IJCRR - 7(21), November, 2015
Pages: 59-65
Date of Publication: 11-Nov-2015
Print Article
Download XML Download PDF
ASSESSMENT OF BONY TRABECULAR PATTERNCHANGES SEEN IN GROWING SKELEAL CLASS-II MALOCCUSION TREATED WITH TWIN BLOCK THERAPY
Author: Shaharyar Ahmad, Ranjit H. Kamble, Sunita Shrivastav, Narendra Sharma, Ranjit Patil, Abhilasha Goyal
Category: Healthcare
Abstract:Purpose: The purpose of this study was to assess the bony trabecular pattern changes seen in growing skeletal class-II malocclusion treated with twin block therapy and comparison with non-treated group. Material and Methods: Full mouth Periapical radiographs of patients were taken pre and post twin block therapy. Regions of interest (100×100 pixels) were located between apices of the teeth of the maxillary and mandibular anterior, premolar, and molar area. The fractal dimension (FD) was calculated by using the box counting method. The particle count (PC) and area fraction (AF) analyses were also performed. Results: There was significant difference in the FD values among the different groups of age, gender, upper, and lower jaws. The p-value of FD-0.011, PC-0.001 and AF-0.002 showed significant results after post twin block therapy. Conclusion: In this study pre-treatment radiographs showed irregular vertical arrangement of the spongy trabeculae running from the walls of the socket of one tooth or root to the next and also parallel to the long axis of tooth. Post-treatment radiograph showed a regular horizontal arrangement of spongiosa and dense trabeculation and perpendicular to long axis of tooth.
Keywords: Twin block therapy, Bony trabeculae, Skeletal class II, Fractal dimensions(FD)
Full Text:
INTRODUCTION
The alveolar bone is the thickened ridge of bone that contains a region of compact bone, adjacent to periodontal ligament(PDL), which is called the lamina dura when viewed on radiographs. The alveolar bone is divided into the alveolar bone proper(compact bone) and supporting alveolar bone (cortical and trabecular bone). The trabecular bone(cancellous bone) is located between alveolar bone proper and plates of cortical bone. It is stated that in the posterior maxilla; the trabeculae are typically thin, and numerous, forming a fine, granular, dense pattern, and the marrow spaces are consequently slightly larger than the anterior region of the maxilla and relatively numerous. In the posterior mandible, the peri-radicular trabeculae are somewhat thicker than in the maxilla resulting in a coarser pattern and they are relatively larger than the trabeculae in the anterior region of the mandible. The trabecular plates in the mandible are also fewer than in the maxilla and marrow spaces are correspondingly larger.(1)Because of its high surface-volume ratio the trabecular bone is believed to have an 8-fold higher turnover rate than cortical bone and to be highly responsive to metabolic stimuli.(2) This is an important phenomenon since the maxilla and mandible are rich in trabecular bone, particularly in the anterior regions.In 1892 Wolf’s Law stated that – “every change in the form and function of bone or of their function alone is followed by certain definite changes in their internal architecture and equally definite alteration in their external conformation, in accordance with mathematical laws”.(3)Wolf’s law states that there is a nature’s attempt to organize and orient the bony trabeculae in the direction of force vector. The most common skeletal problem in orthodontics is the Class II malocclusion characterized by mandibular retrognathia.(4) Functional appliances contribute to Class II correction in growing patients through a combination of dentoalveolar and skeletal effects. Skeletal changes has been shown to account for approximately one-third of the decrease in overjet that is seen in successful cases, with the remainder predominantly maxillary incisor retroclination.(5) A wide range of functional appliances aimed to stimulate mandibular growth by forward posturing of the mandible are available to correct this type of skeletal and occlusal discrepancy. (6)Among all the functional appliances, the Twin-block has gained increasing popularity during the last decade,(7)Hence twin block appliance was chosen to assess the changes in bony trabeculae. Twin block appliance was introduced by Scottish orthodontist William Clark, in 1977. It is like a two-piece or split activator using separate maxillary and mandibular appliances with occlusal acrylic portions that serve as inclined guide plane and bite blocks. This bite blocks induce favourably occlusal forces by causing a mandibular displacement in downward and forward direction. (8) Twin block appliance has to be worn full time and it is tooth borne and tissue borne. This appliance tends to bring out new pattern of mandibular closure. It favours or stimulates potential mandibular growth in sagittal plane thereby correcting skeletal class-II malocclusion and changing the orientation of trabeculae due to the change in the position of mandible. To visualize these changes in trabeculae, IOPA and Panoramic radiographs are the most preferable diagnostic aid. An understanding of normal anatomical structures on the radiographic image is fundamental for using the images as a diagnostic aid or in designing research. Therefore, an effort has been made to identify and understand most structures that appear on intra- and extra-oral radiographs. Dental researchers and clinicians have historically assumed the lattice-like pattern observed on intra-oral radiographs as an accurate image of the internal bony medullary cavity. The radiographic appearance of normal (healthy) trabecular bone was described almost 80 years ago and that traditional description has not been changed since then.(9) Bone trabecular pattern can be characterized by a number of measures including area of the bony plates, circumference of the trabeculae, number of bony and marrow regions, thickness of the trabeculae, trabecular spacing, and osseous fractal dimension.(10) It must be recognized, however, that it is unclear which structures give rise to the trabecular pattern seen on dental radiographs. Hence the purpose of this study was to visualize the changes seen in bony trabeculae due to change in the position of mandible by twin block appliance in skeletal class II patients with retrognathic mandible.
MATERIAL AND METHODS:
The present study was carried out in the Department of Orthodontics and Dentofacial Orthopaedics, Sharad Pawar Dental College, Datta Meghe Instiute of Medical Sciences, Wardha, and Maharashtra. The study was approved from the ethical committee of Datta Meghe Institute of Medical Sciences. Study sample comprised of 10 skeletal class-II cases with mandibular deficiency in mixed or early permanent dentition attended the OPD of Sharad Pawar Dental College and Hospital, Sawangi. Written consent form from all the participating samples was taken. Routine orthodontic records along with full mouth IOPA were taken. Data was analysed using software: - INTRA ORAL GRID for analysis of bony trabeculae’s. The sample consisted of 10patients (5Males and 5Females) with the average age of 10 to 13years with no specific medical history. The patients were clinically and cephalometrically diagnosed as skeletal class II with retrognathic mandible. IOPA of all 10 patients were taken at 2 intervals: pre-treatment and post twin block therapy (duration was 6-8months).
METHOD
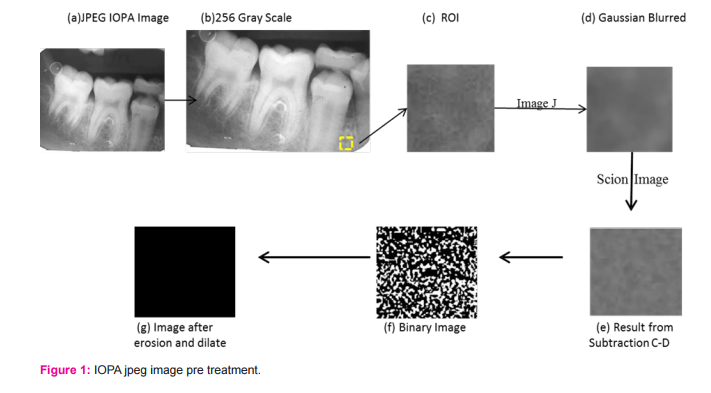
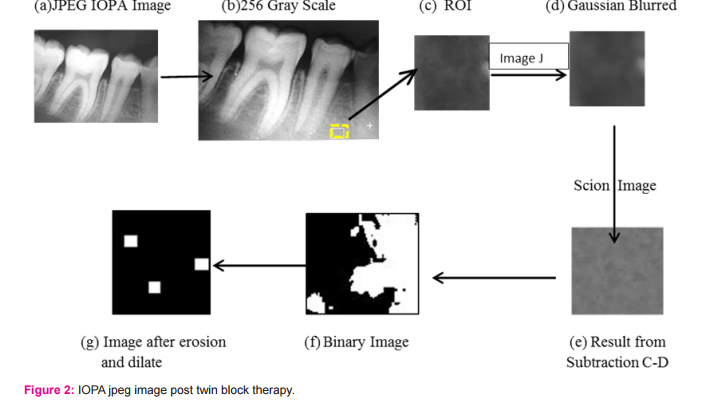
The alveolar bone surrounding the maxillary and mandibular permanent or mixed dentition on the periapical radiographs was evaluated. The periapical radiographs were digitized with windows 8.1 interfaced with Adobe Photoshop 7.0 software. A 256-gray-scale image was captured from a single periapical film at a resolution of 600 pixels per inch. Region of interest (ROI) measuring 64 X 64 pixels was selected near the root apices of the incisors, canines, premolar and molar teeth. Teeth structure, periodontal ligament (PDL), and lamina dura excluded upon selection of each ROI. Then the image was cropped and saved in BMP format. The ROI was selected in six regions (anterior, premolar, and molar areas in the upper and lower jaws) from each case using Image J (ver. 1.46r, National Institute of Health, USA, Java 1.6.0_20: 64-bit). The ROI was selected and processed further using the method designed by White and Rudolph.(11) In brief, the original cropped ROI was filtered using Gaussian blur in Adobe Photoshop 7.0 software to remove the fine and medium scale variations in image brightness, and then saved again. Using Scion image, the original ROI and the blurred one were subtracted from each other and multiplied by 1 and added 128. Then the resultant image was converted to binary with threshold at grey level of 128. The binary image was eroded three times and dilated three times to reduce the noise shown in fig. 1 and 2. Final image was obtained and used for fractal analysis and particles count and area fraction. All digital manipulations and measurements were made within ROIs. Image J software was used for calculating the fractal dimensions (FDs) of the image by the Box Counting function. Initially, the binary or threshold image was converted by square grid and the widths of the square boxes were 2, 3, 4, 6, 8, 12, 16, 32, and 64 pixels.(12) Subsequently, the numbers of the counted tiles were plotted against the total number of tiles in a double logarithmic scale. Finally, FD was calculated from the slope of the line fitted on data points. Image J software was used to measure the particles counts (PCs) and the area fraction (AF) of the region of interest (ROI). The particles counts (PCs) command counted and measured the objects in the region of interest (ROI) in binary images. Here, AF means the percentage of pixels in the image.(12)
STATISTICAL METHODS
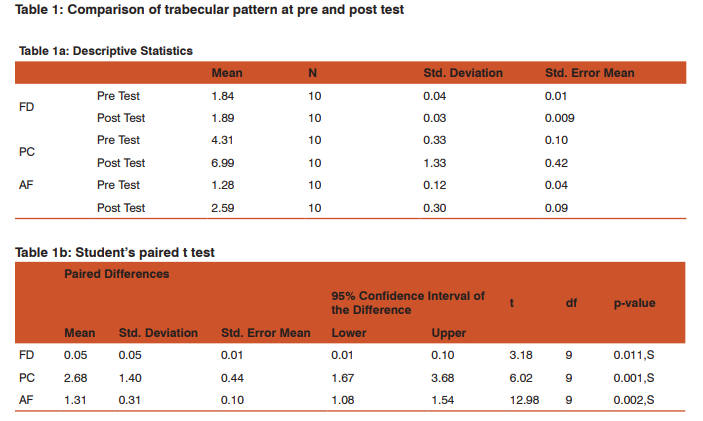
Statistical Analysis was done by using descriptive and inferential statistics using student’s paired t test and software used in the analysis was SPSS 17.0 version and p<0.05 is considered as level of significance.
OBSERVATIONS AND RESULTS
The cases in this study included 5males, and 5females. There was significant difference in the FD values among the different groups of age, gender, upper, and lower jaws.
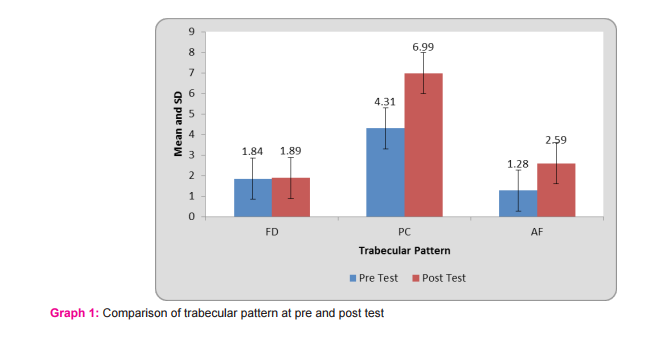
1. The mean value for FD in pre-treatment was 1.84 ± 0.04& in post twin-block therapy was 1.89 ± 0.03 and the p-value of FD was 0.011 showed statistically significant changes.
2. The mean value for PC in pre-treatment was 4.31 ± 0.33 & in post twin-block therapy was 6.99 ± 1.33 and the p-value of PC was 0.001 showed statistically significant changes.
3. The mean values for AF in pre-treatment was 1.28 ± 0.12 & in post twin block therapy was 2.59± 0.30 and the p-value of AF was 0.002 showed statistically significant changes.
DISCUSSION
This study examined the trabecular architecture on intraoral radiographs. Intra-oral periapical radiographs are usedin general dental practice to diagnose dental diseases like periapical lesions, to locate the position of impacted teeth. From orthodontic point of view it is commonly used to assess orthodontically induced root resorption, root formation, bony trabecular pattern and growth status (mandibular canine calcification and MP3). In addition, it needs no special standardization technique. Thus, it is a cost-effective tool to identify individuals. Intra-oral radiographs are preferred over extra-oral as they overcome the geometric distortion that occurs in panoramic radiographs. In addition they better visualize the bone density and the trabecular pattern.(13) Therefore to visualize the changes in bony trabeculae pattern, IOPA of 10 patients were taken pre-treatment and post treatment (twin block therapy) and these IOPA were examined by fractal analysis. The result showed statistically significant changes in the bony trabeculae of maxilla and mandible in all regions of interest due to the functional therapy. Of the several methods that have been developed to estimate the alveolar bone density from dental radiographs, fractal analysis appears to hold the greatest promise as an inexpensive and readily available method.(14) The trabecular bone has a branching pattern that exhibits fractal properties such as self-similarity and lack of well-defined scale. Because of this phenomenon, the application of fractal geometry and the measurement of fractal dimensions can be used to determine trabecular complexity and bone structure.(15) Fractal analysis is a technique for identifying scale-invariant structure that is not affected by exposure or minor alignment variations of radiographs. This makes it well suited for the analysis of trabecular bone patterns in radiographs. There are many approaches for estimating fractal dimension, but the box counting method is the most widely used and is suited for binary image analysis. Fractal analysis gives any idea about quantitative changes as being increased or decreased but does not give a numerical value of changes occurring in the trabeculae. There is still an opportunity to further optimize the image for characterization of the trabecular and marrow components of the bone. In this study the fractal dimension in all regions of upper and lower jaw pre-treatment and post twin block therapy showed statistically significant results with pvalue-0.011 (Table 1b). This proved that the FD of all the jaw sites pre-treatment and post treatment were not similar, thus the results indicated further investigation to rule out changes in BMD. However, it must be stressed that the clinician or the researcher would have to follow the same data processing protocol described in this study because any variations in this process might affect the results. In 2006, Jolley et al(16) showed that the periapical radiographs could provide a reliable method for determining fractal dimension to analyse the changes in alveolar bone density of various bone diseases. In 2012 Maha Eshak Amer et al(12) examined that the PC of each site revealed a significant correlation with the other sites of the jaws. The PC represented the area of the trabeculae in the ROI, therefore it might not be related with its perimeter which was represented by FD. AF, the ratio of the particles in ROI, of the anterior premolar area showed a significant correlation with those of the upper premolar and lower premolar areas, while the AF of premolar area showed a significant correlation with those of the upper anterior, lower premolar, and lower molar areas. The AF of the upper molar area showed a significant correlation with those of the upper anterior, the lower anterior, and lower premolar areas. In this study the p-value of PC was 0.001(Table.1a) which showed statistically significant changes and also the difference in the mean value of pre-treatment and post-treatment 4.31 ± 0.33 and 6.99 ± 1.33 (Table.1a). Also there was a significant correlation seen in the value of PC in upper and lower jaw(Table.1b). Results of this study showed that changes occurred in the area of trabeculae in the region of interest in upper and lower jaw after post twin block therapy. The p-value of AF was 0.002 showed a statistically significant changes in post twin block therapy compare with pretreatment (Table.1b) and there was a significant changes seen in upper and lower jaw (Table 1b). Results showed that the ratio of particles in ROI have changed in post twin block therapy in relation to pre-treatment Trabecular shape and orientation are adaptive to changes in the mechanical environment, such as those induced by aging or osteoporosis. In these conditions some trabeculae disappear; indeed, trabeculae oriented in the direction of the main forces applied to the bone are not removed, or are removed last because of the adaptation phenomenon.(12) In this study trabecular shape, orientation and pattern were changed due to the change in the position of mandible by a functional appliance therapy. According to Proffit(4) and other researchers it is believed that bony trabecular pattern is perpendicular to occlusal plane and parallel to long axis of tooth and when a orthodontic force is applied, the position of mandible is changed and the bony trabecular pattern arranged parallel to the forces and perpendicular to the long axis of tooth. In this study there was significant changes have occurred in bony trabecular pattern visible in the post treatment IOPA of patients.
CONCLUSION
Pre-treatment radiographs showed irregular vertical arrangement of the spongy trabeculae running from the walls of the socket of one tooth or root to the next and also parallel to the long axis of tooth. Post-treatment radiograph showed a regular horizontal arrangement of spongiosa and dense trabeculation and perpendicular to long axis of tooth. Thus the retention phase is advisable after the active treatment phase for the re-orientation of trabeculae to its original position for preventing the relapse.
ACKNOWLEDGEMENT
The authors thank Dr. R. Patil and Dr. Vishal Khanna for supporting and analysing the study material. Special gratefulness is extended to Dr R. Kamble, Dr. S Shrivastav and Dr. Abhilasha Goyal for their support and guidance throughout this study. Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors /publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Van Rietbergen B, Muller R, Ulrich D, Ruegsegger P, Huiskes R. Tissue stresses and strain in trabeculae of a canine proximal femur can be quantified from computer reconstructions. Journal of Biomechanics 1992 February; 32(2) : 165-173.
2. Lang P, Steiger P, Faulkner K, Gluer C, Genant HK. Osteoporosis. Current techniques and recent developments in quantitative bone densitometry.RadiolClin North Am 1991; 29:49-76.
3. Wolf J, Das Gesetz der Transformation der Knochen. Hirschwald A, Berlin ( Springer-Verlag published an excellent English translation of this monograph in 1986),1982.
4. Proffit WR, Fields HW. Contemporary Orthodontics. 3rd edition. St Louis, Mo: Mosby; 2000; 13: 96–98, 260–269, 481.
5. O’Brien K, Wright J, Conboy F. Effectiveness of early orthodontic treatment with the Twin-block appliance: a multicenter, randomized, controlled trial. Part 1: Dental and skeletal effects. Am J Orthod Dentofacial Orthop. 2003;124: 234–243
6. McNamara JA Jr, Brudon WL. Orthodontics and dentofacial orthopaedics. Ann Arbor: Needham Press; 2001. p. 67-80.
7. Baccetti T, McNamara JA. Treatment Timing for Twin block Therapy; (Am J Orthod Dentofacial Orthop 2000; 118:159-70)
8. Clark WJ. The twin-block traction technique.Eur J Orthod 1982; 4:129-38.
9. Jett S, Shrout MK, Mailhot JM, Potter BJ, Borke JL. An evaluation of the origin of trabecular bone patterns using visual and digital image analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004; 98: 598-604.
10. Parfitt AM. Trabecular bone architecture in the pathogenesis and prevention of fracture. Am J Med 1987; 82: 68-72.
11. White SC, Rudolph DJ. Alterations of the trabecular pattern of the jaws in patients with osteoporosis. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1999; 88: 628-35.
12. Amer ME, Min-Suk Heo, Brooks SL, Benavides E. Anatomical variations of trabecular bone structure in intraoral radiographsusing fractal and particles count analyses. Imaging Sci Dent 2012; 42 : 5-12.
13. Diane P, Grethe J, Stavros K. Assessment of trabecular pattern on periapical and panoramic radiographs: A pilot study. Acta Odontol Scand, 2010; 68: 91-97.
14. Yasar F, Akgünlü F. Fractal dimension and lacunarity analysis of dental radiographs. Dentomaxillofac Radiol 2005; 34 : 261-7.
15. Haire TJ, Hodgskinson R, Ganney PS, Langton CM. A comparison of porosity, fabric and fractal dimension as predictors of the Young’s modulus of equine cancellous bone. Med Eng Phys 1998; 20: 588-93.
16. Jolley L, Majumdar S, Kapila S. Technical factors in fractal analysis of periapical radiographs. Dentomaxillofac Radiol 2006; 35: 393-7.
17. Updegrave, William J. Normal Radiographic Anatomy. Dental Radiorraphy and Photography, December 1958: 57-65.
18. Nicholas Joseph Brescia. A Roengenographic Study of the Trabecular Pattern of the Alveolar Processes of the Human Maxilla and Mandible.Loyolauniversity, Chicago 1959.
19. Graber, Rakosi and Petrovic, Dentofacial Orthopaedics with Functional Appliances, 2nd Edition.
20. Laura E, Bollen AM, Robert ML, Susan WH, Jeremy BC, Curtis SK Chen, Lars GH et al. Trabecular and cortical bone as risk factors for orthodontic relapse. Am J Orthod Dentofacial Orthop 2006; 130:476-84
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





