IJCRR - 13(17), September, 2021
Pages: 88-91
Date of Publication: 12-Sep-2021
Print Article
Download XML Download PDF
Correlative Evaluation between Clinical and Pathological Diagnosis in Multinodular Goiter
Author: Abhay D. Havle, Kaenat Ahmed, Munnuru Khaleel Basha
Category: Healthcare
Abstract:Introduction: Multinodular goitre is an enlarged, diffusely heterogeneous thyroid tissue. Initial presentation may include diffuse enlargement, but asymmetrical nodularity develops later on. Objective: To correlate between clinical features, FNAC and histopathology findings in cases of multinodular goitre. As far as the Study Design is concerned it is a prospective observational study. Materials and Methods: All clinically diagnosed cases of multinodular goitre were included in the study. All cases underwent FNAC and subsequent thyroidectomy after routine pre-operative work up such as CBC, Urine, BT, CT, FT3, FT4 and ultra TSH, blood sugar, BUN and ultrasonography of neck etc. The surgical specimens of thyroidectomy were subjected to histopathological examination in all cases. Result: The commonest presenting symptom was neck swelling (100%) and associated pain (48%). The pressure symptoms on food, air passage and recurrent laryngeal nerve like dysphagia, dyspnoea and hoarseness of voice were noted in 42, 22, and 22 per cent of cases respectively with a mean 28.6\? 11.54. A significant association of these pressure symptoms was seen with colloid goitre (74%). Hyperthyroidism (14%) was in association with multinodular goitre. On fine needle aspiration cytology (FNAC) the most common finding was nodular colloid goitre 64%, followed by Hashimoto's thyroiditis 11% and follicular neoplasm 4%. On histopathological examination of the resected thyroid specimen, colloid nodular goitre was seen at 74% and Hashimoto's thyroiditis in 18%. 1 % of cases had papillary and follicular carcinoma each. Conclusion: Multinodular goitre was more common in females belonging to the age group of 30 to 40 years. The most common (48%) presenting symptom was swelling in front of the neck and associated pain. Pressure symptoms were significantly associated with colloid goitre. Associated hyperthyroidism was in (14%) multinodular goitre cases. The FNAC is a useful investigation for initial diagnosis in cases of multinodular goitre but it could not differentiate between follicular neoplasms. Therefore, histopathology remains an imperative investigation to rule out malignancy in multinodular goitre
Keywords: Multinodular Goitre, Presenting Complaints, Fine Needle Aspiration Cytology, Thyroidectomy
Full Text:
INTRODUCTION:
Multinodular goitre is an enlarged, diffusely heterogeneous thyroid tissue. Initial presentation may include diffuse enlargement, but asymmetrical nodularity develops later on. Iodine deficiency is a common cause. Initially, the patient is euthyroid; however, eventually, T3 and T4 levels get elevated and later may progress into a clinical hyperthyroid state or malignancy in the nodule. Ultrasonography (USG) and radioisotope scanning help to identify the heterogeneous thyroid substance in the goitre. Nodules with poor uptake of radioactive isotope- I131 or 128 suggest suspicion of malignancy.1-3 The possibility of malignant transformation of thyroid nodule in multinodular goitre is 5% to 10%.4 A variety of tests are carried out to know the anatomical and functional status of the thyroid gland. Fine Needle Aspiration Cytology (FNAC) is an established outpatient procedure useful in knowing the cytological status of thyroid neoplasia. According to American Thyroid Association and National Comprehensive Cancer Network, FNAC should be used as an initial test, because of its superior diagnostic reliability and cost-effectiveness, before both thyroid radioisotope study and ultrasonography.5 Similarly, the most sensitive imaging modality, high-resolution ultrasonography, is available for thyroid gland examination and associated abnormalities. USG in cases of thyroid disease, apart from being useful in interventional diagnostic procedures, is non-invasive, easily available, less expensive and without any ionizing radiation.6
The thyroid functions, i.e. whether the thyroid gland is underactive, overactive or normal cannot be assessed by the USG alone for which simultaneous thyroid function tests and subsequent radioactive isotope study may be required. Hyperthyroidism may be adequately controlled by drugs, but surgical management and histopathological examination of the resected tissue is preferred as it provides an insight as to whether total thyroidectomy would be needed additionally. Subtotal or total thyroidectomy is performed depending on the portion involved. Radioactive iodine therapy is reserved for the elderly who are part of poor operative risk.7 There are many studies conducted about the correlation between FNAC and histopathology of nodular goitre. This study about the correlation between clinical presentation, FNAC and histopathology in cases of nodular goitre was conducted at the rural tertiary care teaching hospital.
MATERIALS AND METHODS:
This is a prospective observational clinical study in cases of multinodular goitre, at the department of otorhinolaryngology of the tertiary care teaching hospital. A total of 100 cases of nodular goitre, irrespective of normal or abnormal thyroid status and having age above 20 years was included in the study. All cases presenting with diffuse enlargement or solitary nodule of the thyroid gland or pregnancy were excluded from the study. The diagnosis of multinodular goitre was based on findings of palpation during clinical examination in all cases. Further, all cases were subjected to T3, T4 and TSH tests, FNAC and ultrasonography of the neck apart from routine CBC(complete blood count), BT(Bleeding time), CT(Clotting time), Urine, blood grouping, x-ray chest and neck etc. Cases with hyperthyroidism were treated and brought to a euthyroid state before surgery. The resected specimen in all cases was further studied by histopathological examination.
STATISTICS METHODS:
A Chi-square test was used to find the significance of age, pain, dysphagia, dyspnoea, hyper/hypo / euthyroid status, hoarseness of voice etc. in the diagnosis of thyroid swelling. All data analysis had been done by using SPSS version 20.0.
RESULTS:
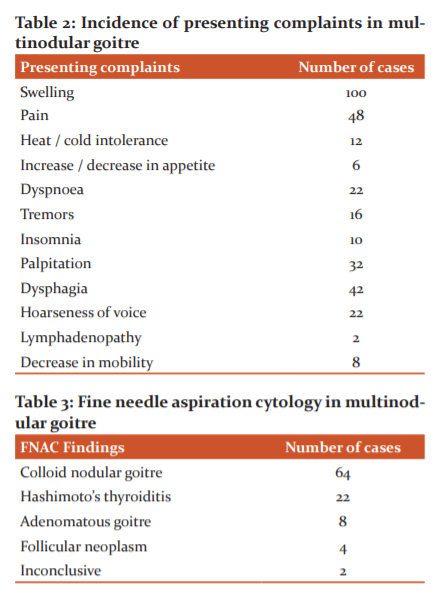
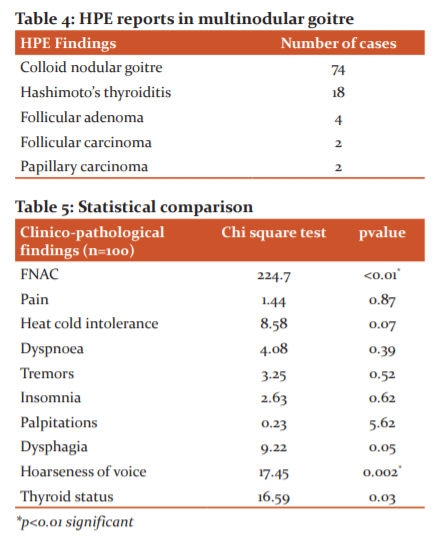
In this study total of 100 diagnosed cases of multinodular goitre without any initial evidence of malignancy were enrolled and subjected to clinical evaluation. The results of relevant investigations, Fine Needle Aspiration Cytology FNAC, the histopathological examinations of surgical specimens were compiled, analyzed. In table 1 Age distribution of multinodular goitre is presented. In table 2 Incidence of presenting complaints in multinodular goitre is presented. In table 3 Fine needle aspiration cytology in multinodular goitre is presented. In table 4 HPE reports in multinodular goitre presented. In table 5 Statistical comparison is presented. The females outnumbered males with M: F ratio of 6:94. The commonest age group was 30 to 40 years and the least common was above 60 years was with 6 females and 4 males. The mean age was 42.26 years ± 12.79. Amongst all cases the commonest associated symptom noted was a pain in neck swelling (48%). Followed by the symptoms due to pressure on food, air passage and recurrent laryngeal nerve noted were dysphagia (42%), dyspnoea (22%) and hoarseness of voice (22%) with an average of 28.6± 11.54. Out of these 42 cases having dysphagia, 20 had only dysphagia, 10 had hoarseness of voice and 12 had dyspnoea as associated symptoms. In 74 cases having colloid goitre the symptoms of dysphagia, dyspnoea, hoarseness of voice and hyperthyroidism were seen with p values 0.05, 0.03, 0.002 and 0.03 respectively. The number of cases of colloid goitre having dysphagia was 48 (35.13%), dyspnoea 15 (20.02%), hoarseness 12 (16.21%) and hyperthyroidism 14 (10.81%). Colloid nodular goitre was the most common finding on FNAC in 64 cases followed by Hashimoto’s thyroiditis 22, adenomatous goitre 8. FNAC was inconclusive in 2 of the cases. In 4 cases follicular neoplasm was found on FNAC who underwent total thyroidectomy to rule out malignancy. On histopathology of surgical specimen colloid, nodular goitre was the commonest finding in 74 of the cases, followed by Hashimoto’s thyroiditis 18, follicular and papillary carcinoma 2 and follicular adenoma 4. The histopathology revealed papillary carcinoma in one case which was inconclusive on FNAC and requiring a total thyroidectomy with nodal clearance at a second surgery.

DISCUSSION:
In this study of 100 cases, the majority were females with an M: F ratio of 6:94. In a similar study, Antonio Rios – Zumbudio et al in 2004 found it to be 11:89. The majority of the cases (33%) were from the age group 30 – 40 years and the least were having age above 60 years. All cases presented with neck swelling. 50% of the cases were having associated symptoms of pain. The mean percentage of the number of cases having symptoms due to pressure by neck swelling like dysphagia (42%), dyspnoea (22%) and hoarseness of voice (22%) was 27.3±9.428. Similarly in the study Rios Zumbudio et al., the average of pressure symptoms is 28.5%. Hyperthyroidism on presentation was found in 14% of cases of multinodular goitres in this study. And in a study of 301 cases of multinodular goitre by Rios- Zumbudio et al it was 22%. This difference maybe because it was presented at an early age in cases of this study as compared to one carried out amongst the western population. In this study out of 100 cases 52% were involving right lobe followed by 44% left lobe and 4% bilateral which correlates with the study by Chakravarthy et al (2017) wherein out of 290 cases 55.1% were involving the right lobe, 40.7 % were left and 4.1% bilateral. One case having multinodular of one lobe with largest measuring 0.7 cm underwent right lobectomy and at 3 months of follow up the opposite lobe was normal. Seven cases involved to left lobe and 4 that involved the right underwent subtotal thyroidectomy. Two cases underwent subtotal thyroidectomy as the initial FNAC was inconclusive. Based on the HPE of the surgical specimen that revealed papillary carcinoma and follicular adenoma, total thyroidectomy was performed in these 2 cases. Therefore, in all 11% underwent subtotal thyroidectomy, 1% right lobectomy and 88% underwent total thyroidectomy. The goitre was confined to the thyroid gland in 90% of cases. Out of the remaining 10%, 8% had a malignant transformation and restricted mobility of thyroid swelling and/ or 2% associated cervical lymphadenopathy which is comparable to 7.9% and 4.1% respectively in the above-mentioned study by Chakravarthy et al.The FNAC finding of the 100 cases revealed nodular colloid goitre in 64% followed by Hashimoto’s thyroiditis 22%, adenomatous goitre 8%, follicular neoplasm 4%and inconclusive in 2%. Cases with follicular neoplasm underwent total thyroidectomy to rule out malignancy. The histopathological examination of the resected specimen revealed colloid nodular goitre in 37% of the cases and Hashimoto’s thyroiditis in 18%. 1 case of follicular neoplasm on FNAC that was operated on turned out to be follicular carcinoma (Hurthle cell variant) on HPE of the specimen. Out 2 cases with inconclusive on FNAC 1 turned out as papillary carcinoma and another follicular adenoma on histopathological examination of the specimen. In all, there were 4 cases of follicular adenoma, 2 cases of follicular carcinoma and 2 cases of papillary carcinoma. Incidence of malignancy in multinodular goitre accounts for 4% which is comparable to the studies by Gondolfi et al. (2004) who had a result of 6.7% in a retrospective study of 81cases, but 1.21% in a study conducted by Nandedkar et al. in 2018. This is probably due to the larger sample size of the study (606) over a long duration (10 years). This study also included all cases of thyroid swellings such as solitary nodular goitre or thyroglossal cyst whereas the present study is focused only on clinically diagnosed cases of multinodular goitre.
CONCLUSION:
Females were the commonest sufferers of multinodular goitre with an M: F ratio of 6:94. The commonest age group was 30 to 40 years amongst all cases of multinodular goitre. Pressure symptoms were significantly associated with colloid goitre. Hoarseness of voice was a significant pressure symptom in 22% of cases of multinodular goitre. FNAC finding of multinodular goitre was significantly useful in making the initial diagnosis. FNAC conclusion of follicular neoplasm could not differentiate further between follicular adenoma and carcinoma therefore histopathological examination to rule out malignancy becomes mandatory. Other symptoms like dysphagia, dyspnoea, tremors, insomnia, palpitation and change in appetite or intolerance to change in temperature were seen in cases suffering from a multinodular goitre but their number was not statistically significant. The presence of cervical lymphadenopathy, as in 2 cases of this study of multinodular goitre, needs to be considered as malignant secondaries arising from the thyroid unless proved otherwise. Similarly, reduced mobility of the gland with irregular margins as in 8 cases of the study to be kept in mind as the possibility of malignancy, however, which was not statistically significant. Even though FNAC is reliable in determining the treatment plan, histopathological evaluation of surgical specimens must be undertaken for confirmation in all cases.
CONFLICT OF INTEREST: There is no conflict of Interest
SOURCE OF FUNDING: No Source of Funding
AUTHORS CONTRIBUTION: This is a collaborative work among all authors. Abhay D. Havle and Kaenat Ahmed performed the statistical analysis, wrote the protocol, and wrote the first draft of the manuscript. Kaenat Ahmed along with Munnuru Khaleel Basha managed the literature searches. All authors read and approved the final manuscript.
References:
1. Pang HN, Chen CM. The incidence of cancer in nodular goitres. Ann Acad Med. 2007;36:241-3.
2. Belfiore A, La Rosa GL, Padova G, Sava L, Ippolito O, Vigneri R. The frequency of cold thyroid nodules and thyroid malignancies in patients from an iodine-deficient area. Cancer. 1987;60:3096-102.
3. Mazzaferri EL, de Los Santos ET, Rofagha-Keyhani S. Solitary thyroid nodule: Diagnosis and management. Med Clin North Am. 1988;72:1177-211.
4. ul Haq RN, Khan BA, Chaudhry IA. Prevalence of malignancy in a goiter-A review of 718 thyroidectomies. J Ayub Med Coll Abbottabad. 2009; 21:134-6.
5. Tan H, Li Z, Li N, Qian J, Fan F, Zhong H, Feng J, Xu H, Li Z. Thyroid imaging reporting and data system combined with Bethesda classification in qualitative thyroid nodule diagnosis. Med. 2019;98:50(e18320).
6. Chaudhary V, Bano S. Imaging of the thyroid: Recent advances. Indian J Endocrinol Metab. 2012;16:371–6. [PMCID: PMC3354842] [PubMed: 22629501]
7. Al-Qurayshi Z, Randolph GW, Srivastav S, Kandil E. Outcomes in endocrine cancer surgery are affected by racial, economic, and healthcare system demographics. Laryng. 2016;126:775-81.
8. Zambudio AR, Rodríguez J, Riquelme J, Soria T, Canteras M, Parrilla P. Prospective study of postoperative complications after total thyroidectomy for multinodular goitres by surgeons with experience in endocrine surgery. Ann Surg. 2004;240:18-25.
9. Ríos A, Rodríguez JM, Canteras M, Galindo PJ, Tebar FJ, Parrilla P. Surgical management of multinodular goiter with compression symptoms. Arch Surg. 2005;140:49-53.
10. Chakravarthy NS, Chandramohan A, Prabhu AJ, Gowri M, Mannam P, Shyamkumar NK, et al. Ultrasound-guided fine-needle aspiration cytology along with clinical and radiological features in predicting thyroid malignancy in nodules ≥1 cm. Indian J Endocr Metab. 2018;22:597-60
11. Gandolfi PP, Frisina A, Raffa M, Renda F, Rocchetti O, Ruggeri C, et al. The incidence of thyroid carcinoma in multinodular goitre: Retrospective analysis. Acta Biomed. 2004;75:114-7.
12. Nandedkar SS, Dixit M, Malkani K, Varma AV, Gambhir S. Evaluation of thyroid lesions by fine-needle aspiration cytology according to Bethesda system and its histopathological correlation. Int J App Basic Med Res. 2018;8:76-82.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





