IJCRR - 13(17), September, 2021
Pages: 80-83
Date of Publication: 12-Sep-2021
Print Article
Download XML Download PDF
Multiple Myeloma Presenting as Fatal Hyperviscosity Syndrome: A Rare Case Report
Author: Jahnabi Bhagawati, Abhijeet Kumar Agrawal, Sunil Kumar, Sourya Acharya
Category: Healthcare
Abstract:Introduction: Hyperviscosity syndrome is regarded as a rare oncological emergency with a bleak prognosis. Though it is more commonly found in patients of Waldenstrom's macroglobulinemia and only 2-6% cases are reported in multiple myeloma. Aim: To highlight the therapeutic burden vindicated by Hyperviscosity syndrome over a case of multiple myeloma. Case Report: A 46-Year-old male patient presented to the emergency department with a history of two episodes of epistaxis with a mild headache for a few hours. The patient gave a history of bony pain at night. On investigation, the patient's complete blood count revealed Hb-1.2g/dl, TLC-6300 cells, platelet count -77 lakhs/cu mm) and Peripheral smear-showed RBC in rouleaux formation. Bone marrow showed myeloma cells. X-ray skull [lateral view] showed punched-out lytic lesions. Urine examination showed no Benz Jones proteins. Hyperviscosity syndrome ultimately leads to the patient's demise. Methods: We are reporting a case of multiple myeloma in a 46-year-old male who presented with epistaxis and acute kidney injury as part of Hyperviscosity syndrome. The database was searched from google, PubMed, Scopus and web of science. Conclusion: This case report represents the minority of multiple myeloma patients. This case report represents the minority of multiple myeloma patients. Hyperviscosity syndrome presents as a significant touchstone when dealing with patients with multiple myeloma and the complications following HVS can be often fatal while the patient may present with varied clinical features each separate time.
Keywords: Hyperviscosity syndrome, Waldenstrom’s macroglobulinemia, Multiple Myeloma, Epistaxis, Acute Kidney Injury
Full Text:
Introduction
Among plasma cell neoplasms, the most common is multiple myeloma. Other included neoplasms are MGUS (monoclonal gammopathies of unknown significance), plasma cell leukaemia, and plasmacytomas. Plasmacytoma is a localized form of neoplasm that is further classified into SPB (solitary plasmacytoma of bone) and EMP (extramedullary plasmacytoma) with each of them forming only < 4% of neoplasm burden whereas multiple myeloma forms the systemic disease.1 Multiple myeloma, a neoplastic lymphoproliferative B-cell systemic malignant disease depicts non-prohibited plasma cell (monoclonal) proliferation inside bone marrow resulting in flooding of peripheral blood with immunoglobulins that are non-functional.2
Blood Hyperviscosity Syndrome (BHVS) encompasses clinical features due to increased blood or plasma viscosity.3HVS presents with a classical triad of neurological manifestations, visual disturbances, and mucosal bleeding. Universal findings in cases of HVS would be epistaxis, oral bleeding, and visual symptoms. Evaluation of patients with Hyperviscosity syndrome must include a clinical history of any haematological disease or a similar disorder that runs in family. Impaired platelet function gives rise to bleeding in the form of Gastrointestinal bleed or epistaxis. The neurological manifestations are due to impaired blood supply to the central nervous system, the peripheral nerves however are affected due to paraproteins getting deposited in their myelin sheath. Patients show easy bruising with characteristic evidence on retinal examination (thick veins, haemorrhages, and papilledema). Patients may develop visual symptoms in the form of a sudden loss of vision, blurred vision, etc. Patients may also show signs of cardiac dysfunction in the form of valvular dysfunction, shortness of breath, myocardial infarction, and high output cardiac failure. The hypoperfusion of kidneys may lead to acute kidney injury (AKI).3 Few case reports are available about multiple myeloma and Hyperviscosity syndrome, but no reports are available regarding this syndrome presenting as fatal epistaxis and acute kidney injury.4,5 We are reporting a case of multiple myeloma in a 46-year-old male who presented with epistaxis and acute kidney injury as part of Hyperviscosity syndrome.
Case report
A 46-Year-old male patient presented to the emergency department with a history of two episodes of epistaxis with a mild headache for a few hours. The patient gave a history of bony pain at night. The patient had no other relevant history in the form of fever, cough, vomiting, loss of consciousness, seizures, head trauma, etc. The patient had similar episodes 2 days back. The patient was initially admitted to the ENT (Oto-rhino-laryngology) department where nose packing with supportive management was given. No Oro-pharyngeal cause could be found to explain the epistaxis. Hence patient was transferred to the medical department for further evaluation.
On examination-patient was conscious, oriented, afebrile with a pulse rate of 102/min, blood pressure of 100/70 mm of Hg in right arm supine position, and a respiratory rate of 22 cycles per min. JVP was not raised, the hepatojugular reflex was negative. Mild Pallor was present, no icterus, cyanosis, pedal oedema, lymphadenopathy. On systemic examination, cardiovascular examination revealed s1s2, respiratory system -no basal rales in bilateral lung fields, abdominal examination showed no splenomegaly, and the patient had no focal neurological deficit.
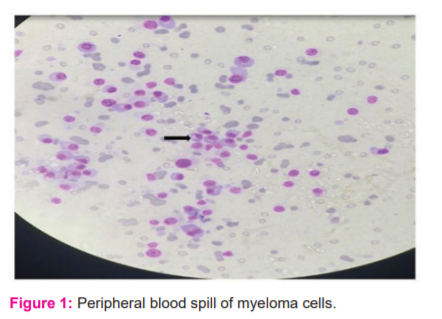
On investigation, the patient's complete blood count revealed Hb-1.2g/dl, TLC-6300 cells, platelet count -77 lakhs/cu mm) and Peripheral smear-showed TLC-6300cells/cu mm, DLC-Polymorphs 57%, lymphocytes 27, eosinophils-02% and monocytes-01% with RBC in rouleaux formation which gave a false impression of anaemia. There was a high suspicion of myeloma cells. Bone marrow showed myeloma cells. The repeat peripheral smear was suggestive of peripheral blood spill of myeloma cells (fig1) Other investigations -ESR-127mm (Westergren)in 1st hour Other relevant investigations revealed punched out lytic lesions on X-ray skull (lateral view), urine examination showed no Benz jones proteins and Hypercalcemia was present. Initial blood urea-160, serum creatinine -5.4. Liver function test showed Total bilirubin -1.3 mg/dl, serum protein-8.3 mg/dl, albumin-2.7mg/dl, globulin-5.6mg/dl.
Specific investigations about multiple myeloma like serum protein electrophoresis showed a small M band, serum-free light chain showed kappa free light chain -19.1, and lambda free light chain -37.
Following the above investigations, the patient was diagnosed to have multiple myeloma with Hyperviscosity syndrome. For the management of Hyperviscosity, the patient was put on extensive intravenous fluid therapy and side by side patient was counselled for plasmapheresis and chemotherapy. For 2 – 3 days patients' urine output started showing decrement and blood urea rose to 200 mg/dl and serum creatinine peaked to a value of 12.5 mg/dl signifying acute kidney injury. Subsequently, the patient was planned for hemodialysis. During the process of dialysis catheter insertion, there was frequent catheter blockage due to increased blood viscosity and the same could not be rectified even after copious heparinization of a dialysis catheter. Similar problems were encountered during future venipuncture for monitoring renal status.
Intractable acute kidney injury (persistent metabolic acidosis and hyperkalemia) due to non-responsive Hyperviscosity syndrome ultimately leads to the patient’s demise.
Discussion
Multiple myeloma as a separate entity was extensively documented for the first time in 1844, in a 39-year-old female named Sarah Newbury via autopsy. The disease was initially thought to have an inflammatory process where the bone substance was eliminated from the body via patients’ kidneys.3 This may explain the rise in cases of multiple myeloma in the western population because of the increasing age of the population. Fatigue and bony pain are often the commonest presenting symptoms in multiple myeloma, especially in patients with a high tumour burden. The hallmark lesions for multiple myeloma comprise lytic lesions seen on x-ray, present in up to 80% of cases. On x-rays, the frequent sites to be affected are the spine and ribs, with around 3% of patients also presenting with clinical features of spinal cord compression following compression fractures in vertebrae or due to soft tissue tumours in the spinal cord. Osteolytic lesions in multiple myeloma in contrast to neoplasms which show bony metastasis does not have new bone formation. These bone lesions are the consequence of an exaggerated osteoclastic process in active myeloma cases. Increased bone lysis may further lead to hypercalcemia which forms the other spectrum of clinical manifestations due to hypercalcemia in the form of constipation, abdominal pain, and confusion. Some red flag signs can contribute to early diagnosis such as chronic backache (forming 58% of complaints by patients), fatigue, weight loss along abnormal blood test results. Pleural effusion is a rare occurrence in multiple myeloma, forming < 6% of cases. However, the presence of pleural effusion indicates a poor prognosis with a median survival of fewer than 4 months. Another rare presentation can be Isolated cystic swelling.1 Evidence of end-organ damage in the form of renal impairment, bone marrow failure, bone damage, or hypercalcemia must induce the idea to start treatment immediately as these patients carry high-risk features. Initially, the tumour burden should be decreased to reduce the ongoing damage. The patients with multiple myeloma can be divided into 2 broad categories depending on if they are eligible for stem cell transplantation and the ones who cannot undergo intensive procedures.2
Plasma viscosity is primarily determined by the number of cells (cell volume), RBC’s mechanical properties, concentration, and nature of plasma proteins, etc. BHVS [blood Hyperviscosity syndrome] consists a characteristic of Waldenstrom’s triad which consists of visual disturbances (visual acuity decline, diplopia), mucosal bleeding (gum bleeding, epistaxis), and neurological manifestations (ataxia, motor deficit, headache, dizziness, tinnitus, chorea, altered consciousness, coma, and seizures). Some non-specific signs like signs of heart failure, dyspnoea, microcirculatory dysregulation (livedo reticularis, extremities necrosis), and pulmonary hypertension.5 Hyperviscosity syndrome presents itself in 3 distinct faces, generalized manifestations, vascular manifestations, and central nervous system manifestations. Patients with HVS may present with symptoms like loss of appetite, tiredness, and loss of weight. They may suffer from episodes of epistaxis that are recurrent in nature, menorrhagia, and bleeding per rectum and through gums. In the periphery, the patient may present with palmar erythema. Central nervous system manifestations may include dizziness, headaches, convulsions, nausea, and peripheral neuropathies. A shift of extra fluid into the vascular compartment due to increased serum proteins can precipitate congestive cardiac failure.6
A patient may suffer bleeding tendencies even with a normal platelet count due to increased blood viscosity. Patients who have chronic diseases may show a lower threshold for the development of HVS. Patients who have diabetes tend to develop visual symptoms earlier than non-diabetic patients, this may be because diabetic patients are already at risk for retinopathy. The rise in serum globulin concentration is not always in proportion to serum viscosity. Serum viscosity also varies as per immunoglobulin structure and their tendency to form aggregates. For example, IgM rapidly produces Hyperviscosity syndrome in lymphoid malignancy due to increased synthesis. HVS is seen in about 4% of multiple myeloma cases, maximum cases having IgG myeloma. This feature may be due to the tendency of IgG to form polymers at lower concentrations leading to an exaggerated rise in blood viscosity with only 3 times a rise in serum protein levels. In contrast, IgA myeloma rarely causes Hyperviscosity syndrome. Many immune complex diseases, some of which are having concomitant cryoglobulinemia develop Hyperviscosity. In patients with rheumatoid factor, they form intermediate complex” due to aggregation of proteins within the circulation. These complexes may come to be by various mechanisms. Their contents may vary as some have only IgG, some may have IgM, and some have ANA (anti-nuclear antibody). Some of these immunoglobulins deposit in glomeruli whereas others may lead to vasculitis.6
Hyperviscosity syndrome is a life-threatening emergency that may present with any of the following complications like ischemia leading to organ failure, myocardial infarction & thromboembolic events.7 The patient must also undergo laboratory investigations for complete blood count, coagulation studies, serum biochemistry, and urine analysis. Urine examination showing heavy proteinuria leading to a high albumin-protein gap may suggest gammopathy. Serum stasis can be indicated by rouleaux formation, serum stasis may further lead to improper lab equipment reading hindering the sample analysis. Immunoglobulins if measured quantitatively may help to determine long-term management.8 Hyperviscosity syndrome often presents as a medical emergency characterized by a wide spectrum of clinical manifestations due to raised plasma viscosity. The most common mode of presentation forms a triad of mucosal bleeding in the form of epistaxis or bleeding from the gums, neurological presentation in the form of altered consciousness, ataxia, chorea, etc. and visual symptoms in the form of diplopia or fall in acuity.5 Our patient came with chief complaints of epistaxis and headache. An extensive blood workup revealed that he has multiple myeloma and a peripheral smear showing rouleaux formation signifying the presence of HVS [Hyperviscosity syndrome].
The most common aetiology for HVS is Hypergammaglobulinemia, Waldenstrom macroglobulinemia to be specifically followed by multiple myeloma. 25% of these cases are due to elevated IgA immunoglobulins in plasma.8 Patients with multiple myeloma are prone to develop renal insufficiency in the presence of HVS that may go unrecognized for some time. Multiple myeloma patients having raised plasma viscosity show features of impaired blood flow through microvascular circulation, this may present as acute renal failure demanding an immediate response. Plasmapheresis is specifically required on an urgent basis either at the first clinical sign of HVS or even prophylactically in patients of multiple myeloma as soon as the patient's paraprotein level crosses the threshold.4 our patient too was planned for plasmapheresis but due to severe HVS the cannulation failed, and the patient succumbed the next day due to acute renal failure.
Classically, the syndrome is a result of increased amounts of immunoglobulin M (IgM) in Waldenstrom macroglobulinemia. Less commonly, symptomatic blood Hyperviscosity has been described in certain cases of MM, especially when abnormal polymers of IgA, IgG, or kappa light chains are produced. HVS is a consequence of stasis of blood that leads to circulatory failure ultimately resulting in organ dysfunction. The clinical spectrum is broad, including the following: Mucosal bleeding to life-threatening gastrointestinal haemorrhage. Cardio-respiratory symptoms. Vascular occlusion in the periphery may present as ulcers or gangrenes of the extremities and Raynaud’s phenomenon. 9,10,11
Conclusion: Hyperviscosity syndrome presents as a significant touchstone when dealing with patients with multiple myeloma and the complications following HVS can be often fatal while patients may present with varied clinical features each separate time. Timely interventions and standard treatment protocol even when followed to the letter may not be enough to save the patient in some cases. Careful clinical and laboratory correlation is a must to make a judgment for prompt management.
Acknowledgement: Nil
Conflict of interest: Nil
Source of funding: Nil
References:
1. Kumar S, Jain A, Waghmare S. Multiple cystic swelling: Initial presentation of multiple myeloma. Indian J Med Paediatr Oncol. 2010;31(1):28.
2. Gerecke C, Fuhrmann S, Strifler S, Schmidt-Hieber M, Einsele H, Knop S. The Diagnosis and Treatment of Multiple Myeloma. Dtsch Arztebl Int. 2016; 113(27-28):470-476.
3. Perez Rogers PA, Estes M. Hyperviscosity Syndrome. In: StatPearls. Treasure Island (FL). 2020.
4.Costa AF, Almeida F, Batista AF. Hyperviscosity syndrome - a case report. Int J Fam Commun Med. 2019;3(4):166-167.
5. El Kassim I, Touab R, Elkoundi A, Khayar Y. Blood Hyperviscosity Syndrome Revealing Multiple Myeloma in Emergency Department: Report of a New Case. 2018; 5:88–91.
6. Goldschmidt N, Zamir L, Poperno A, Kahan NR, Paltiel O. Presenting Signs of Multiple Myeloma and the Effect of Diagnostic Delay on the Prognosis. J Am Board Fam Med. 2016;29(6):702–9.
7. Yogesh Khithani, Sunil Kumar, Nitin Raisinghani, Sachin Agarwal, Ayush Somani.Multiple myeloma presenting as a pleural effusion in the elderly. Ann Geriatr Educ Med Sci. 2018 ;5(1):36–7.
8. Jewell S, Xiang Z, Kunthur A, Mehta P. Multiple Myeloma: Updates on Diagnosis and Management. Fed Pract Health Care Prof VA DoD PHS. 2015;32(Suppl 7):49S-56S.
9. Kaur G, Umar J, Thoguluva Chandrasekar V, Graziano S. Acute Respiratory Failure Secondary to Hyperviscosity Syndrome in a Rare Case of IgM Myeloma. Chest. 2016;150(4):410A.
10. Akhilesh Annadatha, Sourya Acharya, Samarth Shukla, Amol Bhawane, Anuj Varma, Amol Andale. Multiple Myeloma presenting as Hypercalcemic Crisis: A case report. Medical Science.2020;24(105):3148-3152.
11. Parveen, Sana, Jain S. Pathophysiologic Enigma of COVID-19 Pandemic with Clinical Correlates. Int J Cur Res Rev. 2020;12: 33-37
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





