IJCRR - 7(21), November, 2015
Pages: 47-52
Date of Publication: 11-Nov-2015
Print Article
Download XML Download PDF
DIGITAL DERMATOGLYPHICS IN CARCINOMA BREAST
Author: Vaishali Paranjape, Ashwini Kundalkar, P. Vatsala Swamy, Yashwant Kulkarni
Category: Healthcare
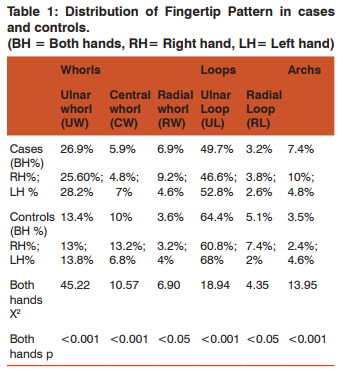
Abstract:Carcinoma breast is the second most common cancer amongst Indian women. Environmental factors, abnormal genetic background, mutations, hormones and changing lifestyle along with genes 17q21: BRCA1 and 13q21:BRCA2 have strong impact on in its etiopathogenesis. Dermatoglyphic patterns are determined by multiple genes and has multifactorial inheritance. Patterns are unique for every individual, remain unaltered throughout life, easy to record and can be studied by non invasive techniques. Methods: Digital dermatoglyphics of 100 histopathologically proven cases of Carcinoma breast were recorded, classified and compared with dermatoglypic patterns of 100 subjects not suffering from any clinically obvious genetic disease. Objective: To evaluate dermatoglyphics as a noninvasive anatomical marker of carcinoma breast. To find patterns most commonly associated with carcinoma breast. Results and Conclusions: Presence of an ulnar or radial whorl or an arch on six or more than six fingertips coupled with absence of a radial loop and central whorl is strongly associated with carcinoma breast. The most common pattern found in cases (49.70%) as well as controls (64.40%) was Ulnar loop (X2= 18.94, p< 0.001). Stastically significant decreased intensity of ulnar loops in patients with carcinoma breast was compensated by stastically significant increased intensity of ulnar whorls (26.90%) radial whorls (6.90%), Arches (7.4%). Fingertips of controls showed stastically significant increased frequency of central whorl
(10%) Radial loops (3.2%).
Keywords: Digital dermatoglyphics, Carcinoma Breast, Loops, Arches, Whorls
Full Text:
INTRODUCTION
Breast cancer is one of the most common and severe diseases encountered in clinical medicine. It is second most common cancer amongst Indian women; and an increasing trend in its incidence has been observed in most of metropolitan cities. 1 Population based epidemiological studies have shown that up to 10% of women all over the world will develop breast carcinoma in their life time. Further, the risk of developing breast carcinoma is increased up to 3 fold if a first degree relative is affected and up to 10 fold if more than one first degree relatives are affected.2There are other predisposing factors also,3 such as early menarche, late menopause, increased frequency in nulliparous than in multiparous, increased risk when the age at first child birth is over 30 years,4 obesity, intake of diet with high lipid content,5 exposure to exogenous estrogens, oral contraceptives,6 and also moderate alcohol consumption7 . Though the exact aetiopathogenesis of the breast cancer is not yet clear, the environmental factors (carcinogens) and hormones, along with an abnormal genetic background, seems to be the most common and possible explanation.2 Breast cancer is a genetic disease. This view is supported by (a) its familial tendency (b) identification of various mutations in tumor cells, for example mutation in gene –BRCA-1and BRCA-28 . Untreated cancers are always and invariably fatal. Hence early diagnosis (at in situ stage) and prompt treatment are important. Identification of people at increased risk of cancer before its development is an important objective of any cancer research8 and the study of dermatoglyphic patterns may provide a noninvasive and economical method to identify such people. This view is supported by Fuller (1973). He studied malignancy in general9 ; Ciovirnache M. et al (1986) 10, Edelstein J. et al (1991)11 have studied dermatoglyhphics in carcinoma thyroid patients and acute lymphocytic leukaemia respectively. Seltzer MH et al (1982)12 (1990)13 ; Abhilasha S et al (2014)14 studied the association between carcinoma breast and dermatoglyphics and strongly feel that dermatoglyphics may have a guiding future role in identifying carcinoma breast patients and also for those women who are at increased risk of its development. Considering these factors current study was undertaken with following aims and objectives: 1. Analysis and classification of the digital dermatoglyphic patterns in patients with carcinoma breast. 2. Compare it with normal subjects. 3. Correlate with previous studies. 4. Evaluate dermatoglyphics as a non invasive anatomical marker of carcinoma breast. 5. To find patterns most commonly associated with carcinoma breast.
MATERIAL AND METHODS
100 patients with carcinoma breast (The cases (gr-A)) were obtained from the Department of Surgery, BJ Medical college and Sasson General Hospital Pune. The diagnosis of all the cases of carcinoma breast was confirmed histopathologically. The control group (gr-B) consisted of 100 normal and healthy, perimenopausal and postmenopausal females less than 60 years of age; without any known genetic disorders, not giving history of cancer in the family, not suffering from hypertension, diabetes, schizophrenia, mental retardation or any other clinical illness having a genetic background. The detail case history was recorded in both the groups. The purpose of study was explained. Then proper information regarding the procedure and purpose of recording prints was given to members of both the groups who agreed for the study. After their consent, finger prints were taken. Fingerprints of both hands were taken using ink and pad method as described by Cummins and Midlo. After taking the prints, fingertip pattern were studied according to Bhanus (1991)15 classifications of digital patterns as follows:
Fingertip pattern
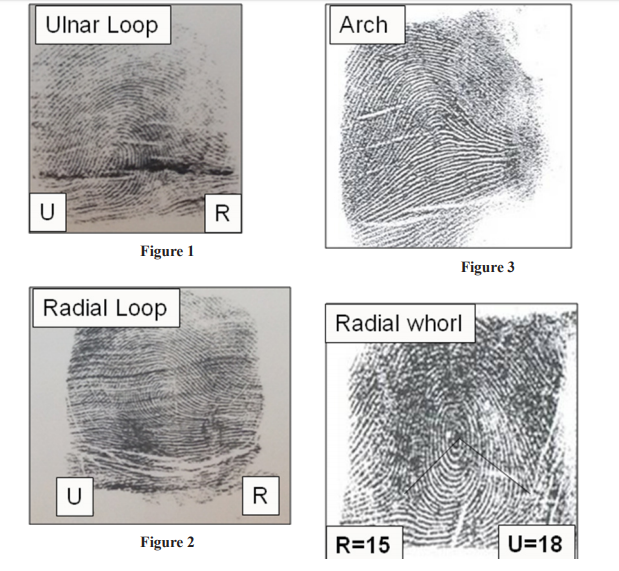
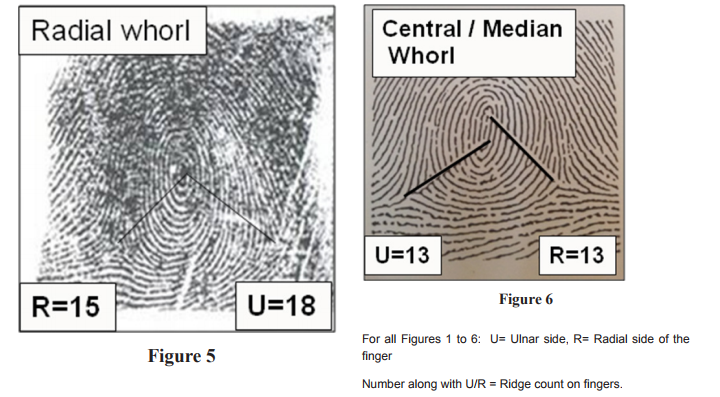
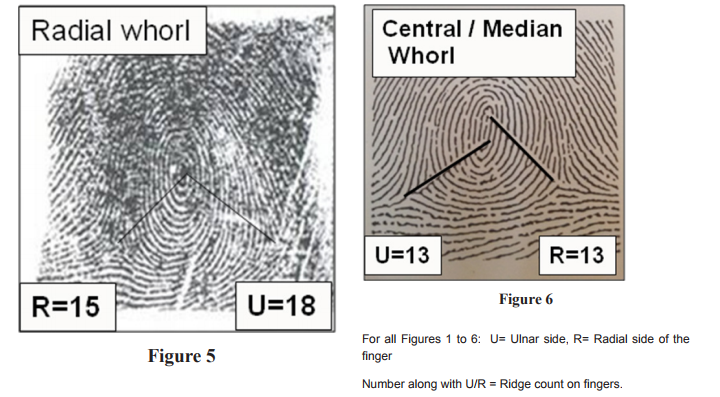
Loops: Series of ridges enter the pattern area on one side of the finger and exit from the same side. If the ridges enter and exit on the ulnar side of the finger it is an-ulnar loop (UL) and those from radial side of the finger are radial loops (RL). Loop has one triradius (ie : meeting point of three ridge lines). (Fig- Radial loop, Ulnar loop) Arches: Series of ridges enter the pattern on one side and exit from opposite side .At the centre of the pattern the ridges are slightly arched. Such pattern is called an arch. (Fig- Arch) Whorls: Ridges are arranged in the series of concentric rings. Whorls have two or more triradii. Whorls are further classified as radial, ulnar and central/median. If we consider left hand and trace the ridges from the centre of concentrically arranged pattern to periphery and the tracing shows clockwise alignment of ridges, it is an ulnar whorl (UW). If the alignment is in anticlockwise direction it is radial whorl (RW). Another way to classify a whorl, as radial, ulnar or median is by counting ridges. The centre of triradius and centre of whorl (core) are joined .The ridges crossing the line are counted from centre of the whorl to the triradius present on ulnar, as well as on the radial side of the finger. For example, If the ridge count is 10, from the centre to the triradius present on ulnar side and 15 from the centre to the triradius present on radial side, it is an ulnar whorl .If it is less on radial side than on ulnar side, it is radial whorl. If the count on both the sides (ulnar and radial) is similar, it is central /median whorl (C /M W). (Fig- Ulnar whorl, Radial whorl, Central/ Median whorl)
Statistical Methods:
Chi square test is used to assess the stastical significance of the data as fingertip pattern is a qualitative variable.
RESULTS
DISCUSSION
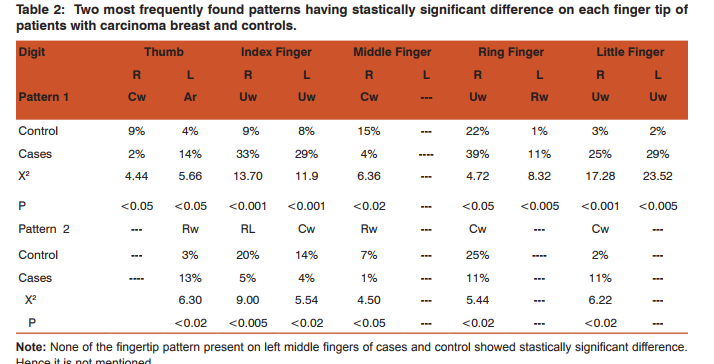
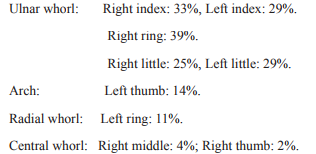
Ulnar loop is the most common pattern seen in less than 50% of the cases with carcinoma breast (49.7%) as compared to (64.4%) the controls. Ulnar whorls (26.9 %) are the second most commonly encountered pattern seen in carcinoma breast cases followed by Arches (7.4%). Radial whorl (6.9%), Central whorl (5.9%), Radial loops (3.2%) are the patterns encountered in decreasing order of frequency in women suffering from carcinoma breast. The highest frequencies of Patterns significantly associated with each fingertip in patients with carcinoma breast are as follows. (Table 2)
Dermatoglypic pattern seen on left middle finger of cases and controls does not show stastically significant difference. (Table 2) Observation of six or more whorls is seen in the studies conducted by Seltzer MH et al (1982)12 and (1990)13, Sakineh Abbasi et al (2006)16, Chintamani et al (2007)17, J. Lavanya et al (2012) 18, Abhilasha S (2013) 14. Sakineh Abbasi et al (2006) 16, quotes that “In 616 Iranian females studied, we have found a stastically significant difference of presence of digital whorl subtypes <6 out of 10 digits between cancer patients and controls and also between subjects with increased risk of developing cancer and controls; but not between the cancer cases and those with increased risk of developing cancer”. Chintamani et al (2007) 17 and Abhilasha et al (2013) 14 have found stastically significant difference in presence whorls on right ring and little finger between cases and controls. However everyone has not categorised whorls in to further subtypes as done in present study. Current study shows that presence of either an ulnar or a radial whorl is more crucial as it is seen associated with carcinoma breast. Central whorl is seen with higher frequency in controls. In our study, 15% controls versus 4% cases and 9% control versus 2% cases showed central whorls on right middle fingers and the right thumbs respectively. Thus central whorl is less frequently associated with carcinoma breast. Decreased frequency of central whorl is a relevant finding and hence has to be considered while screening; as it is not only the whorl but “which type of whorl” is important because increased frequency of ulnar and radial whorls is associated with cancer patients and central whorls with controls. In our study, Radial loops are less frequently associated with cancer cases (20% controls versus 5% cases and is seen commonly on right index finger) (Tables 1 and 2). Similarly decreased frequency of radial loops was seen on right thumb, left index, middle and left thumb of cases by Aparajita Raizada et al (2013) 19. Decreased number of radial and ulnar loops is found associated with carcinoma breast by S. B. Sukre et al (2003) 20 , Abhilasha et al (2013)14; P.E. Natekar et al (2006)21 found that six or more loops are significantly associated with carcinoma breast, but they have not mentioned if the loops are ulnar or radial. Loops are the most frequent pattern found in general population 22, 23, 24. The cases and controls are pooled from general population as they are a part of general population. In our study we have found decreased number of radial loops in cases than in patients with carcinoma breast. This is an important finding. Authors strongly recommend that, further classification of every pattern should be done. The study then would be more conclusive and hence beneficial. Our study shows presence of an arch with stastically significant difference on left thumb of cases (cases 14% versus control 4%). Chintamani et al (2007)17 found more arches on left digits of cases (cases 14.8% versus controls 6%). Arches were noted in 8% of the cases and 4% in controls by Abhilasha. S. et al (2013)14. This is in concurrence with our study. Arches being the least encountered pattern (0.4% in controls vs 0.7% in cases) are excluded from further analysis by P. E Natekar et al (2006) 21. Uduak Umana et al (2013) 25 studied 100 histolopatholgically proven cancer cases out of which only 18 had carcinoma breast and compared their Dermatoglyphic and Cheiloscopic findings with 126 normal subjects. They have found positive correlation between dermatoglyphics and carcinoma breast and negative correlation between cheiloscopic findings. This positive correlation even in a small study group warrants attention. All studies including the present one conducted till date have found positive correlation between carcinoma breast and digital dermatoglyphics. Sheltzer et al (1990)13 quotes that “the positive predictive value of 6 or more digital whorls is comparable to that of mammography and biopsy”.
CONCLUSION
Present study concludes that, presence of an ulnar or radial whorl or an arch on six or more than six fingertips coupled with absence of a radial loop and central whorl is strongly associated with carcinoma breast. In order to designate the finger tip patterns that would be pathognomonic of carcinoma breast, uniform system of classification should be used and larger sample size in different population groups needs to be studied. Since the study of digital dermatoglyphics is cost effective, non invasive and dermatoglyphic patterns remain unaltered throughout the life, dermatoglyphics thus definitely holds a promising future as far as screening of patients with increased risk of carcinoma breast is concerned.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors/ publisher/ of all those articles, journals, and books from where the literature for this article has been reviewed and discussed. This work would not have been possible without the guidance of Prof. Dr. B V Bhanu. (Retired Professor and Head, Department of Anthropology, University of Pune.)
References:
1. ICMR Bulletin Estrogens and breast cancer. 2003 Feb; 3(2): 13-24.
2. Cotran, Kumar, Robins: Robins Pathologic Basis of Disease. 4th Edition, W.B. Sunders International edition. 1192-1193.
3. Hulka, B.S. and Stark, A.T. Breast cancer: cause and prevention. Lancet. 1995; 346: 833.
4. Kelsey, J.L. Gammon, M.D. and Jhon, E.M. Reproductive Factors and Breast Cancer. Epidemiol Rev. 1933; 15:36.
5. Kuller, L.H. Eating fat or being fat and risk of cardiovascular disease and cancer among women. Ann Epidemiol. 1994; 4:199.
6. Wu, A.H. Pike, M.C. and Starm, D.O. Meta analysis: dietary fat intake, serum estrogens levels, and the risk of breast cancer. J Natl Cancer Inst. 1999; 91:529.
7. Miller, W.R. Estrogen and breast cancer: Biological considerations. Br Med Bull. 1990; 47: 470. 8. Robert L. Nussbaum, Roderick R. McInnes, Hungtington F. Willard, Thompson and Thompson Genetics in Medicine. 6th Edition. Genetics and Cancer. pp. 311-333.
9. Fuller, I.CInherited. Predisposition to cancer. British J of ca. 1973; 28:186.
10. Ciovirnache. M, Dumitru. L, Mogos. I, Spandonide. T, Damian. A, Handoca. A, Stoenescu. D, Dermatoglyphics in thyroid cancer. Endocrinologie. 1986; 24(3): 171-83.
11. Edelstein, J. Amylon,M. Walsh, J.A. Dermsatoglyphics and acute lymphocytic lukemia in children. Pediar Oncol Nur. 1991; 8(1):30-8.
12. Murray H. Seltzer, Chris C. Plato, Peter E. Engler, and H. Stephen Fletcher. Digital dermatoglyphics and breast cancer.Berast cancer research and treatment.1982; 2,261-265.
13. Seltzer, M.H. Plato, C.C. Fox, K.M. Dermatoglyphics in the identification of women either with or at risk for breast cancer. Am J Med Genet. 1990; 37(4):482-8.
14. Abilasha S, Harisudha R, Janaki CS. Dermatoglyphics: a predictor tool to analyze the occurrence of breast cancer. Int J Med Res Health Sci. 2014;3(1): 28-13.
15. Bhanu B. V. (1991).Digital patterns: A new classification system in dermatoglyphics today. B Mohan Reddy, S.B. Reddy, S.B. Roy, and B.N. Sarkar. (eds) Calcutta: 1-16.
16. Sakineh Abbasi, Nahid Einollahi, Nasrin Dashti, F. Vaez-Zadeh. Study of dermatoglyphic patterns of hands in women with breast cancer. Pak J Med Sci 2006 ; (22) 1 : 19-22.
17. Chintamani , Rohan Khandelwal, Aliza Mittal, Sai Saijanani. Amita Tuteja, Anju Bansal, Dinesh Bhatnagar and Sunita Saxena. Qualitative and quantitative dermatoglyphic traits in patients with breast cancer: a prospective clinical study. BMC Cancer 2007; 7:44.
18. J Lavannya, P Saraswathi, J Vijayakumar, S Prathap. Analysis of dermatoglyphc traits in patients with breast cancer. Journal of Pharmaceutical and Biomedical Sciences. 2012; 23(24): 1-5.
19. Aprajita Raizada, Vishwas Johri, T Ramnath, D S Chowdhary, R P Garg. A Cross-Sectional Study on the Palmar Dermatoglyphics in Relation to Carcinoma Breast Patients. Journal of Clinical and Diagnostic Research. 2013 April, 7(4): 609-612.
20. S.B. Sukre, A.A. Mahajan, A.G. Shroff. (2003) Dermatoglyphics in the identification of women either with or at risk for breast cancer. Paper presented at National Conference Anatomical Society Of India Dec 2003; Smt N. H. L. M. Medical College Ahmedabad.
21. P.E. Natekar, F. M. DeSouza, D.D. Motghare and A.K. Pandey. Digital Dermal Patterns in Carcinoma of Breast. Anthropologist .2006; 8(4): 251-254.
22. Oladipo GS, Paul CW, Bob-Manuel IF, Fawehinmi HB, Edibamode EI. Study of digital and palmar dermatoglyphic patterns of Nigerian women with malignant mammary neoplasm. J. Appl. Biosci.2009; 15: 829-34.
23. Daljit Singh, B.R.Prabhakar, Shivmohan Singh Bhalla Dermatoglyphic study in breast carcinoma. Indian J. Pathol Microbiol. 1979; 21: 27-32.
24. Nandy A. Identification of an individual In: Principles of Forensic Medicine. New Central Book Agency (P) Ltd. Calcutta. 2nd ed. (Reprint); 2001: 48- 111.
25. Uduak Umana, C.O. Ahunna, J.A. Timbuak, A.O. Ibegbu, S.A. Musa and W.O. Hamman. Dermatoglyphics and Cheiloscopic Patterns in Cancer Patients; A Study in Ahmadu Bello University Teaching Hospital (ABUTH), Zaria, Nigeria. Current Research Journal of Biological Sciences. 2013; 5(5): 220-225.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





