IJCRR - 13(13), July, 2021
Pages: 222-232
Date of Publication: 05-Jul-2021
Print Article
Download XML Download PDF
A Study on Occupational Health Hazards of Sanitation Workers in District Multan, Pakistan
Author: Muhammad Meesum Hassan, Naveed Farah, Saima Afzal, Abu Safian, Sidra Hussain
Category: Healthcare
Abstract:Introduction: An investigation into sanitation workers' lives was undertaken in the aftermath of the recent fatalities of manual scavengers in Pakistan. A few personal accounts of sanitation workers were used to illustrate their hardships. It's been more than a century since the working circumstances of these sanitation employees have altered much at all. Because of their employment, these employees are subject to specific health concerns in addition to the social horrors they confront. To name a few of the po�tential health risks: exposure to hazardous gases, cardiovascular disease problems, muscular-skeletal diseases, and infections Engineers, doctors, and legislators can help prevent this from happening through engineering, medical, and legislative methods. In addition to preventing exposures, the medical measures will aid in the early diagnosis of these exposures' consequences. Developing an effective occupational health service for this set of employees can help to achieve this. Aims: There should also be frequent awareness campaigns aimed at educating workers about safer work processes and the proper use of personal protective equipment. Methods: This study was the explanatory study by purpose because it explained the health hazards faced by the sanitation workers; by use, this was an applied study that will help the officials to provide necessary measures to escape the severe health hazards. Result: As a result of this, the researcher utilised Pearson and Spearman correlation to determine whether or not there is a link between Demographic information, Job Nature, and distinct Health concerns of sanitation employees. Conclusion: In addition to being subjected to occupational health dangers, sanitation employees are both socially and economi�cally disadvantaged. Infected cut wounds on sanitation workers were documented to be caused by bumping into sharp things, shattered glass, pins, sharp materials, and hazardous trash.
Keywords: Sanitation workers, Manual scavengers, Sewage workers, Septic tank cleaner, Job of hazards, Social humiliation
Full Text:
INTRODUCTION
When confronted with dirty toilets, overflowing septic tanks, or sewage-stained roadways, many of us are unaware of the importance of sanitation employees' work. We need a lot more of these employees to meet the ambitious goal of Sustainable Development Goals (SDG). Despite this, sanitation workers are generally unseen, and they labour in settings that expose them to the worst effects of poor sanitation, including severe illnesses, physical injuries, social humiliation, and even death in the course of their work.1 In the literature, sewage-exposed employees are typically referred to by several job names. A difference is made between employees at the sewage treatment facility and those who maintain the duct system, or sewer system. Often, they are referred to as sewer workers or sewage treatment facility personnel, respectively. There is no obvious difference between the varied labour duties performed by sewage employees and those who operate in other areas of the sewage system.2
It’s unfortunate that within Pakistan, janitorial work is highly stigmatized and reserved for individuals from low-income social classes. These janitors work in highly unhygienic, often life-threatening and working conditions. Every year, thousands of people in Pakistan lose their lives in gutters and manholes, due to exposure to poisonous gases and unhygienic waste materials. They don’t have access to safety equipment and supplies. As a result, they are always at risk of contracting illnesses such as hepatitis and TB, as well as smallpox and rabies. In terms of medical or safety support, workers are not compensated in any way.3 In cities, urbanisation has led to many sanitation issues, including a huge amount of waste, unclean streets, and clogged drains, all of which increase the sanitation employees' workload and working hours significantly. Sanitation employees are in charge of keeping the environment clean. As a result of inadequate resources in underdeveloped nations, the majority of the cleaning procedure in metropolitan areas is still done by hand. Garbage of all kinds is dumped on the streets due to poor waste material categorization at the source. Worker exposure to filth, infectious organisms and other dangerous items such as chemicals, animal excrement and sharp objects is a daily occurrence for sanitation personnel Sanitation employees are exposed to rain, snow, sand, cold, and UV radiation due to their outside employment. These variables have a negative impact on the sanitation employees' general health .4
The job of a sewer man includes several occupational risks that pose a serious threat to the worker's health and life. Accidental risks like gassing, injury, and immersion are common among sewer workers (flooding). Other health issues that affect them include occupational lung diseases, upper respiratory tract infection (URI), contact dermatitis, neurological problems such as headache and dizziness, eye problems such as burning or watering that can turn into redness, parasitic infections in the gut, and musculoskeletal problems such as fatigue and backache. Workers tended to have reduced lung function. 5 Sewer cleaning employees aren't properly trained, and the city doesn't enforce safety measures like wearing safety gear and utilising suitable equipment. They are inadequate for the employees even if it is provided, which leads to worker compromises and diseases and accidental fatalities. States often underreport the number of fatalities in these situations. Almost a century has passed since the working circumstances of sanitation employees changed.6
From permanent public or private employees with health benefits and retirement to some of the most marginalised and mistreated elements of society who take up low-grade and risky employment. It is financially unstable for individuals who work informally, with little compensation and minimal benefits. As a result of inadequate legal protection, a lack of or ineffective standard operating procedures, and lax enforcement of laws safeguarding their rights and health, sanitation employees often suffer. According to a comparative study of the instances, reducing the occupational health and safety concerns along the sanitation service chain (whether manual or mechanised) requires a systematic approach. 6,7
This study explored challenges faced by sanitation workers. In Pakistan with the advent of drainage machinery and trucks the manual scavenging and sanitation in Government departments is decreasing but this problem is persistent with the individual mobile sanitation workers who work individually without protective measures. Moreover, in congested urban areas, mechanized trucks cannot reach for sanitation purposes. A large part of the problems sanitation employees confronts stems from the fact that they are largely invisible in society. Only a small number of nations in the developing world have any kind of rules to safeguard these people. Governments may not have the financial or technological resources to implement laws, and the informality of positions creates further obstacles to implementation. Many more sanitation employees with safe, healthy, and decent working conditions will be needed in the future. To provide us with safe sanitation, employees who manage and maintain the sanitation services must have a safe and dignified working environment.
Understanding what sanitation hazards are is the first step in reducing them. It is important to avoid direct exposure to the hazards previously stated by taking sufficient health and safety measures. Sanitation risk assessment at the local level can identify the most important risks at each stage of the service delivery process Improved management practices, technology, and worker behaviour will be used to decrease exposure. PPE, such as gloves, full-body suits, boots, glasses, and gas detectors, are examples of suitable PPE. Included in this is also technology that will reduce the need for sanitation personnel to go into the pits or sewers. All personnel must be educated in the use of technology following standard operating procedures, and measures to guarantee they are followed must be in place to minimize hazards.
Sanitation employees should be given vaccinations, have regular health checks, and be covered by insurance, according to the findings of this study. As a result of this study, standard operating procedures and local-level sanitation standards may be established and approved at the city level. Training on occupational risks and the usage of personal protective equipment (PPE) are included, as well as safeguards for the employees' health and livelihoods. Monitoring of sanitation personnel' work and behaviour is required to ensure that standard operating procedures are followed. To safeguard the most vulnerable sanitation employees, standard operating procedures and standards that include manual emptying techniques are needed. However, informal, unlicensed, and temporary employees are more prone to violate the rules. Several systemic factors are at play in this situation: Caste and gender-based discrimination, a lack of technology alternatives, difficulties in implementing the legislation, entrenched behaviour that perpetuates the practice, and a lack of worker understanding of their rights and other employment opportunities are some of the obstacles that employees face.
Jaiswal away from the social horrors, these sewage employees are also subjected to various occupational health dangers such as exposure to toxic gases, drowning, musculoskeletal disorders, infections, skin difficulties and respiratory system issues as well as cardiovascular disease. Toxic gases that come from sewages and have a direct effect on the health of sewer workers such as hydrogen sulphide, carbon monoxide (CO), ammonia gas, carbon dioxide (CO2), and methane gas.7
Watt et al. researchers discovered that the majority of sanitation employees had sub-acute symptoms such as a sore throat, cough and chest discomfort. Dosage seems to be a factor in symptom severity. A year after the event, individuals who were more badly impacted are still unable to work due to deteriorating respiratory symptoms and lung function. Patil and Kamble survey and peak expiratory flow rate (PEFR) analysis were used to determine the occupational health risks of sanitation employees. In the workplace, workers were exposed to a variety of environmental and occupational risks that resulted in musculoskeletal diseases (85%), exposure to hazardous gases (65%), respiratory issues (45%), headaches (40%) and dermatological problems (35%).7,8 As a result, 90 per cent of the employees suffered from cough and colds, while 50 per cent had skin problems, 15 per cent had allergies, 15 per cent had malaria, and 15 per cent had typhoid, while 10 per cent suffered from bronchitis, lung difficulties, and hearing issues, etc.
Quansah investigated musculoskeletal problems. The common observations were bent backs, bent legs, heavy manual handling and the poor design of the workplace which was causing problematic working postures. Ntatamala, said sanitation workers are an occupational group commonly affected by shoe dermatitis.8
RESEARCH QUESTIONS
-
What are the challenges in executing the work?
-
What are the implications of the work on the social and health status of workers?
-
What are the typologies of sanitation work? What is the scale of the problem?
-
What is the level of knowledge of the workers about occupational hazards?
-
Is there a relationship between workers using personal protective devices and their health problems?
-
Is there a relationship between worker’s knowledge about occupational hazards and their health problems?
OBJECTIVES OF THE STUDY
-
Assessing the knowledge of the workers about occupational safety and health hazards related to Sanitation work.
-
Assessing the workers' health problems.
-
Assessing the workers' use of personal protective devices.
-
Assessing the worksite, environmental safety and hazards
THEORETICAL FRAMEWORK
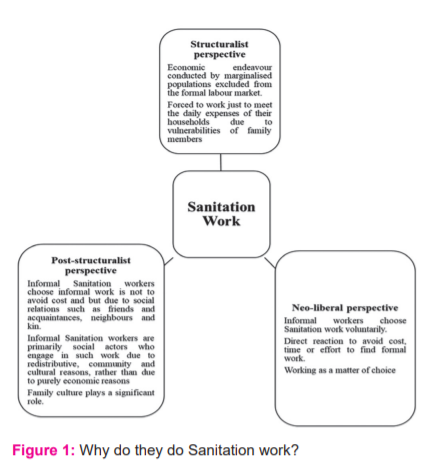
In the theoretical framework, researchers have made two general parts. In the first part, it is shown theoretically why the sanitation workers opt to choose this work as informal work. In the second part, it is showed with the help of theory that how a disease can be caused by any sociological phenomenon.
-
Structuralist perspective
Informal sanitation labour is seen as an economic activity carried out by underprivileged people excluded from the official employment market because they have no other choices. According to this definition, informal sanitation workers are persons who labour for low salaries in poor circumstances with no job security. Due to vulnerabilities such as disability, illness or accident, and the death of family members, sanitation workers are obliged to labour merely to pay the daily expenditures of their homes. In addition, family size and unemployment have a major influence on the poor salaries and exploitative working conditions of sanitation workers in general.
-
Neo-liberal perspective
Unlike structuralists, neoliberal researchers argue that informal labourers choose to work in Sanitation of their own. In this view, the rise of informal labour is regarded as a direct response to the need to avoid the expense, time, and effort of finding an official job. Because they choose to work in the informal sector, sanitation employees choose to do so.
-
Post-structuralist perspective
According to this view, informal workers participate in the informal sector willingly for reasons other than what neo-liberals claim. In contrast to neo-liberals, post-structuralists think that informal sanitation workers chose informal employment because of social ties, such as friends and acquaintances, neighbours and relatives. It is believed that informal sanitation workers are largely social actors who participate in such labour for redistributive, communal, and cultural reasons rather than for merely economic ones according to post-structuralist researchers. Children are inspired by their parents or other family members who are already involved in Sanitation work.9
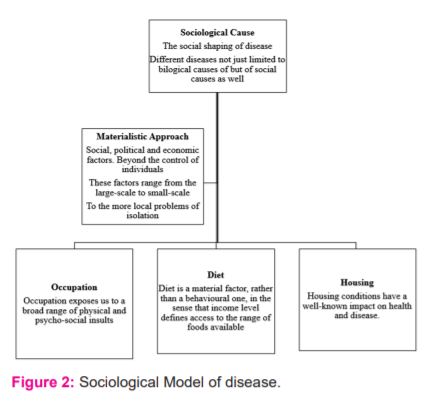
A Sociological Model of Disease
Prof. Peter Davis from Christchurch University in New Zealand is one of the sociologists who has created this type of illness model which emphasises social factors rather than disease mechanisms (Davis, 1994). While health research and policy should not focus just on individual diseases and bodies, Davis argues that they should be directed at the economic and political structures that create sickness rather than the individuals themselves. His categorization of sickness is therefore based on economic, social, cultural and political factors.
-
As a result of a capitalist economic system that prioritises profit over safety, the institution of the labour market would be blamed for industrial deaths and accidents.
-
Hypertension and mental illness would be studied as a result of the social moulding of disease through the institutions of family and kinship in the context of urbanisation and social mobility.
-
In obesity, bowel and lung cancer there are cultural variables of attitudes, practices, and lifestyles that express themselves in various consumption patterns - notably of nutrition and alcohol.
-
As a result of power structures and unequal participation rates in society, illnesses are a result of difficulties with access to services and fairness in-service distribution. 8,9,10
Materialist Approach
As a result, materialist theories of social inequality try to connect the biological and sociological aspects. In an attempt to isolate the role of material components in causing certain illnesses. Cancer, coronary artery disease, accidents and chronic obstructive pulmonary disease can all be linked to occupational and dietary factors as well as housing and environmental pollution (COAD). Each of these factors has a direct correlation to a person's job and income. In addition to providing greater access to housing and food choices, higher salaries can affect where a person resides within a city. Despite this, it is possible to isolate the elements experimentally.8
-
Diet
Eating habits are more of an economic decision as opposed to an emotional one. The availability of certain meals is determined by income level. Heart disease, stroke, and type 2 diabetes deaths can be increased by consuming too much or too little of specific foods and minerals.
-
Housing
Living conditions are determined by your economic level, rather than by your behaviour. Water leaks, inadequate ventilation, unclean carpets, and insect infestations in substandard housing can lead to a rise in mould, mites, and other allergens that are linked to poor health and disease. Poor infrastructure may be demolished, resulting in injuries and fatalities for those who depend on it.
-
Occupation
As a result of our jobs, we are subjected to a wide spectrum of physical and psychological abuse. Let's use cancer-causing chemicals as an example. Asbestos, for example, is an extremely high-risk sector where occupational exposure is the exclusive cause of cancer. An estimated 340 people died in 19 states and union territories owing to manual sewer and septic tank cleaning between 2012 and 2020, with Uttar Pradesh (52), Tamil Nadu (43) and Delhi (36) leading the list. In Maharashtra, there were 34 of these deaths .7
RESEARCH METHODOLOGY
An explanatory, cross-sectional survey research design was followed to investigate the Occupational Health Hazards of Sanitation Workers. The research was a quantitative study by the method. This study was the explanatory study by purpose because it explained the health hazards faced by the sanitation workers; by use, this was an applied study that will help the officials to provide necessary measures to escape the severe health hazards. Multan was the area of study. By population, it is the fifth-largest city and by area, it is the third-largest city in Pakistan. The universe of this study was all Sanitation Workers of Multan. The sample size was 150. For this study, both primary and secondary data were obtained. To obtain primary data, a survey and a structured interview schedule were used. It was decided to use the probability sample approach to choose the subjects after getting a list of registered sanitation personnel in the Town Municipal Authority. A non-probability sampling technique called handy sampling was used to determine the number of Mobile sanitation employees.
The researcher made 32 visits to the eight areas of Multan. On each visit, the researcher got data from 3 mobile sanitation workers.100 Mobile sanitation workers were included in the study while out of 150, Only 50 Government sanitation workers were available in WASA Office GolBagh which were included in the study. Researchers collected data from 20 sanitation employees to assess the questionnaire's reliability and validity. As a result of the workers' responses, it was decided to include open-ended questions. Stata for social sciences was used to analyse the collected data to codify, convert, and recode structures (SPSS-21). The researcher analysed all the possible variables through univariate i.e. Percentage and frequency and Bivariate analysis i.e. Pearson and Spearman correlation.
RESULTS AND DISCUSSION
Sanitation workers' demographic and health features were analysed using descriptive statistics. As a result of this, the researcher utilised Pearson and Spearman correlation to determine whether or not there is a link between Demographic information, Job Nature, and distinct Health concerns of sanitation employees
Univariate Analysis
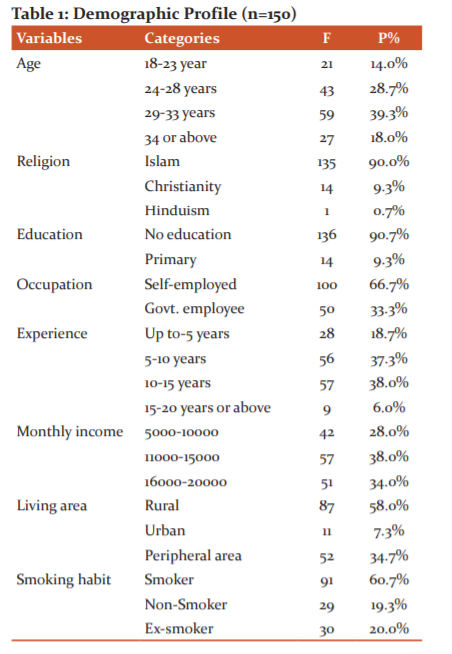
Table No.01 Demonstrates that The table is consisting of the responses of respondents in different strata of life that are discussed with different categories. The first one is the age structure of respondents. 14.0% of the respondents belong to the category of 18-23 years of age, 28.7% of the respondents belong to the category of 24-28 years of age, 39.3% of the respondents belong to the category of 29-33 years of age and 18.0% of the respondents belong to the category of 34 or above years of age. 100.0% of the respondents belong to the category of Males. As only male sanitation workers were the sample of this study.90.0% of the respondents belong to the category of Islam, 9.3% of the respondents belong to the category of Christianity and 0.7% of the respondents belong to the category of Hinduism. 90.7% of the respondents belong to the category of No education and 9.3% of the respondents belong to the category of Primary education. 66.7% of the respondents belong to the category of Self-employed and 33.3% of the respondents belong to the category of Government employee. 18.7% of the respondents belong to the category of 5 years of experience, 37.3% of the respondents belong to the category of 10 years of experience, 38.0% of the respondents belong to the category of 15 years of experience and 6.0% of the respondents belong to the category of 20 or above years of experience.28.0% of the respondents belong to the category of 5000-10000 Rs of income per month, 38.0% of the respondents belong to the category of 11000-15000 Rs of income per month and 34.0% of the respondents belong to the category of 16000-20000 Rs of income per month. 60.7% of the respondents belong to the category of Smoker, 19.3% of the respondents belong to the category of Non-smoker and 20.0% of the respondents belong to the category of Ex-smokers. 58.0% of the respondents belong to the category of Rural area, 7.3% of the respondents belong to the category of Urban area and 34.7% of the respondents belong to the category of Peripheral area as their living areas.
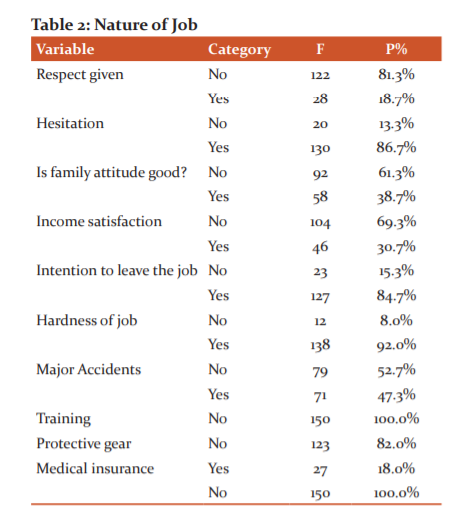
Table No.02 Demonstrates that 13.3% of the respondents belong to the category that they Feel No Hesitation while doing their job and 86.7% of the respondents belong to the category that they Feel Hesitation while doing their job. 81.3% of the respondents belong to the category that they are Not Given Respect for what they do and 18.7% of the respondents belong to the category that they Are Given Respect despite their profession. 61.3% of the respondents belong to the category that the attitude of their family/relatives is Not Good with them while 38.7% of the respondents belong to the category that the attitude of their family/relatives Is Good with them despite their profession. 69.3% of the respondents belong to the category that is Not Satisfied with their Income while 30.7% of the respondents belong to the category that Is Satisfied with their Income. 15.3% of the respondents belong to the category that has No Intention to Leave the job while 84.7% of the respondents belong to the category that Has an Intention to Leave the job. 8.0% of the respondents belong to the category that Does Not Perceive their job as a Hard job while 92.0% of the respondents belong to the category which Perceives their job as a Hard job. 52.7% of the respondents belong to the category that has no Major Accidents while doing the job while 47.3% of the respondents belong to the category that has Major Accidents while doing the job. 100.0% of the respondents belong to the category that they Never Received Training for their job. 82.0% of the respondents belong to the category that they Never use Protective Gears while 18.0% of the respondents belong to the category that they Use Protective Gears. 100.0% of the respondents belong to the category that they never had Medical Insurance.
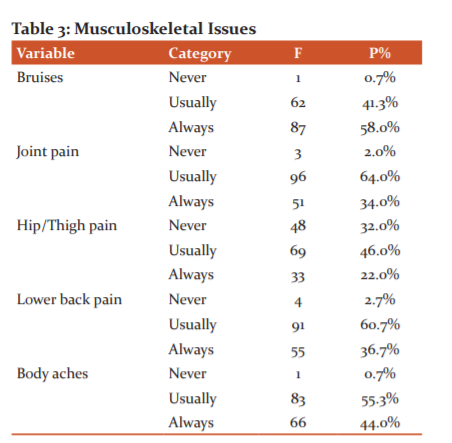
Table No.03 Demonstrates that 0.7% of the respondents belong to the category that Never had Bruises.41.3% of the respondents belong to the category that Usually had Bruises. And 58.0% of the respondents belong to the category that Always had Bruises. 2.0% of the respondents belong to the category that Never had Joint Pain. 64.0% of the respondents belong to the category that Usually had Joint Pain and 34.0% of the respondents belong to the category that Always had Joint Pain. 32.0% of the respondents belong to the category that Never had Hip/Thigh Pain. 46.0% of the respondents belong to the category that Usually had Hip/Thigh Pain and 22. 0% of the respondents belong to the category that Always had Hip/Thigh Pain. 2.7% of the respondents belong to the category that Never had Lower Back Pain. 60.7% of the respondents belong to the category that Usually had Lower Back Pain and 36.7% of the respondents belong to the category that Always had Lower Back Pain. 0.7% of the respondents belong to the category that Never had Body Aches.55.3% of the respondents belong to the category that Usually had Body Aches. And 44.0% of the respondents belong to the category that Always had Body Aches.
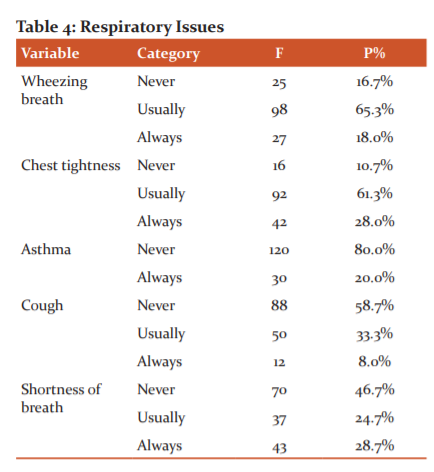
Table No.04 Demonstrates that 16.7% of the respondents belong to the category that Never had Wheezing Breath. 65.3% of the respondents belong to the category that Usually Had Wheezing Breath and 18.0% of the respondents belong to the category that Always Had Wheezing Breath. 10.7% of the respondents belong to the category that Never had Chest Tightness. 61.3% of the respondents belong to the category that Usually had Chest Tightness and 28.0% of the respondents belong to the category that Always had Chest Tightness.80.0% of the respondents belong to the category that Never had Asthma and 20.0% of the respondents belong to the category that Always had Asthma. 58.7% of the respondents belong to the category that Never had Cough. 33.3% of the respondents belong to the category that Usually had Cough and 8.0% of the respondents belong to the category that Always had Cough. 46.7% of the respondents belong to the category that Never had Shortness of Breath. 24.7% of the respondents belong to the category that Usually had Shortness of Breath and 28.7% of the respondents belong to the category that Always had Shortness of Breath.
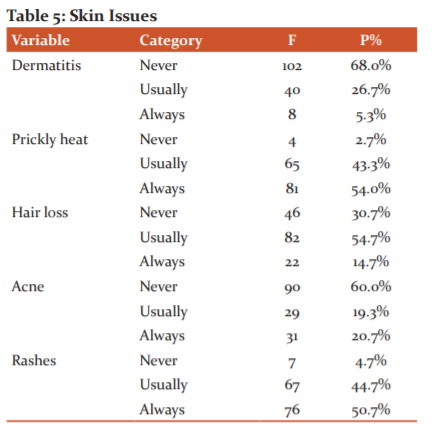
Table No.05 Demonstrates that 68.0% of the respondents belong to the category that Never had Dermatitis. 26.7% of the respondents belong to the category that Usually had Dermatitis and 5.3% of the respondents belong to the category that Always had Dermatitis. 2.7% of the respondents belong to the category that Never had Prickly Heat. 43.3% of the respondents belong to the category that Usually had Prickly Heat and 54.0% of the respondents belong to the category that Always had Prickly Heat.
30.7% of the respondents belong to the category that Never had Hair Loss. 54.7% of the respondents belong to the category that Usually had Hair Loss and 14.7% of the respondents belong to the category that Always had Hair Loss. 4.7% of the respondents belong to the category that Never had Rashes. 44.7% of the respondents belong to the category that Usually had Rashes and 50.7% of the respondents belong to the category that Always had Rashes.60.0% of the respondents belong to the category that Never had Acne. 19.3% of the respondents belong to the category that Usually had Acne and 20.7% of the respondents belong to the category that Always had Acne.
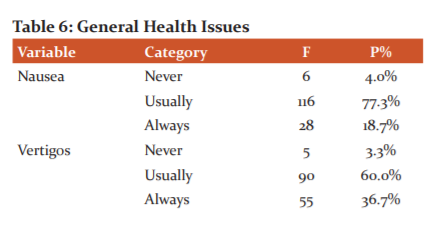
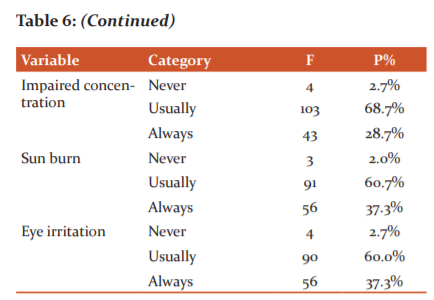
Table No.06 Demonstrates that 4.0% of the respondents belong to the category that Never had Nausea. 77.3% of the respondents belong to the category that Usually had Nausea and 18.7% of the respondents belong to the category that Always had Nausea. 3.3% of the respondents belong to the category that Never had Vertigos. 60.0% of the respondents belong to the category that Usually had Vertigos and 36.7% of the respondents belong to the category that Always had Vertigos. 2.7% of the respondents belong to the category that Never had Impaired Concentration. 68.7% of the respondents belong to the category that Usually had Impaired Concentration and 28.7% of the respondents belong to the category that Always had Impaired Concentration. 2.7% of the respondents belong to the category that Never had Eye Irritation. 60.0% of the respondents belong to the category that Usually had Eye Irritation and 37.3% of the respondents belong to the category that Always had Eye Irritation. 2.0% of the respondents belong to the category that Never had Sun Burn. 60.7% of the respondents belong to the category that Usually had Sun Burn and 37.3% of the respondents belong to the category that Always had Sun Burn.
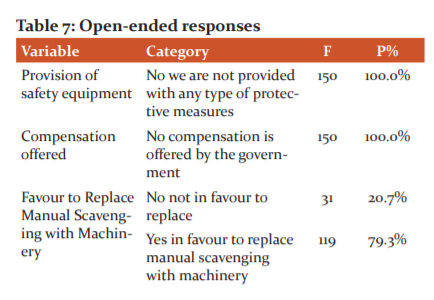
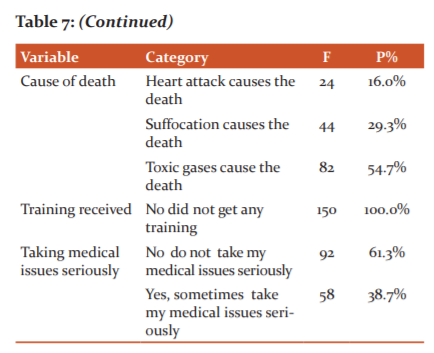
Table No.07 Demonstrates that 100.0% of the respondents belong to the category that No compensation is offered by the government. 20.7% of the respondents belong to the category that is not in favour to Replace Manual Scavenging with Machinery. And 79.3% of the respondents belong to the category that is in favour to Replace Manual Scavenging with Machinery. 16.0% of the respondents belong to the category that Heart attack causes death, 29.3% of the respondents belong to the category that Suffocation causes death and 54.7% of the respondents belong to the category that Toxic gases cause death. 100.0% of the respondents belong to the category that did not get any training.61.3% of the respondents to belong to the category that does not take their medical issues seriously and 38.7% of the respondents belong to the category that takes their medical issues seriously.
Bivariate Analysis
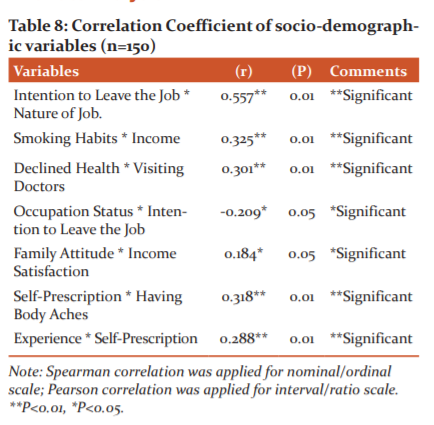
Table No.08 Demonstrates that The hypothesis for the first Spearman Correlation test was that Intention to leave the job and Nature of the job is positively correlated with each other. The value for the Spearman Correlation is 0.557** it was found significant with a significance value of 0.01. So it is concluded that there is a positive correlation between Intention to Leave the Job and Nature of Job. The researcher interpreted it as when the nature of Job is hard the intention to leave the job is also increased. From the nature of Job, it is showed that whether the sanitation workers perceived their job as a hard job or not. 92% of the respondents perceived that their job was hard in terms of work and health hazards related to their job and 84.7% were having an intention to leave the job. So the hardness of jobs in economic, social and biological contexts made them think to leave the job for better job opportunities.
The hypothesis for this Spearman's Correlation test was that Smoking Habits and Income are positively correlated with each other. The value for Spearman's Correlation is 0.325** it was found significant with a significance value of 0.01. So it is concluded that there is a positive correlation between Smoking Habits and Income. The researcher interpreted it as when the Income increases the smoking habit is also increased. From the bivariate analysis, it was showed that the higher the income the higher will be the tendency to smoke. If the income keeps on increasing the sanitation workers spend most of their income on smoking. While asking about, why do they smoke they said they use it as a source of coping strategy against stress and stigmatization. The percentage of smokers in the respondents was 60.7%. The smoking tendency was low in independent mobile sanitation workers as they had very low incomes.
The hypothesis for the Pearson Correlation test was that Declined Health and Visiting Doctors are positively correlated with each other. The value for the Pearson Correlation is 0.301** it was found significant with a significance value of 0.01. So it is concluded that there is a positive correlation between Declined Health and Visiting Doctors. The researcher interpreted it as when the Health has declined the visits to the doctors are increasing. From the results, it was revealed that the health problems of sanitation workers were quite high. 52.7% of the respondents revealed that their health was declining due to their job. Their health was deteriorating due to their profession so they visited doctors most often due to the nature of their job.
The hypothesis for the Spearman Correlation test was that Occupation Status and Intention to Leave the Job are negatively correlated with each other. The value for the Spearman Correlation is -0.209* it was found significant with significance value of 0.05. So it is concluded that there is an inverse correlation between Occupation Status and Intention to Leave the Job. From the nature of Job, it is showed that whether the sanitation workers are mobile sanitation workers or Govt. employees. Most of the workers were mobile sanitation workers which were unable to enjoy social security that is why the intention to leave the job was high among mobile sanitation workers as they were in search of a new good opportunity. The researcher interpreted it as when the Occupation status is increased i.e. from mobile sanitation worker to Government sanitation worker the intention to leave the job is decreased.
The hypothesis for the Pearson Correlation test was that Family Attitude and Income Satisfaction are positively correlated with each other. The value for the Pearson Correlation is 0.184* it was found significant with a significance value of 0.05. So it is concluded that there is a positive correlation between Family Attitude and Income Satisfaction. The researcher interpreted it as when Income satisfaction increases the family attitude becomes good. 69.3% of the respondents were not satisfied with their income so they and similarly 61.3% of the respondents perceived that their family behaviour was not good with them so the lower-income satisfaction and bad family attitude are significantly correlated which shows that if they had higher income levels the family attitude might get changed.
The hypothesis for the Pearson Correlation test was that Self-Prescription and Having Body Aches are positively correlated with each other. The value for the Pearson Correlation is .318** it was found significant with a significance value of 0.01. So it is concluded that there is a positive correlation between Self-Prescription and Having Body Aches. The researcher interpreted it as when Body aches increased the self-prescription also increased. The researcher explored that 44.0% of the sanitation workers were doing self-prescription because 55% were having body aches usually. They had no education and had low income which forced them not to go to the doctor and prescribe by themselves.
The hypothesis for the Spearman Correlation test was that Experience and Self-Prescription are positively correlated with each other. The value for the Spearman Correlation is 0.288** it was found significant with a significance value of 0.01. So it is concluded that there is a positive correlation between Experience and Self-Prescription. The researcher interpreted it as when the experience in sanitation job increased the habit of self-prescription also increased. 38.0% of the respondents had an experience of 10-15 Years and 44.0% had a habit of self-prescription so from Bivariate analysis there was found a significant correlation as when the experience in sanitation field gets increased the habit of self-prescription is also increased among the sanitation workers.
CONCLUSION
The majority of the respondents belong to the category of 29-33 years of age. All the respondents were male. Most of them were Muslim. The majority were Illiterate living in the Rural areas. Most of them were Self Employed as Mobile Sanitation workers independent of any Institution. The majority of them had 15 years of experience and an Income of Rupees 16000-20000. They were found to be Smoker. They Felt Hesitation while doing Sanitation jobs. Due to their profession majority of the respondents Perceived that their Family Attitude is not Good with them, they are not given Respect. Due to lack of social security and small income majority were not Satisfied with their Income. Respondents Perceived sanitation jobs as Hard Job which is why they had an Intention to Leave the Job. Mostly had no Major Accident at the workplace. All of them did Not Receive Training and did not use any Protective Gear. They had no Medical Insurance at all.
The majority of the respondents were Agreed concerning feeling Lethargic, feeling Anxious, getting Annoyed and having Medical Issues. Most of the respondents agreed concerning the Association of their job with Health Issues. They had a common Habit of Self-prescription and using Tranquilizers. The majority had the Perception of having More Medical Issues than Normal People and having a Declined in Health due to their profession. Most of them had a neutral response concerning Visiting Doctors often. Most of the sanitation workers always had Body Aches and Bruises. While Joint Pain, Wrist Pain, Shoulder Pain, Hip/Thigh Pain, Ankles/Feet Pain, Lower Back Pain, Upper Back Pain and Elbow Pain were usually observed. Wheezing Breath, Chest Tightness, Irritation of the Nose were usually observed in the majority of the respondents while they never had Dyspnea, Asthma, Cough, Lung Issues, Shortness of Breath, Allergic Rhinitis and Sinus Infection.
The major proportion of the respondents never had Dermatitis, Frostbite, Fissures, Varicosity, Acne, Hives and Pyrosis. While they usually had Hair Loss, Blisters, Prickly Heat and Rashes. The majority of Sanitation workers had Issues of Nausea, Vertigos, Impaired Concentration, Cold, Eye Irritation, Headache, Sun Burn, Blood Pressure Issues usually. While there was no obvious majority complaining have Heart Issues. Preventive Measures were not followed by the majority and they were not provided with Safety Equi
References:
-
Giri PA, Kasbe AM, Aras RY. A study on morbidity profile of sewage workers in Mumbai city. Int J Collab Res Intern Med Public Health. 2010; 2(12), 180-185.
-
Jaiswal A. Sewage Work and Occupational Health Hazards: An Anthropological Insight.
-
Jeggli S, Steiner D, Joller H, Tschopp. Hepatitis E, Helicobacter pylori, and gastrointestinal symptoms in workers exposed to wastewater. Occupational and environmental medicine, 2004; 61(7): 622-627.
-
Kelly SA. Reconstructing Social Housing: The Socio-spatial Effects of Welfare State Transformation in Toronto's Regent Park. University of Toronto (Canada).2008.
-
Quansah R. Harmful postures and musculoskeletal symptoms among sanitation workers of a fish processing factory in Ghana: A preliminary investigation. Int J Occup Saf Ergon. 2005; 11(2): 171-180.
-
The Hindu 340 sewer cleaning deaths in past 5 years: 2019 Government https://www.thehindu.com/news/national/340-sewer-cleaning-deaths-in-past-5-years-government/article33732992.ece
-
Tiwari RR.Occupational health hazards in sewage and sanitary workers. Indian J. Occup. Environ. Med.2008; 12(3):112.
-
Tsinda A, Abbott P, Pedley S, Charles K, Adogo J, Okurut K, Chenoweth J. Challenges to achieving sustainable sanitation in informal settlements of Kigali, Rwanda. Int J Environ Res. Public Health. 2013;10(12): 6939-6954.
-
Watt MM, Watt SJ, Seaton A. Episode of toxic gas exposure in sewer workers. Occupational and environmental medicine.1997; 54(4): 277-280.
-
World Bank, ILO, Water Aid, WHO. Health, safety and dignity of sanitation workers.2019.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





