IJCRR - 13(18), September, 2021
Pages: 124-128
Date of Publication: 26-Sep-2021
Print Article
Download XML Download PDF
Efficacy of Proprioceptive Neuromuscular Facilitation on Posture in Parkinson's Disease: A Randomized Controlled Trial
Author: Punia S, Malik M, Singh V, Bodwal K, Kaur J
Category: Healthcare
Abstract:Aim: The study aimed to assess the effect of PNF techniques forward head posture (FHP) in patients suffering from Parkinson's disease. Material and Methods: This is a randomized controlled trial study. 40 subjects of forwarding head posture (FHP) with Parkin�son's disease with craniovertebral angle (CVA) measured less than or equal to 500 and subjects were randomized in two groups: groups A experimental (N=20) & group B control (N=20). The intervention group performed forward head posture corrective exercise in the form of PNF stretching exercise. The craniovertebral angle was measured before and after thrice in a week for 2 weeks exercise program. Result: After 2 weeks, a significant increase was observed in the intervention group regarding the mean of CVA (p< 0.001). When we compared the mean difference of outcome variable of both groups, CVA increased significantly after 2 weeks (MD= 2.63; 95% CI -2.16 to -1.13; t38= -6.50; p< 0.001). Conclusion: The current study showed that PNF stretching is a more effective treatment and could significantly improve the CVA angle in forwarding head posture. The results of the study suggest that PNF stretching is more effective in FHP. PNF stretching also increases the cervical range of motion, improve muscle elasticity.
Keywords: Parkinson’s disease, Forward Head Posture, Craniovertebral Angle, Proprioceptive Neuromuscular Facilitation, Strength�ening, Stretching
Full Text:
Introduction
Parkinson’s disease was described by James Parkinson in 1817. ‘An essay on shaking palsy. In 1912, firstly it was recognized as an extrapyramidal disorder by Kinner Wilson.1 It is a chronic, progressive degenerative disorder of the nervous system characterized by cardinal features of rigidity, akinesia, bradykinesia, tumour, postural stability and muscle weakness.2 About 10 million people are affected worldwide.3 Parkinson’s disease affected about 3% of the population. It is characterized by the loss of dopaminergic function and consequently diminished motor function, leading to the clinical presentation of the disease.4 Nigrostriatal dopaminergic pathway degeneration leads to primary motor symptoms of Parkinson’s.disease that includes inflexibility, bradykinesia, resting tremor & gait disturbances.5 Motor symptoms include disturbances in the posture of gait & posture is responsible for functional disability in individuals with Parkinson’s disease.3
Forward head posture (FHP) is the increase in the extension of the cervical spine in the upper region with an increase in flexion of the cervical spine in the lower region and upper thoracic spine, the position of the head is around the sagittal plane shows forward deviation through gravity line. Assessment of FHP is done in mainly two positions: a sitting position and a standing position. In each position, a picture of each subject was taken from the lateral view and the craniovertebral angle (CVA) is calculated which is a reliable and valid indicator for FHP.6,7
The Researcher illustrated proprioceptive neuromuscular facilitation (PNF) exercise pattern consists of a diagonal movement that places greater prominence on functional training. Past studies evidence suggest that optimization of PNF as an exercise training protocol, especially in the elderly can improve proprioception, muscle strength, physical-functional, coordination, mobility, balance & gait of patients.8,9 Previous research finding evaluated the effect of stretching &strengthening exercise to improve FHP but the PNF & resisted exercise can also beneficial to increase range of motion & FHP in Parkinson’s patients.3 several theories show the significant result of either resistance training or PNF training to improve stability (balance) and correct FHP in Parkinson’s condition8,9,10. Therefore, we hypothesized to differentiate between the effect of resistance training and PNF to improve FHP in participants with Parkinson’s disease. So this randomized controlled trial was designed for assessing the effect of PNF techniques & strengthening exercise in forwarding head posture in patients suffering from Parkinson’s disease.
Material and Methods
The present study was a randomized control trial, with the flow diagram shown in Figure 1. The proposed study was done after moral endorsement from the Institutional Ethics Committee of the Department of Physiotherapy, Guru Jambheshwar University of Science & Technology, Hisar via letter-number PTY/2019/1014. This trial is also registered under the clinical trial registry of India (CTRI/2019/12/022415). Each participant of the study gave informed consent after an explanation of the procedure in their local language and we followed Helinski's 2000 declaration. All subjects had given verbal information about the purpose, risk & benefits of the study.
Study participants: 40 subjects fulfilled the eligibility criteria for the study. The Patient suffering from Parkinson's disease with forwarding head posture and CVA less than 500 should be included in the study. Patients with any metabolic disorders, heart disease, congenital anomaly of the cervical spine, and un-cooperative behaviour were excluded. Subjects were randomized and allocated into 2 groups: the experimental group (N=20) and the control group (N=20). The selection of the flow of participants was summarized in figure 1.
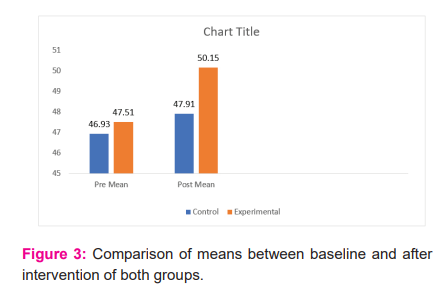
The outcome variable was non-significant at the start of the intervention. Post interventions reading of outcome variables after intervention were compared between the two groups using an independent t-test. The outcome measure shows significant improvement in the outcome variable.When we compared means (pre-post) of both groups, CVA increased significantly after 2 weeks (MD= 2.63; 95% CI -2.16 to -1.13; t38= -6.50; p<0.001).
First FHP was checked by photographic methods. The camera was placed 1.5m away from the participant for clicking the pictures. The good inter-rater reliability of the measurement of CVA in standing position was already proved.7 The subject was positioned in a standing position with shoes off with the camera faced on the right-hand side of the subject. The CVA was calculated between the intersections of a line drawn from the tragus of the ear to the spinous process of C7 with a horizontal line through C7.6 The outcome measure was calculated before the start of the intervention and after 2 weeks of the intervention in both groups. Baseline reading and post-intervention reading was used for final analysis.

The experimental group received the PNF (hold relax) technique in the upper limb and the control group received strengthening exercises of the upper limb to correct forward head posture. In the experimental group using the hold relax technique; from D1 flexion to D1 extension of upper extremity the PNF stretching was given. The hold-relax technique muscle was stretched isometrically, contracted 7–15 seconds & briefly relaxed 2–3 seconds. PNF stretching was given thrice a week for 2 weeks. The shoulder of the patient was placed in an extension, abduction, and internal rotation, the forearm in pronation, and the wrist and finger in extension. The therapist's hand is placed in the patient's palm to assume a firm grip of the patient's hand and the wrist has been moved into flexion and radial derivation. The therapist's second hand on the anteromedial aspect of the patient's arm just above the elbow. The movement was ended by taking the shoulder is in the flexed, adducted and externally rotated position, forearm pronation with and finger flexion along with radial deviation.11,12,13
In the control group, the first start with chin tuck was performed in a sitting or standing position. Sit up straight and watch directly above the shoulders with your ears. Ask the subject to put the finger on the chin. Pull the chin without moving the finger and head back until a good stretch is felt at the base of the head & at the top of the neck. Stretch was held for at least 5 seconds and 10 repetitions were advised.14,15 For strengthening exercise of shoulder retractors, the participants are positioned in optimal posture and asked to placed left arm behind the body and depress the shoulder tuck chin and slowly drew it right ear to the right shoulder, also was asked to rotate the neck upward toward the ceiling until a slight stretch was felt on the left side. Hold the position for 30 seconds and then repeat it in the opposite direction 10 times in a session.14,15 In the last, pectorals muscles stretching: Sit and stand with feet separated by hip-width with back straight. If there is a problem keeping the patients upright on the chair both shoulders should be squared with the body. Place the fingers behind the forehead. The elbows pointed outward. The back was straight and the patient's neck wasn't bent. Elbows moved backwards. The therapist moved the elbow; squeeze the shoulder blades together so that patient feels a good stretch in the chest muscle. Participants were asked to breathe and exhale deeply as the therapist hold stretch while in mind that the neck is straight. Hold the position for 15-20 seconds 10 times in a session.14,15
Data Analysis
Data were analyzed using the SPSS software (version 21). Descriptive statistics were driven by the mean and standard deviation for Cranio-vertebral angles (CVA). Normality for all variables was checked using the Kolmogorov-Smirnov test. The significance was determined at a p-value of <0.05. Paired t-test was used to compare pre & post-treatment values within the group and an independent t-test.was used for intergroup comparison.
Results
The trial started with 40 participants and in the experimental group, there were 20 participants, with a mean age of 63.25±9.17 and 20 participants in the control group, with a mean age of 63.20±5.79. 16 males and 23 females were included in the study. There were 20 participants (Male: 5 & Female 15) in experimental group and 20 (Male=10 & Female=10) in control group.
The T-test (paired) was used for determining the efficacy of resistance exercise on CVA variables after 2 weeks. CVA increased significantly after 2 weeks (MD= -.58; 95% CI -.83 to - .34, p<0.001). CVA also improved significantly after 2 weeks (MD= -2.23; 95% CI -2.70 to -1.76, p<0.001) in experimental group.


Discussion
This interventional study examined the effect of strengthening and stretching exercise and PNF stretching on FHP in a patient suffering from Parkinson's disease. The postural assessment was done with CVA (standing position) measurements also. The result of the study supports our hypothesis that PNF stretching is more effective as compared to strengthening exercise on FHP in Parkinson's disease. A significant improvement in CVA was found in both groups but the mean difference was more in the experimental group. The result of the study showed significant postural changes.
Parkinson's disease is the most common problem in FHP.6,7 It causes an increased lordosis of the lower cervical, extension of the middle cervical spine & flexion of the lower cervical spine. FHP can lead to cervical muscle imbalance.16
FHP is associated with weakness in the deep cervical short flexors and mid-thoracic scapular retractors, and shortness of the cervical extensors and pectoralis muscles.12 FHP can be corrected by restoring the normal muscle balance between agonist and antagonist muscles.16 An intervention protocol as a form of two strengthening (deep cervical flexors and shoulder retractors and two stretchings (Pectoralis and Sternocleidomastoid muscles) exercises can improve postural alignment shown by significant improvement of CVA.17
PNF is more effective in raising the range of the reciprocal activation of agonists and antagonist provides the improved muscle tendon. In the process of PNF, when the patients are asked to contract the muscles in the internal rotation against resistance, there is the development of muscle tension and inhibition of alpha motor neuron activity of GTO fibres and reduction of tension in muscle tendon. So, in the neuromuscular system, inhibition is a state of decreased neuronal activity and altered synaptic potential that impair the ability to contract muscles.18
The group that received PNF also showed recovery in movements of both left & right sides i.e. shoulder flexion, abduction, and external rotation in comparison to the static group. The hold relaxes the procedure improved the range of shortened muscle, which was lengthened to the point of the limitation or up to the extent of the comfort of the subject.14,15 The isometric contraction for 10 sec was followed by the voluntary relaxation of the tight muscle. Then limb was passively moved up to the elongation of the range limiting muscle (Kisner 4thed). The range of movements for shoulder external rotation was taken before and after 2 weeks of training. Holds relax and PNF stretching was effective in increasing the range of motion of the shoulder19. The result of the present study also supported the findings that the PNF group also showed improvement in FHP and movements of both rights and left shoulder i.e. flexion, abduction and external rotation when compared to the static group.
Conclusion
Hold relax technique of PNF is effective in improving the forward head posture of patients with Parkinson’s disease. Future researches are warranted to optimize the dose (like frequency, duration and repetitions) of the technique for the best possible results. Further, the hold relaxes technique can also be compared with the contract relax PNF technique in future studies.
Acknowledgement
The authors acknowledged the patients who participated in the study.
Conflict of interest
None is declared.
Financial support
The study did not get any financial support.
Authors Contribution
All the authors contributed to every segment of the manuscript like content, collection of data, writing, and analysis of data and formatting of data.
Punia S: Conceptualization; Formal analysis; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualization; Writing - review & editing.
Malik M: Conceptualization; Data collection; Formal analysis; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualization; Roles/Writing - original draft.
Singh V: Conceptualization; Data collection; Formal analysis; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualization; Roles/Writing - original draft
Bodwal K: Conceptualization; Data collection; Formal analysis; Investigation; Methodology; Roles/Writing - original draft; Writing - review & editing.
Kaur J: Conceptualization; Data collection; Formal analysis; Investigation; Methodology; Roles/Writing - original draft; Writing - review & editing.
References:
1. Lindsay KW, Bone I, Fuller G, Callander R. Neurology and neurosurgery illustrated. Edinburgh: Churchill Livingstone; 2010.
2. Borrione P, Tranchita E, Sansone P, Parisi A. Effects of physical activity in Parkinson's disease: A new tool for rehabilitation. World J Methodol. 2014 Sep 26;4(3):133-43.
3. Ball N, Teo WP, Chandra S, Chapman J. Parkinson's disease and the environment. Front Neurol 2019 Mar 19;10:218.
4. DeMaagd G, Philip A. Parkinson’s disease and its management: part 1: disease entity, risk factors, pathophysiology, clinical presentation, and diagnosis. Pharm Therap. 2015 Aug;40(8):504.
5. Borghammer P, Van Den Berge N. Brain-first versus gut-first Parkinson’s disease: a hypothesis. J Parkinsons Dis. 2019 Jan 1;9(s2): S281-95.
6. Ahmadi A, Maroufi N, Sarrafzadeh J. Evaluation of forwarding head posture in sitting and standing positions. Eur Spine J. 2016 Nov;25(11):3577-82.
7. Salahzadeh Z, Maroufi N, Ahmadi A, Behtash H, Razmjoo A, Gohari M, et al. Assessment of forwarding head posture in females: observational and photogrammetry methods. J Back Musculoskelet Rehabil. 2014 Jan 1;27(2):131-9.
8. Gholop A, Chitra J. A comparative study on the effectiveness of resistance training and PNF to improve balance in Parkinson’s patients - A randomized clinical trial. Int J Sci Res. 2014;3(7):1535-1539.
9. Carvalho EL, Queiroz IP, Queiroz IP, Batista IM, Maciel TD, Arêas FZ. Effects of proprioceptive neuromuscular facilitation on the functional independence measure in patients with Parkinson’s disease. Ther Posturology Rehabil J .2015 Nov 18;13.
10. Shah P. Effectiveness of PNF along with stair gait training on dynamic balance assessed by functional reach test in patients with idiopathic Parkinson’s Disease. Int J Yoga, Physioth Phys Edu. 2018;3(5):4-6.
11. Cho J, Lee E, Lee S. Upper thoracic spine mobilization and mobility exercise versus upper cervical spine mobilization and stabilization exercise in individuals with forward head posture: a randomized clinical trial. BMC Musculosk Disor. 2017 Dec;18(1):1-10.
12. Suvarnnato T, Puntumetakul R, Uthaikhup S, Boucaut R. Effect of specific deep cervical muscle exercises on functional disability, pain intensity, craniovertebral angle, and neck-muscle strength in chronic mechanical neck pain: a randomized controlled trial. J Pain Res. 2019;12:915.
13. David FJ, Rafferty MR, Robichaud JA, Prodoehl J, Kohrt WM, Vaillancourt DE, et al. Progressive resistance exercise and Parkinson's disease: a review of potential mechanisms. Parkinsons Dis. 2012 Jan 1;2012.
14. Kisner C. Therapeutic exercise foundation and technique. New York: Churchill Livingstone; 2002.
15. Yoshii F, Moriya Y, Ohnuki T, Ryo M, Takahashi W. Postural deformities in Parkinson's disease -Mutual relationships among neck flexion, fore-bent, knee-bent and lateral-bent angles and correlations with clinical predictors. J Clin Mov Disord. 2016;3:1.
16. Candace WY, Kennis CK, Evelyn KY, Jeffrey TH, Margaret LY, Hwang SS, et al. Effect of a 4-week Theraband exercise with PNF pattern on improving mobility, balance and fear of fall in community-dwelling elderly. J Korean Soc Phys Med. 2017 Nov 30;12(4):73-82.
17. Abdollahzade Z, Shadmehr A, Malmir K, Ghotbi N. Effects of 4 weeks postural corrective exercise on correcting forward head posture. J Mod Rehab. 2017 Apr 1:85-92.
18. Al Dajah SB. Soft Tissue Mobilization and PNF Improve Range of Motion and Minimize Pain Level in Shoulder Impingement. J Phys Ther Sci. 2014;26(11):1803-1805.
19. Bandekar M, Rao K. Effectiveness of Kinesiological taping and PNF stretching in students with forwarding shoulder posture. Int J Multidisc Res Develop. 2019;6(2):106-109.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





