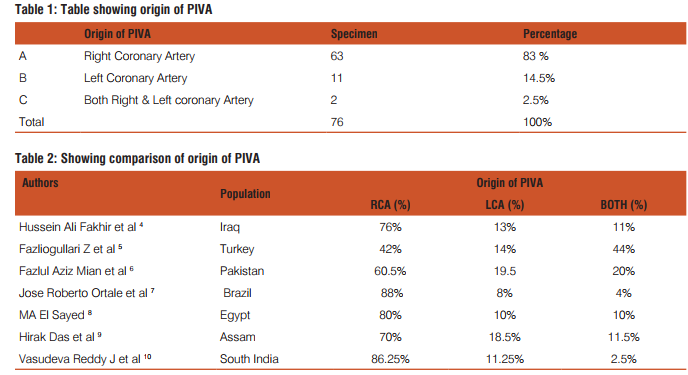
The present study is carried on 76 specimens of cadaveric hearts and observed for the dominance of coronary arteries. In our study, it is observed that out of 76 specimens studied, the PIVA originated from RCA (right coronary artery) in 63 (83%) cases, in 11 (14.5%) cases PIVA originated from LCA, in 2 (2.5%) cases PIVA originated from both RCA and LCA.
DISCUSSION
The incidence of left coronary arterial dominance in present study was 14.25% as compared to 18.5% reported by Hirak Das et al 9 , 11.5% by Vasudeva Reddy J et al 10, 10% by MA El Sayed 8 , 8% by Jose Roberto Ortale et al 7 . The variation in result could be due to racial and geographical variation. Keshav Kumarstudied the relation between coronary arterial pattern and coronary artery disease. He described about the types of dominant pattern. 1. Right coronary arterial dominance (83%) 2. Left coronary arterial dominance (16%) 3. Right coronary arterial great dominance (0.7%) 4. Coronary arterial no dominance (0.3%) There is increased incidence of coronary heart disease in the persons with left coronary arterial dominance and co dominance heart. In left coronary dominance and co dominance, the left coronary artery has to supply entire interventricular septum due to which the pulse pressure of blood rises more than 60mmHg in it producing atherosclerosis.11 Hirak das et alstudied coronary dominance in population of Assam in 70 hearts and found right dominance in 70%, left dominance in 18.75% and co-dominance in 11.43%.9 Dr Hussein Ali Fakhir et alstudied the coronary artery dominance by angiography and their relationship with coronary artery disease in 657 Iraqi patients consecutively suffering from coronary artery disease. The right coronary artery was dominant in 76.4%, left dominant in 12.6%, co dominant in 10% cases. No significant difference in type of coronary dominance in relation to sex and age. There was significant association between right dominant system and coronary artery disease especially 3 vessel disease and right coronary artery occlusion.4 J. Vasudeva Reddy et al studied the origin, branching pattern and termination of coronary arteries in population of Andhra Pradesh. He dissected 80 human heart specimens by using vascular corrosion technique. Out of 80 specimens dissected 69 were of right dominance, 9 specimens were of left dominance and 2 specimens were of co-dominance type of coronary circulation. Incidence of right coronary dominance is higher in males than females. Left predominance is higher in males indicating the reason for higher incidence of myocardial infarction in males when compared to females.10
CONCLUSION
Schlesinger in his study correlated the thrombosis and angina pectoris with coronary arterial pattern and concluded that the coronary artery disease is more prevalent in left coronary arterial dominance.1 Left coronary dominance have high mortality while performing cardiac catheterisation for acute coronary syndromes. Left coronary dominance is the only predictor of peri procedural myocardial infarction following the implantation of second generation drug eluting stents and was also associated with higher rate of myocardial infarction during follow up. Left coronary dominance and co-dominance had higher mortality in hospitals after performing percutaneous intervention for acute coronary syndrome.12 In our study Right dominance is found in 83%, left dominance in 14.5% and co dominance in 2.5% cases. Considering the risk of higher mortality in left coronary dominance and coronary co-dominance pattern, more prevalence of myocardial infarction in left coronary dominance, the present study was done. This study would be helpful to the cardiologist, radiologists and surgeons of The Hyderabad Karnataka region.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in the reference of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed
References:
1. Schlesinger, M. J. Relation of the anatomic pattern to pathologic conditions of the coronary arteries. Arch.Pathol.30:443, 1938.
2. Ayer AA, Rao YG. A radiographic investigation of coronary arterial pattern in human hearts. J Anat Soci India. Jun 1957; 6(1) 63-67.
3. Subhash D Joshi, Sharda S Joshi et al. Origins of the coronary arteries and their significance. Clinics 2010; 65 (1):79-84.
4. Dr. Hussein Ali Fakhir, Pattern of coronary artery dominancy by coronary angiography in Iraqi patients and the relationship with coronary artery disease. Journal of college of education 2012; 3(2):180-189.
5. Fazliogullari Z et al. Coronary artery variations and median artery in Turkish cadaver hearts. Singapore Med J 2010; 51(10) : 775.
6. Fazlul Aziz Main et al. Coronary Artery Dominance: What pattern exists in Pakistani Population? Annals of Pakistan Institute of Medical Sciences 2011; 7(1): 3-5.
7. Jose Roberto Ortale et al. The posterior ventricular branches of the coronary arteries in human artery. Arquivos Brasileiros de Cardiologia 2004; 82(5):468-471.
8. Madiha Awad El Sayed. Anatomical study of right coronary artery with special reference to its interventricular branch. Alexandria faculty of medicine 2008, vol.44 (2); 536-547.
9. Hirak Das, Geeta Das et al. A study of coronary dominance in the population of Assam. Journal of Anatomical Society of India 2010; 59 (2): 187-91.
10. Vasudeva Reddy J, Lokanadham S. Coronary Dominance in South Indian Population. Int J Med Res Health Sci.2013; 2(1):78-82.
11. Kumar Keshaw. Coronary arterial pattern and coronary heart disease. Anatomica Karnataka 2008; 3 (2): 27-34.
12. Nisha I. Parikh, Emily F. Honeycutt, Matthew T. Roe et al. Coronary Artery dominance and death in Acute Coronary Syndromes. Circ Cardiovasc Qual Outcomes, journal of American heart association November 2012(5) p1-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





