IJCRR - 13(18), September, 2021
Pages: 112-116
Date of Publication: 26-Sep-2021
Print Article
Download XML Download PDF
A Rare Large Odontogenic Keratocyst of the Mandible: Surgical Management and a Long Term Follow Up of 10 Years
Author: Balani M, Ustad F, Bhavikatti SK, Abouzeid HL, Karobari MI
Category: Healthcare
Abstract:Introduction: The commonly found developmental cysts are the dentigerous cysts of the maxilla and mandible, which are often related to impacted third molar teeth in the mandible and impacted canines. Bilateral dentigerous cysts are rare and occur typically in association with a developmental syndrome or systemic diseases such as mucopolysaccharidosis and cleidocranial dysplasia. Case Presentation: The following is a report of management of a case of unusual bilateral, non-syndromic dentigerous cysts associated with right mandibular canine and first premolars and left mandibular canine and both premolars. The most unusual aspect of the case was that contrary to the radiologic appearance of a developmental dentigerous cyst and with permanent teeth impacted and deciduous teeth present in the oral cavity, histopathologic examination on the right side revealed an aggressive follicular odontogenic keratocyst which was mimicking a dentigerous cyst. The case had a long term follow up of 10 years. Conclusions: This case report strongly emphasizes the importance of the fact that the final diagnosis of an odontogenic cyst requires proper clinical, radiographic and histopathological coordination as was seen in the above case, failing which a diagnostic dilemma arises.
Keywords: Dentigerous, Follicular odontogenic keratocyst, Impacted, Bilateral, Segmental resection
Full Text:
Introduction
A dentigerous cyst is an epithelial-lined developmental cavity that covers the impacted tooth crown at the cementoenamel junction, the third molar in the mandibular and maxillary canine is most frequently involved. There is usually no pain or discomfort. When cysts are small, they are usually discovered in radiographic examinations that are taken to investigate other symptoms or a failure of tooth eruption, but when cysts enlarge there are asymptomatic facial swellings. The radiographs taken with the impacted tooth show the association of the crown with a radiolucent lesion (unilocular) having a sclerotic margin (well-defined). One common finding at the lesion is radicular resorption. Following the radicular cysts, the most common type of odontogenic cysts, dentigerous cysts are second. Which is approximately 24% of all true cysts in the jaws.1Furthermore, their incidence has been evaluated at 1.44 cysts for every 100 unerupted teeth amongst the general population. 2The treatment of choice will be the removal of the lesion and the involved teeth as the cyst size may keep increasing. 3Histologically, the cyst is lined by non-keratinized stratified squamous epithelium and the connective tissue is usually flat, but it often becomes highly irregular with inflammation, 4 The odontogenic keratocyst is a distinctive type of developmental odontogenic cyst with specific histopathologic features and clinical behaviour. 5
Keratocysts differ from other odontogenic cysts in that they have a biologically aggressive behaviour because of a high-proliferative activity of the lining epithelium, a tendency to expand along with bony cancellous spaces and a considerably high rate of recurrence.6 Keratocyst may impede the eruption of teeth, resulting in dentigerous appearance radiologically. Such lesions are frequently misdiagnosed as dentigerous cysts. Altini and Cohen introduced the term “follicular keratocyst” for this group of lesions.7
Because of the aggressive growth pattern and neoplastic nature of the OKC, it is now designated by the World Health Organisation (WHO) as a keratocystic odontogenic tumour (KCOT) and is defined as “a benign uni- or multicystic, intraosseous tumour of odontogenic origin, with a characteristic lining of parakeratinised stratified squamous epithelium and potential for aggressive infiltrative behaviour”.8
Follicular OKCs are relatively uncommon. They account for 25 to 40% of all the OKCs.9 This paper tries to emphasize the importance of multiplicity of appearance and occurrences wherein a very rare manifestation of the bilateral dentigerous cyst was initially diagnosed and only after histopathological and 3D-CT investigations a surprising diagnosis of follicular odontogenic keratocyst on one side and a dentigerous cyst on the other side was made. Another very rare and interesting finding was the presence of multiple impacted permanent teeth associated with cysts in a patient in the fifth decade of life.
CASE REPORT
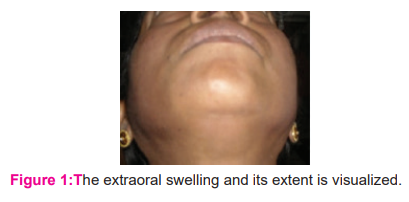
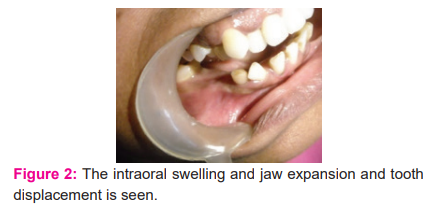
A 57-year-old female patient reported a complaint of swelling in the right lower jaw for 6 months. The swelling had gradually increased in size and there was associated pain since the last 2 months. Extra-oral examination revealed that the swelling extended anteriorly to about 1cm from midline in the right lower jaw region and posteriorly to about 2cm from the angle of the mandible, superiorly about 1cm above the corner of the mouth and inferiorly to the base of the mandible (Figure1). Intraoral examination revealed obliteration of the mesiobuccal fold in the right vestibule and swelling extended in the mandible from mesial aspect of right lateral incisor to mesial aspect of the right first molar (Figure 2).
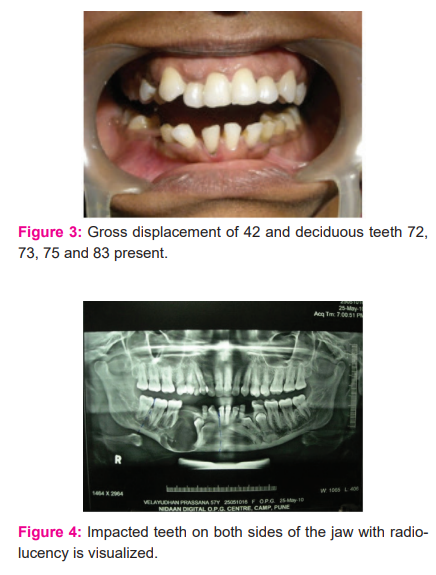
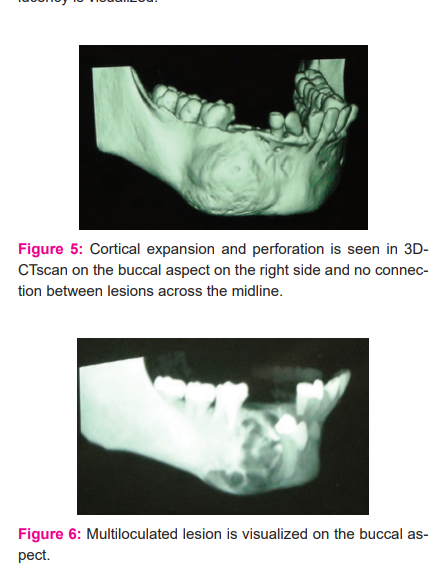
The mandibular right lateral incisor showed gross displacement. Despite the age of the patient, deciduous teeth were present (Teeth number: 72, 73, 75 and 83) (Figure 3). Palpation revealed a hard swelling. Aspiration was done and it yielded thick blood-tinged cream coloured fluid. Panoramic radiograph revealed unilocular radiolucency extending from distal aspect of tooth number 41 to mesial aspect of 46 with expansion and thinning of the lower border and impacted canine and premolar within the radiolucency. Tooth number 42 showed gross displacement and radicular resorption (Figure 4).
Another radiolucency on the other side of the midline was seen extending from the distal aspect of 31 to the mesial aspect of 36 but with no expansion or thinning of the lower border and presence of impacted canine and first and second premolars within the radiolucency. Displacement and radicular resorption of 31was observed(Figure 5).
A provisional diagnosis of bilateral dentigerous cysts associated with multiple impacted permanent teeth was made. Considering previous literature an incisional biopsy before actual surgery was planned for both sides under local anaesthesia and the specimen was sent for histopathology.
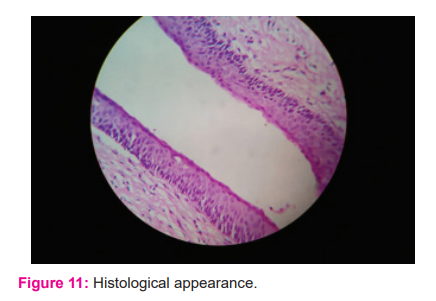
Surprisingly the report revealed typical cystic lining of uniform thickness (6-8 cell layer thickness) with corrugated parakeratinized stratified squamous epithelium with palisaded polarized basal cell layer giving a picket fence appearance and suggestive of odontogenic keratocyst on the right side. On the left side, the report revealed cystic lining with 2-3 cell layered thick non-keratinized stratified squamous epithelium. Retepegs were absent and the connective tissue showed inflammatory cell infiltrate suggestive of a dentigerous cyst.
Considering the presence of odontogenic keratocyst mimicking a dentigerous cyst a diagnosis of odontogenic keratocyst was arrived at. Since odontotogenic keratocysts are known to be aggressive and since delineation of the lesion at the midline was to be done to ascertain whether it was one lesion with the difference in histologic lining or two separate lesions a 3D-CT scan was advised.
3D-CT SCAN
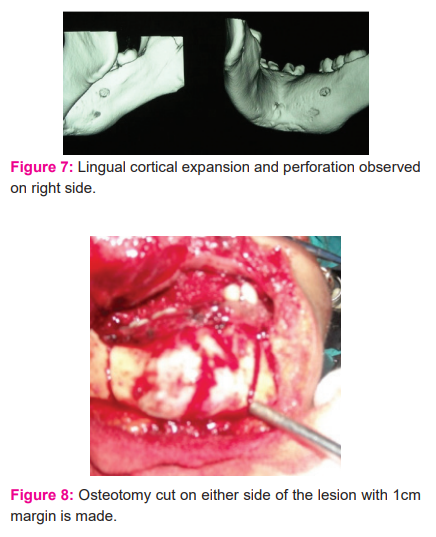
It revealed a highly expansile multilocular radiolucent lesion involving the right side of the mandible with expansion and perforation of both buccal and lingual cortical plates. Beyond the midline, the bone was intact with not much expansion or thinning and the two lesions were distinctly separate from each other with no connection at the midline( Figures 5,6,7).
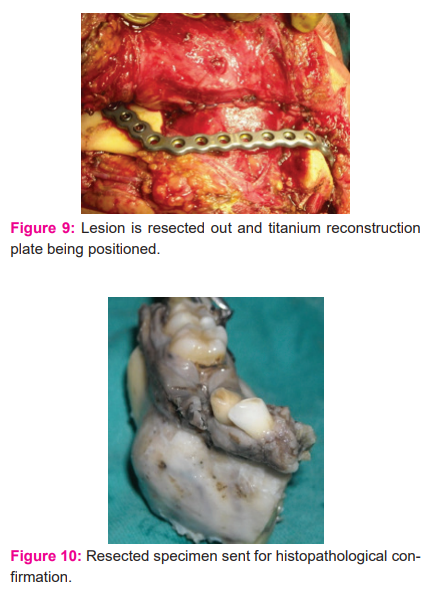
Considering the aggressiveness of the lesion and the chances of recurrence at a later age when the patient may not be able to withstand a major surgical procedure it was decided to go in for segmental resection (Figures 8,9,10) of the lesion on the right side and subsequent enucleation and curettage of the lesion on the left side considering the morbidity associated with the first procedure.
Histopathology report of the resected specimen confirmed the diagnosis of an odontogenic keratocyst with impacted teeth present within the cystic lumen and with cystic lining attached to the necks of the teeth (Figure 11). The patient was followed up for 10 years with no signs of recurrence. (Figure 12).
DISCUSSION:
Follicular odontogenic keratocysts were first described by Browne in the year 1970 as that which occurred when an enlarging OKC involved the follicle of an unerupted tooth and fused with the reduced enamel epithelium. He pointed out that in such cysts the epithelium immediately around the neck of the tooth was not keratinized and showed inflammatory changes in the underlying capsule.10
An odontogenic keratocyst may envelop an adjacent impacted tooth (envelopment keratocyst). Sometimes a true dentigerous cyst lining relationship might be similar when compared with an odontogenic keratocyst. 11
Altini et al termed this follicular primordial cyst (follicular keratocyst) and which may arise after the tooth eruption within the pre-existing keratocyst cavity similarly to that a tooth erupts into the oral cavity. 7,10,12,13
In a study done by Altini and Cohen in the year 1987, they were able to support their hypothesis in a series of experiments done on velvet monkeys, recipient sites were prepared by drilling holes in the alveolar bone and autogenous palatal mucosa was placed in them. In one of the animals killed after 52 weeks, the follicle of an erupting premolar tooth collided with one of the cysts, the lining of which became incorporated into the follicle, partly replacing the follicular reduced enamel epithelium and forming an integral part of this follicle of the erupting tooth.14 Thus, in the above case, on correlating all findings the confirmed diagnosis of a follicular odontogenic keratocyst was made.
CONCLUSION: This case report strongly emphasizes the importance of the fact that the final diagnosis of an odontogenic cyst requires proper clinical, radiographic and histopathological coordination as was seen in the above case, failing which a diagnostic dilemma arises. Very few case reports of follicular odontogenic keratocysts mimicking a dentigerous cyst and with concurrent existence of a dentigerous cyst in the same jaw in a patient in the fifth decade have been reported which makes this case a very rare occurrence.
CONSENT: Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
ACKNOWLEDGEMENTS: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
CONFLICTS OF INTEREST: Authors declare no conflict of interest with this paper
SOURCE OF FUNDING: None

References:
1. Daley TD, Pringle GA. The relative incidence of odontogenic tumours and oral and jaw cysts in a Canadian population. Oral Sur Oral Med Oral Patho 1994; 77:276-80.
2. Mourshed F. A roentgenographic study of dentigerous cysts. I. Incidence in a population sample. Oral Surg Oral Med Oral Pathol 1964; 18:47-53.
3. Motamedi MH, Talesh KT. Management of extensive dentigerous cysts. Br Dent J 2005; 198: 203–206.[CrossRef][Medline]
4.Shafer WG, Hine MK, Levy BM. A textbook of oral pathology, 4th ed. Philadelphia: WB Saunders; 1983;260-5
5. Neville, Damm, Allen, Bouquot. Oral and maxillofacial pathology 2nd edition. WB Saunders; 2016;636-8
6. Vered M, Buchner A, Dayan D, Shteif M, Laurian A. Solid variant of odontogenic keratocyst. J Oral Pathol Med. 2004;33(2);125-128.
7. Altini M, Cohen M. The follicular primordial cyst - Odontogenic Keratocyst. Int J Oral Surg. 1982; 11(3): 175-182.
8. Madras J, Lapointe H. Keratocystic odontogenic tumour: Reclassification of the Odontogenic keratocyst from Cyst to Tumour, J Can Dent Assoc. 2008; 74(2): 165a-165h.
9. Kim DK, Ahn SG, Kim J, Yoon JH. Comparative ki-67 expression and apoptosis in odontogenic keratocyst associated with or without an impacted tooth in addition to multilocular and unilocular varieties. Yonsei Med J.2003;44(5):841-846.
10. Browne RM. The pathogenesis of odontogenic cysts: a review. J Oral Pathol 1975 Jul; 4(1):31-46.
11. Hajj G, Anneroth G: Odontogenic keratocysts – a retrospective clinical and histologic study. Int. J.OralMaxillofac. Surg. 1996; 25:124-129.
12. Shear M. Cysts of the oral regions. 3rd ed, Wright, 1992:5-45.
13. Altini M, Cohen M. Experimental extra-follicular histogenesis of follicular cysts. J Oral Pathol.1987;16:49-52.
14. Altini M, Cohen M. Experimental extra-follicular histogenesis of follicular cysts. J Oral Pathol.1987;16:49-52.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





