IJCRR - 13(17), September, 2021
Pages: 10-15
Date of Publication: 12-Sep-2021
Print Article
Download XML Download PDF
Clinician's Choice of Health Related Quality of Life Index in Maxillectomy Patients with Obturator Prostheses: A Systematic Review
Author: Raut A, Hota S, Bhusan P, Mohanty A K, Padmanaban A
Category: Healthcare
Abstract:Introduction: Patients suffering from maxillary defects generally encounter difficulty in mastication, speech and postoperative depression. Such clinical cases can be rehabilitated with reconstructive surgery or obturator prostheses with or without implants to improve the quality of life(QOL). Study Selection: A systematic search of PubMed and web of science databases for articles published before 2020 December was performed by reviewers (reviewed). A manual search of articles published from January 2000 to December 2020 was also conducted. The present study identifies the most preferred QOL assessment index in patients with head and neck cancers who had undergone rehabilitation with obturator prostheses. Result: Most of the studies were cross-sectional and the most preferred HRQOL index used was OFS and UWQOL scale version 4. The result of the study also showed that meaningful quality of life can be achieved in patients who have undergone reconstruction with obturator prosthesis following maxillectomy. The study provides relevant information in selecting HRQOL measures as well as planning future studies and developing treatment protocols. Conclusion: The limited data indicate that fabrication of the obturator prostheses significantly contributes to improved psycho-logical well-being and the quality of life for maxillectomy patients. Well-designed clinical studies are necessary to draw definitive conclusions about how the fabrication of obturator prostheses affects the quality of life of maxillectomy patients.
Keywords: Health-related quality of life, Maxillectomy, Obturator functioning, Mastication, Swallowing, Cancer
Full Text:
INTRODUCTION
Maxillofacial Prosthetics is the art and science of anatomic, functional or cosmetic reconstruction using non-living substitutes of those regions in the maxilla, mandible, face and even other body parts that are missing or defective because of surgical intervention, trauma, pathology or developmental or congenital malformation.
The WHO defines the quality of life as the individual’s perception of their position in life in the context of the culture and value systems in which they live and concerning their goals, expectations, standards and concerns.2
Maxillary cancer represents a rare form of head and neck malignancy that can have a profound impact on the quality of life. The direct effect of cancer required therapeutic interventions and it can result in significant facial disfigurement as well as functional disability involving both swallowing and speech.4,16
Studies on the quality of life of patients with head and neck cancer have shown high levels of emotional anguish, physical constraints and disturbances in body image and damage in social relations.12 However, studies on changes perceived in quality of life after prosthetic rehabilitation are limited.
Traditionally, obturator prostheses have been used to occlude areas of the palate that have been resected. Reconstruction with obturator prostheses (with or without implants) diminishes difficulties associated with mastication and swallowing and has been shown to result in significant improvement in speech intelligibility and communication performance.16,17
Studies in the literature on quality of life in patients with maxillectomy and rehabilitation with obturators have shown that the correlation between obturator function and quality of life can be influenced by clinical factors, such as type of tumours and stage of disease, the extent of the ablative defect, postoperative radiation therapy, number and condition of remaining maxillary teeth and demographic and other social variables.1,14
Also, there are various types of scales/ indices available to assess the quality of life after prosthetic rehabilitation that increases randomness to draw a significant conclusion.
AIM
The study aims to identify
-
most frequently used index for assessment of the quality of life with obturator prosthesis in maxillectomy patients and
-
Factors/determinants that can influence overall QoL.
MATERIALS AND METHOD
A systematic literature review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The PRISMA Statement consists of a 27-item checklist and a four-phase flow diagram. The checklist includes items deemed essential for transparent reporting of a systematic review.11
Focused question patient intervention comparison and outcome (PICO format)
The review is focused on:” What is the efficacy of obturator prosthesis on quality of life of maxillectomy patients?”
Search strategy
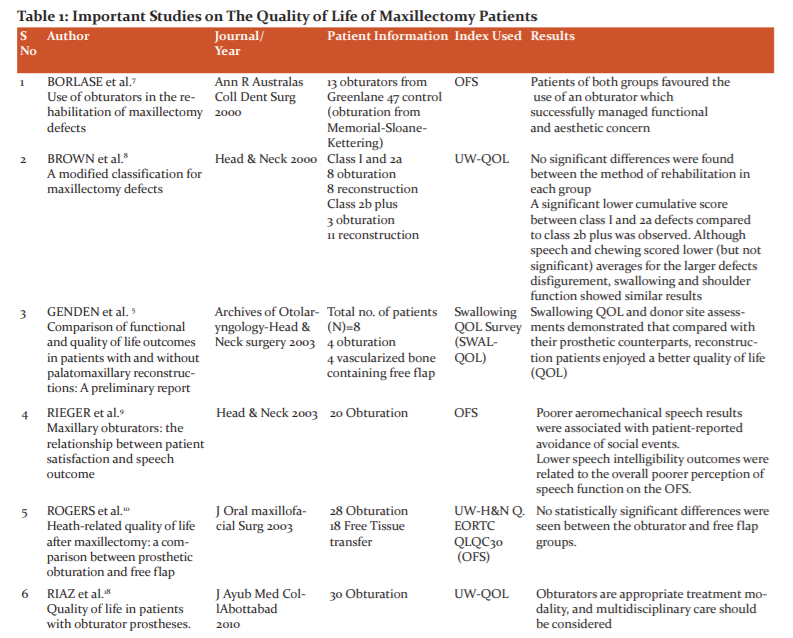
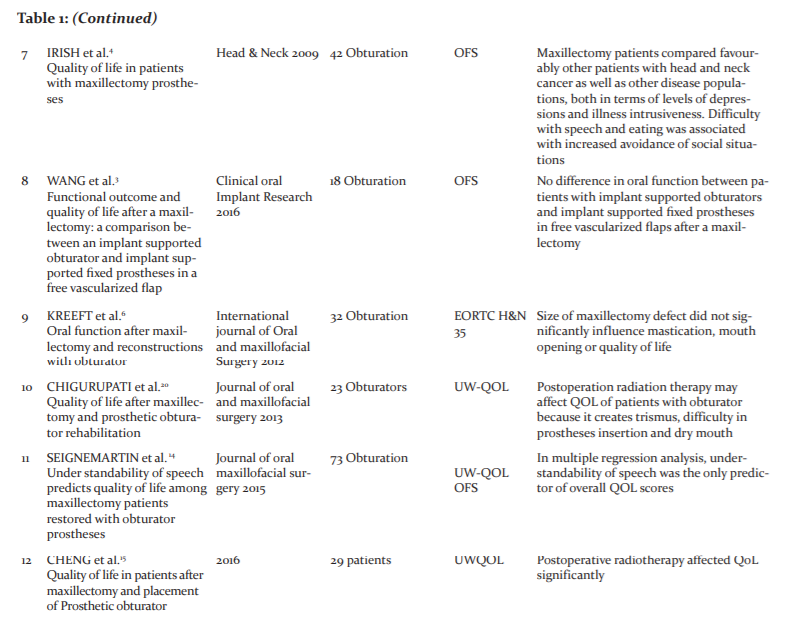
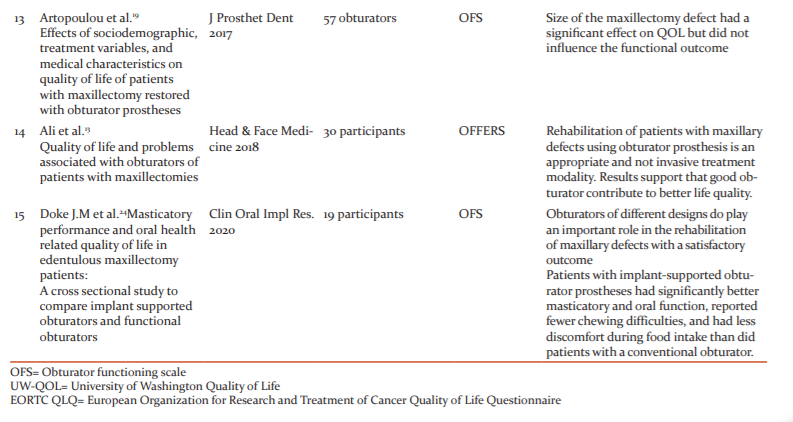
A MEDLINE electronic search on PubMed from January 2000 to December 2020 was conducted for articles published in the dental literature, and limited to human trials, using the search terms 'maxillofacial prosthesis', 'patient satisfaction, 'palatal obturators', 'positive life evaluation', 'head & neck cancer', 'health-related quality of life, 'maxillary obturator', 'facial prostheses'. (Table 1)
Moreover, a manual search of the following journals was also conducted: Journal of Prosthetic Dentistry, Journal of Oral Maxillofacial Surgery, and the International Journal of Oral and Maxillofacial Surgery, Journal of Plastic, Reconstructive & Aesthetic Surgery, Journal of Archives of Otolaryngology-Head and Neck Surgery, Journal of Head & Neck, Journal of Advanced prosthodontics.
Study exclusion criteria: Duplicate studies, in vitro and in vivo, obtained from the search results, case reports or case series, and studies based on interviews or commentaries were excluded to eliminate bias in the results. Studies of patients other than non-neoplastic origin were also excluded.
Two independent reviewers selected the studies for the systematic reviewing through each phasing of review screening, eligibility criteria and inclusion criteria. The Cohen kappa method was used to calculate inter-reviewer agreement. The selected studies were classified according to the Jadad scale. Studies classified as “low quality” had a score between 0 and 2, and those between 3and 5 were classified as “high quality.”
RESULTS
A total of 15 articles from the electronic and manual search of the PUBMED database were included in the study (Table 1). Out of 15 articles, twelve studies have used the OFS assessment index as it is the most common tool for such a study. The mean age was 55 years. Of the 15 articles, eleven were cross-sectional and four were longitudinal.
Results of the study can be summarized as
-
No significant correlation between the extent of the defect or maxillary defect classification and QOL or obturator functioning.
-
No significant correlation between various age groups and QOL.
-
Maxillectomy patients who receive additional radiation and chemotherapy rate score low on the QOL scale. Otherwise no significant difference between QOL of patients with prosthetic obturator prostheses or free flap reconstruction.
-
No complications related to obturator prostheses were reported.
-
The use of dental implants in combination with CAD/CAM results in the best functional outcome and least morbidity.
-
Further research such as the application of stem cells may help to overcome associated problems of obturator prostheses or free flap reconstruction and improve overall QOL.
DISCUSSION
The systematic review shortlisted a limited number of studies that evaluated the QOL of patients with maxillary defects who underwent prosthetic rehabilitation with obturator prostheses. A direct comparison of the QOL scores was a challenge as most of the studies included were not randomized or double-blind studies. Most of the articles are based on cross-sectional study design tending to adapt to most treatments over time and thus differences among groups may be identified only in a longitudinal study.
UWQOL score
The questionnaire consists of 15 questions. The first 12 domains concern areas of daily living that are often affected by treatment of head and neck cancer, such as pain, disfigurement, activity, recreation and entertainment, chewing, swallowing, speech, shoulder disability, taste, saliva, and 2 new emotional domains of mood and anxiety. To describe current functional status, each domain has a maximum score of 100 points, indicating the highest level of function, and a minimum score of 0, indicating the poorest level of function.
OFS score
The OFS was developed at Memorial Sloan-Kettering Cancer Center as a means of assessing the self-reported functioning of an obturator. TheOFS score gives information about the degree of patient satisfaction and qualitative assessment of obturator prosthesis. The questionnaire is very intelligently framed to give relevant information regarding eating and speech. Dryness of mouth, an effect of radiotherapy on major and possibly minor salivary glands, was included as an item in the scale because poor lubrication of the mouth is a possible contributor to poorer fit or functioning of the prosthesis. Another item, “difficulty talking on the phone,” was added to the scale to assess communication difficulties in the absence of visual cues. The answer to each question is rated in a numerical value from 0 to 100.
Most of the studies used more than one index to measure HRQOL. The most frequently used scale is OFS, however, more studies are needed for establishing the clinical utility of OFS as a screening measure. Different retention mechanisms like the addition of attachments, zygomatic implants and rapid prototyping or CAD/CAM techniques score high on the scale.
Other Variables
Brown et al. attempted a practical classification of maxillectomy defects that describes the defect and indicates the likely functional and aesthetic outcome.8In this study most commonly reported defects were 2A or 2B. Leakage when swallowing food was the most commonly reported problem however adaptation develops to maintain QOL.
Age was considered an influential factor to decide the type of reconstruction by the patient. One study based on the rehabilitation of hemipalato maxillectomy defects using a prosthetic obturator or a vascularized bone containing free flap highlighted the advantage of a permanent tissue closure of the palatal defect to reduce morbidity.5The study revealed young patients prefer surgical closure despite the additional cost and procedure involved. Prosthetic rehabilitation is better when it follows reconstruction. However, no statistically significant differences were seen between obturators and free flap groups. Reconstruction complications are more evident in patients with malignant tumours resulting in relapse, dehiscence of the grafted tissue, fistula development and necrosis.
The quality and quantity of supporting tissue and remaining natural teeth influence the relationship and position of the prosthesis to the implant. A retained implant obturator prosthesis is indicated as long as the supporting bone is adequate for the fixation of implants.
Postoperative radiotherapy negatively influences mean maximal mouth opening. The limited mouth opening profoundly diminishes the quality of life due to the inability of speech, mastication and deglutition. Post radiation trismus compromises the prognosis. Open defects were more compromised because of both radiotherapy and chemotherapy leading to elevated response on the total OFS score which would suggest overall dissatisfaction with the obturator scale.6,10,20,23
Reduced salivation and susceptibility to frequent soft tissue injury and frail nature of oral mucosa following radiation therapy is a significant limiting aspect. The absence of clinically significant xerostomia does not preclude the possibility of dry mouth. Silicone-lined obturators were well anchored and comfortable exhibiting greater efficiency towards QoL. Dryness of mouth is also associated with lower speech intelligibility scores. Another study revealed participants found moist and softer foodstuff easier to masticate; hard and dry foods presented the greatest difficulty. This was attributed to the greater likelihood of reduced salivation post maxillectomies.22
One of the studies added a question specifically related to difficulty talking on the phone in the OFS scale as an adaptation measure.4Poor aeromechanical speech results were associated with patient-reported avoidance of social events, whereas lower speech intelligibility outcomes were related to the overall poorer perception of speech function on the OFS.9
Two studies emphasized specialists emphasizing regular care and follow up visits for obturators as an appropriate treatment option to identify tumour recurrence, discomfort and adaptation failure before treatment failure.12,21
One study claimed that patients who underwent a facial approach reported on lower quality of life than those who underwent a transoral approach. Female patients showed a higher level of depression than male patients, although this did not reach significance.4Also better ratings were found for patients who received a higher level of education.
Implants offer more promising and predictable treatment options by supporting an obturator prosthesis in place and improving mastication and tissue adaptation.24However, limited residual bone after a maxillectomy is a large problem for the implant approach. The use of zygomatic implants with magnets and bar attachments has changed the treatment modality and offered retention force to enhance support and improve the stability of the obturator prosthesis. A treatment approach consisting of multiple zygomatic implants was considered to create a source of vertical resistance and retention. The advent of zygomatic implants has drastically enhanced treatment and potentially revolutionized maxillary reconstruction following extensive ablative tumour resection.3
As the selected articles are suggestive of low quality on the Jadad scale no robust inference can be drawn. The free tissue transfer reconstruction eliminates physiologic distress to the patients and provide excellent management of maxillectomy defects but on the contrary obturator prostheses provide immediate reestablishment of facial morphology and oral functioning. There is a significant improvement in speech, swallowing and overall quality of life with operators under regular follow up period.
Health-related quality of life (HRQOL) is an important outcome parameter following treatment of head and neck cancer. Two national bodies, the British Association of Head and Neck Oncologists and the British Association of Otorhinolaryngologists Head and Neck Surgeons http:/www.bahno.org.uk/bulletin.htm#quality, both recommend that HRQOL should be longitudinally recorded. Questionnaires give a structured insight into the patients’ opinions. They facilitate multidisciplinary teams working with the recognition of poor outcome groups and the opportunity to identify problem areas and target support/intervention.
Limitations of the study:
-
The most important limitation in the included studies was that there was significant clinical heterogeneity between the studies which makes it difficult to conclude. Statistically, significant improvement cannot be calculated due to the inability to perform the meta-analysis. Prospective, blinded, randomized, multicenter studies with standardized methodology need to be performed. According to the Jadad scale, all selected studies showed low quality. Direct comparison of the results are not possible as in different studies, different tests and scales were used to evaluate the QoL.
-
Small sample size: As maxillary cancer is a rare tumour with increased mortality small sample sizes are typically found in studies of maxillectomy patients.
-
Despite intensive research related to the quality of life post-cancer therapy, only a few studies evaluate the quality of life of maxillectomy patients rehabilitated with an obturator.
-
Because of the low incidence of maxillofacial tumors, it is not possible to organize prospective studies.
CONCLUSION
This systematic review reveals good obturator function is strongly correlated with the improved quality of life. Patients who undergo maxillectomy often enquire about the quality of life post-surgery. The present study data can be used to reassure patients following maxillectomy and prosthetic reconstruction to have an acceptable quality of life. However, the presence of family members, socioeconomic status and valued activities and interests all help people with cancer to overcome functional disability. Stem cell regeneration and advanced future research can modify the approach to obturator prosthesis or free flap reconstruction and will help to improve patients' QoL after maxillectomy in the future. Future research objective also includes the need for meta-analysis.
Acknowledgment: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding: self
Conflict of Interest: Nil
References:
1. Kumar P, Alvi HA, Rao J, Singh BP, Jurel SK, Kumar L, et al. Assessment of the quality of life in maxillectomy patients: A longitudinal study. J Adv Prosthodont. 2013;5:29-35.
2. What quality of life? The WHOQOL Group. World Health Organization Quality of Life Assessment. World Health Forum. 1996;17:354-6.
3. Wang F, Huang W, Zhang C, Sun J, Qu X, Wu Y.Functional outcome and quality of life after a maxillectomy: a comparison between an implant-supported obturator and implant-supported ?xed prostheses in a free vascularized flap.Clin. Oral Impl. Res. 2017 Feb;28(2):137-143.
4. Irish J, Sandhu N, Simpson C, Wood R, Gilbert R, Gullane P, et al. Quality of life in patients with maxillectomy prostheses. Head Neck. 2009;31:813-21.
5. Genden EM, Okay D, Stepp MT, Rezaee RP, Mojica JS, Buchbinder D, et al. Comparison of functional and quality-of-life outcomes in patients with and without palatomaxillary reconstruction: a preliminary report. Arch OtolaryngolHead Neck Surg 2003;129:775-80.
6..Kreeft AM, Krap M, Wismeijer D, Speksnijder CM, Smeele LE, Bosch SD, et al. Oral function after maxillectomy and reconstruction with an obturator. Int J Oral Maxillofac Surg 2012;41:1387-92.
7..Borlase G. Use of obturators in rehabilitation of maxillectomy defects. Ann R AustralasColl Dent Surg. 2000 Oct;15:75-9.
8. Brown JS, Rogers SN, McNally DN, Boyle M. A modified classification for the maxillectomy defect. Head Neck. 2000;22:17-26.
9. Rieger JM, Wolfaardt JF, Jha N, Seikaly H. Maxillary obturators: the relationship between patient satisfaction and speech outcome. Head Neck. 2003;25:895-903.
10. Rogers SN, Lowe D, McNally D, Brown JS, Vaughan ED. Health-related quality of life after maxillectomy: a comparison between prosthetic obturation and free flap. J Oral Maxillofac Surg. 2003;61:174-81.
11 Brandao TB, Filho A, Batista V, Oliveira M, Silva A. Obturator prostheses versus free tissue transfers: A systematic review of the optimal approach to improving the quality of life for patients with maxillary defects. J Prosthet Dent. 2016;115:247-253
12. Goiato MC, Pesqueira AA, Silva CR, Filho HG, Santos DMD. Patient satisfaction with maxillofacial prosthesis. Literature review. JPlas Recons Aes Surg. 2009;62:175-180.
13. Ali MM, Khalifa N, Alhajj MN. Quality of life and problems associated with obturators of patients with maxillectomies. Head Med. 2018 14:2:1-9
14. Seignemartin CP, Miranda ME,Luz JGC,Teixeira RG. Understandability of speech predicts quality of life among maxillectomy patients restored with obturator prosthesis. J Oral Maxillofac Surg 2015;73:2040-2048.
15. Chen C, Ren WH, Huang RZ, Gao L, Hu ZP, Zhang LM, et al.Quality of Life in Patients After Maxillectomy and Placement of Prosthetic Obturator.Int J Prosthodont. Jul-Aug 2016;29(4):363-8.
16. Arigbede AO, Dosumu OO, Shaba OP, Esan TA. Evaluation of speech in patients with partial surgically acquired defects: pre and post prosthetic obturation. J Contemp Dent Pract. 2006;7:89–96.
17. Sullivan M, Gaebler C, Beukelman D, Mahanna G, Marshall J, Lydiatt D et al. Impact of palatal prosthodontic intervention on communication performance of patient’s maxillectomy defects: a multilevel outcome study. Head Neck. 2002;24:530–538.
18. Riaz N, Warriach RA.Quality of life in patients with obturator prostheses. J Ayub Med Coll Abbottabad. Apr-Jun 2010;22(2):121-5.
19. Artopoulo LL, Karademas EC, Papadogeorgakis N, PapathanasiouI, Plyzois G. Effects of sociodemographic, treatment variables and medical characteristics on quality of life of patients with maxillectomy restored with obturator prostheses. J Prosthet Dent. 2017
20. Chigurupati R, Aloor N, Salas R, Schmidt BL. Quality of life after maxillectomy and prosthetic obturator rehabilitation. J Oral Maxillofac Surg. 2013;71:1471-8.
21. Santos DMD, Caxias FP, Bitencourt SB, Turcio KH, Pesqueira AA, Goiato MC. Oral rehabilitation of patients after maxillectomy. A systematic review.Br J Oral Maxillofac Surg. 2017.
22. Ikusika OF, Dosumu OO, Ajayi DM, Ogurinde TJ. Effect of the resilient lining of obturator bulbs on patients with maxillectomies. J Prosthet Dent. 2016 Dec;116(6):932-936.
23. Said M, Otomaru T, Yeerken Y, Taniguchi H. Masticatory function and oral health-related quality of life in patients after partial maxillectomies with closed or open defects. J Prosthet Dent. 2017 Jul;118(1):108-112
24. Buurman DJM, Speksnijder CM, Engelen BHBT, Kessler P Peter Kessler, Masticatory performance and oral health-related quality of life in edentulous maxillectomy patients: A cross-sectional study to compare implant-supported obturators and conventional obturators. Clin Oral Impl Res. 2020;31:405–416.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





