IJCRR - 2nd Wave of COVID-19: Role of Social Awareness, Health and Technology Sector, June, 2021
Pages: 220-226
Date of Publication: 11-Jun-2021
Print Article
Download XML Download PDF
Clinical Presentation and Outcomes of COVID-19 in Pediatric Age Group: An Observational Study of 93 Children from North India
Author: Motiani P, Shukla U, Madan J, Bhakri B K, Singh D K, Jain D
Category: Healthcare
Abstract:Introduction: Worldwide the data regarding the epidemiological features and transmission patterns of COVID-19 infection among children is evolving. We present our observations on the presentation and clinical course of COVID-19 infection among children. Methods: Retrospective analysis of records of children admitted with COVID infection in a tertiary care COVID facility in north India. Results: Records from 93 case files were analysed. Most of the children were infected after close contact with an infected family member. The majority of them were males and asymptomatic. Younger anaemic children were more likely to be symptomatic. Only a small proportion (< 4 %) required intensive care and one infant with severe malnutrition expired. Conclusion: Children are primarily getting COVID infection from household contacts and have a relatively better prognosis. The clinical outcomes observed in India are comparable to those reported from other regions of the world.
Keywords: COVID-19, Pediatric, North India
Full Text:
INTRODUCTION
The epidemiological information for COVID-19 is still evolving. While a growing number of studies from across the globe have widely discussed the presentation of COVID-19 since its outbreak, very limited data is available on epidemiological features and transmission patterns among children.1-3 Worldwide, children of all ages and with a wide range of demographic and socioeconomic characteristics and ethnicity appear susceptible.4,5,6 Majority of available literature suggest relatively better disease outcomes among children, with more than 90% of them being either asymptomatic or presenting with mild or moderate disease.7,8 However, despite being assured, the available quantum of literature on pediatric COVID-19 infection is not yet enough to be considered conclusive. There is a need of generating further data with particular emphasis on the populous tropical Indian subcontinent region.
We present our observations on the presentation and clinical course of COVID-19 infection among children (birth to 18 years of age) from a tertiary care teaching hospital in India.
METHOD
This was an observational study involving the analysis of records of children (up to 18 years of age) admitted at our hospital between 1st April 2020 and 31st July 2020. Data were collected retrospectively for patients admitted till 23rd June 2020 and prospectively for children admitted subsequently. The study was approved by the Ethics committee of the institute. Ours is an exclusive paediatric super-speciality teaching hospital located in north India which was designated as an exclusive COVID care facility in early April 2020. The hospital offered comprehensive care for children including a critical care facility. Children were either diagnosed by contact tracing following the detection of COVID-19 infection among any of their close contacts or by the screening of the children visiting our facility with signs and symptoms conducive to the possibility of COVID-19 infection. Records from children diagnosed with COVID-19 infection either with:
-
Rapid Antigen Test-A rapid, qualitative, chromatographic immunoassay was done using a card-based sensor of the make SD Biosensor, with a turnaround time of 30 mins.
-
TruNAT test – Done in a 2 step process using TruelabR AUTO V2 Universal Cartridge based Sample Prep Device and TruelabTM Quattro Real-time Quantitative micro PCR analyzer, with appropriate Kits, from M/s Molbio Diagnostics Private Limited or
-
Reverse transcriptase-polymerase chain reaction test (RT-PCR) involving Extraction using ZYBIO Nucleic Acid Purification system; and Amplification using The AriaMx Real-Time PCR system from M/s Agilent Technologies or CFX96 from M/s Biorad with various ICMR Approved kits.
As per the guideline released by the Ministry of Health & Family Welfare, the presentation of illness among children was defined either asymptomatic or with mild, moderate or severe symptoms.9 Children were managed as per the standard guidelines as adopted by the administration of the state from time to time.10
The recorded parameters included demographic (age, gender, residential location, history of travel during last 2 weeks, either international or to any area designated as disease hotspot, close contact with a person tested positive for COVID-19), clinical details (parameters at the time of admission, evidence of past BCG immunization, presence of comorbidities, duration of hospital stay and outcome) and laboratory parameters (haematological, liver and renal functions and chest radiograms) which were performed as and when indicated as per standard practice.
The data were recorded in Microsoft Excel sheets and analyzed using SPSS software. Continuous measures were depicted as mean (SD) or median (IQR) as applicable and analyzed using the test. Categorical measures were depicted as proportions and analyzed using either the ‘Chi square’ or ‘Fisher exact’ test. Correlation among the parameters was studied using Pearson’s correlation coefficient. The ‘p’ value of <0.05 was considered significant.
RESULT
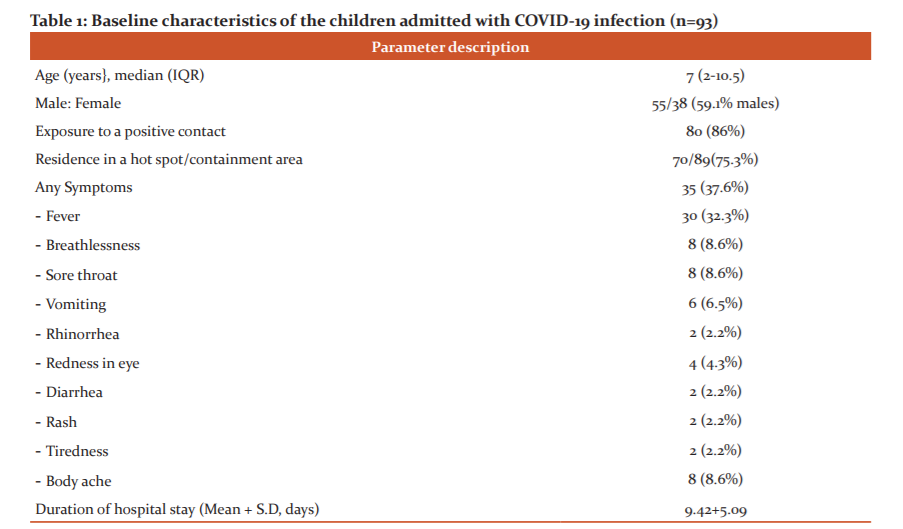
During the study period, 93 children with COVID-19 were admitted. The baseline characteristics of the cases are depicted in Table 1. There was insignificant male preponderance and 15 children were aged less than 1 year (3 newborns). The majority of patients, of varying age groups and either gender, had been exposed to a COVID-19 positive contact or resided in the locality designated hot spot containment zone by the government. The information about receiving BCG vaccination during early infancy was recorded in the case records of 36 children, all of which received it. The presentation of the disease, as well as the duration of hospital stay among these patients, was similar to the rest in the study.
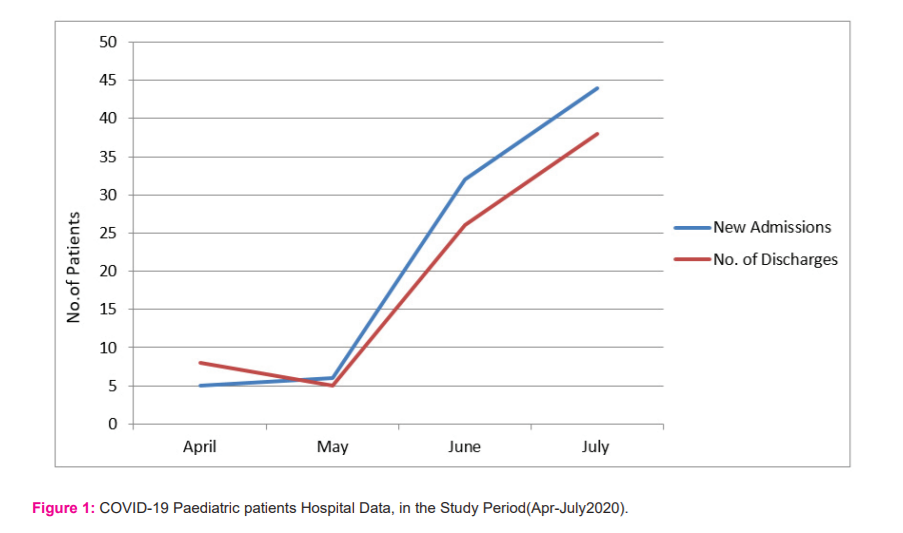
Thirty-five (37.6%) patients were symptomatic at admission with fever being present in the majority. Among them, a majority presented with mild disease (n=31; 33.3 %), a few with moderate (n=3, 3.22%) and only one (1.07%) with severe disease. There were a relatively higher proportion of infants among symptomatic (7 of 35) than asymptomatic children (8 of 58) but the result was not statistically significant (p=0.21). The number of hospital admissions showed an increasing pattern from April to July 2020. Discharges showed an initial decrease followed by an increase (Figure1). Till the end of data collection, 14 of the enrolled patients were still admitted, 78 (83.8%) children were discharged while one expired.
Associated comorbidity was observed among 5 (5.37%) patients. These included coeliac disease, congenital muscular dystrophy, acute myeloid leukaemia, pulmonary tuberculosis and traumatic hydropneumothorax in one child each (Figure1 and Table 1).
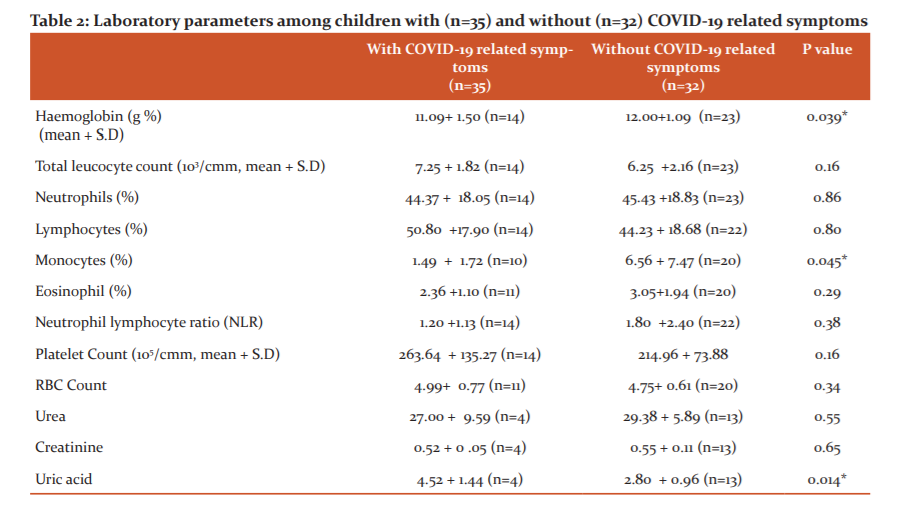
Haematological and renal function parameters along with chest radiogram were assessed in the children who had symptoms related to COVID-19 infection, any comorbidity or other clinical signs (anaemia, poor weight gain etc) warranting investigation. Among the 67 patients for which these investigations were performed, 35 were admitted with symptoms suggestive of COVID-19 infection. The comparison of lab parameters among those with and without COVID-19 related symptoms is presented in Table 2. Among all the children investigated, the mean +S.D haemoglobin, total leucocyte count and platelet count were 11.85 + 1.12 g%, 6.68 + 2.09 X 103/cmm and 2.32 + 1.29 X 105/cmm respectively. Compared to others, children with COVID-19 symptoms had significantly lower haemoglobin levels, monocyte count and uric acid levels (p=0.039, 0.045 & 0.014 respectively). Among 37 chest radiograms performed over patients, abnormalities were only noticed in 2 (one each with hydropneumothorax and bilateral pulmonary infiltrates secondary to tuberculosis).
Oxygen supplementation was needed in 4 children who also received Azithromycin and Dexamethasone. The only child who succumbed to the infection was 10 months old severely malnourished boy. He presented with encephalopathy and hemodynamic instability which progressed during the hospital stay of 60 hours. The mean duration of hospital stay was 9.42+5.09 days without any significant difference among symptomatic or asymptomatic patients (p=0.23). The hospital stay was neither significantly correlated with the age or gender of the patients (Table 2).
DISCUSSION
In our study, the majority of children were infected after close contact with infected family members. While most of the children were asymptomatic, younger anaemic children were more likely to be symptomatic. Only a small proportion (<4 %) required intensive care and one infant with severe malnutrition expired among 93 children.
Our observations represent the spectrum of presentation and outcomes of paediatric COVID-19 infection prevalent in the Indian subcontinent region. Though there is a reasonable amount of information available for adult COVID-19 patients, our observations should meaningfully add to the limited worldwide literature on paediatric COVID-19 infection. The set of patients from our institute, which caters to children with a wide range of socio-demographic characteristics, fairly represents the general population in the region.
Our study indicates an initially slow but later moderate rise in the number of patients admitted at the institute. This is following the trend of progression of the disease in the region possibly due to early implementation of effective infection control measures.11 The initial blunting of pandemic progression appears to have provided a reasonable time frame for strengthening clinical care and diagnostic facility infrastructure to manage the later rise in the infection rate.
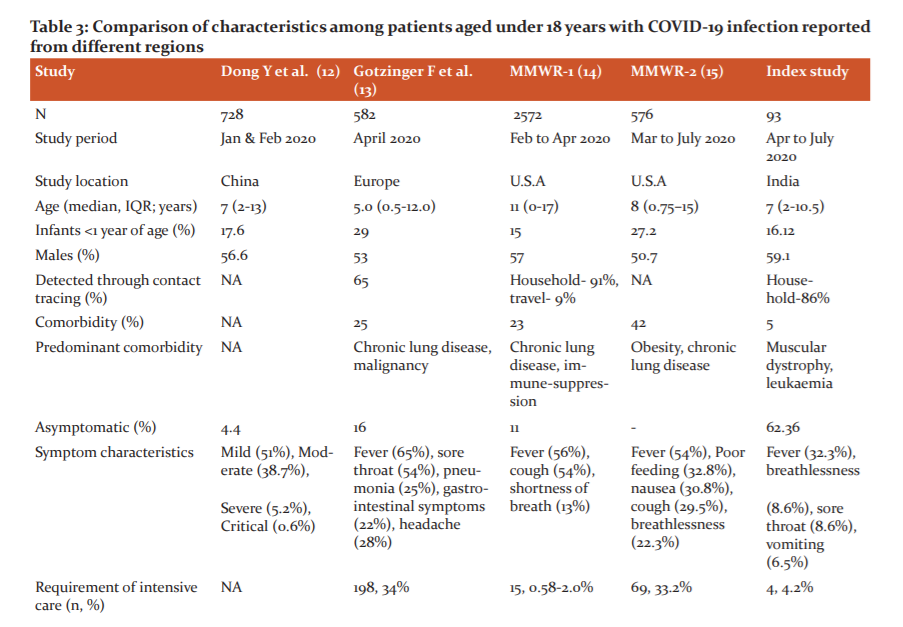
Our key observations are presented in comparison with those from few major studies from China, Europe and North America in Table 3.12-15 The age distribution of our study group (median, IQR: 7.0 (2-10.5 years) is comparable to the published data from these regions. In our study, males constituted 59.1% of the patients. This male predominance was maintained across all age subgroups and is similar to the observations made in these studies. Though not statistically significant it could be an important potential indicator towards the possibility of biological factors playing a role in COVID-19 susceptibility by gender. Exposure to close contact in the family (n=80/93; 86%) and residence in a hot spot containment zone (n=70/89; 75.3%) constituted the most important exposure characteristic of these patients in our study. This is in concurrence with reports on paediatric COVID -19 cases from the USA which identifies travel and exposure to a COVID-19 patient in the household or community, as the main factors responsible for transmission.14 Similar observations were reported from China as well as from 82 institutes in 25 European countries.12,13
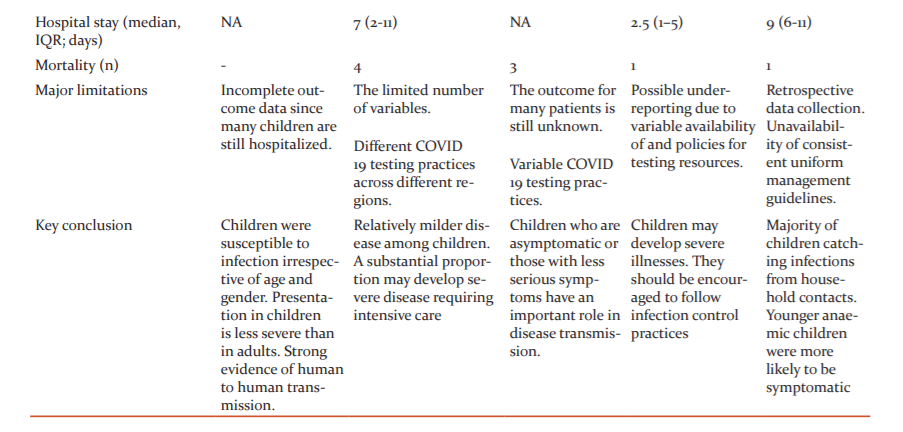
The trends in the number of hospital admissions and discharges observed by us appear to reflect the changing epidemiology of the infection in the region as well as the variations in admission and discharge policies released by regional administration from time to time. The mean+S.D duration of hospital stay was 9.42+5.09 days. There was no difference in the duration of hospital stay in symptomatic patients or symptomatic ones. The duration of hospital stay was, however, longer in the early months. This could be partly because earlier all patients were discharged from the hospital only after repeat microbiological testing at the end of a certain period of hospital stay. This was modified in the subsequent recommendations. In our study, 58 of 93 (62.36%) patients were asymptomatic at admission. Among those who were symptomatic, 31 (33.3%) had a mild, 3 (3.2%) had moderate and 1 patient was admitted with severe symptoms of COVID-19. This is similar to that reported in studies from China, Europe and the USA where a large majority of children have either been asymptomatic or have had mild disease.12-15 Somebody of evidence also identifies the asymptomatic patients as the cause of concern as they are potential carriers or transmitters of infection in society.16
The presentation of COVID-19 has been less severe in children as compared to adults and the reasons for this may be related to both exposure and host factors. Children have been usually well cared for at home and have had fewer opportunities to expose themselves to pathogens and /or sick patients. It has been further speculated that children are possibly less sensitive to nCOV 2019 because the binding ability of ACE-2, a likely cell receptor of nCOV 2019, in children may be lower than that of adults17. In contrast, a European study has concluded that a substantial proportion (8%) of COVID-19 affected children develop severe disease requiring intensive care and prolonged mechanical ventilator support.13 They identified the risk factors for ICU admission to be age ≤ 1 month, male gender, presence of lower respiratory tract infection and presence of a pre-existing medical condition and viral coinfection. An American study similarly concluded that though children can also develop a severe COVID 19 illness requiring intensive care (33.2% children) similar to adults (32.0%), invasive mechanical ventilation was less frequently required in children (5.8%) than in adults (18.6%).15 Similar to our study (32.3%), fever was documented as the commonest symptom in most of the studies (56-65%).12-15 In our patients, sore throat and breathlessness (in 8.6% each) were other common symptoms. There were 5(5.3%) patients with comorbidities in our study. This was lower than that reported in other studies where chronic lung disease, immunosuppression and obesity have been identified as major comorbidities.13,14,15 The mortality rate in our study was lower than that reported by other authors.12-15 This difference may be partially explained by variation in the hospital admission criteria being followed in different regions.
The data regarding laboratory parameters was available in 67 of our patients. At admission, the baseline haemoglobin and monocyte count were significantly lower in symptomatic as compared to asymptomatic patients (p=0.039; p=0.045 respectively). A lower haemoglobin count in symptomatic children has also been reported in a study from Wuhan’s Children Hospital, China.18 They however reported a higher monocyte count in these children, in contrast to our findings. We also observed a higher white blood cells count and lymphocyte count among symptomatic children. However, the difference was not statistically significant. We also observed significantly elevated serum uric acid levels among symptomatic as compared to asymptomatic children (p=0.014). A similar observation was reported in a study from China and maybe a potential indicator of renal involvement during the illness.19
Being a preliminary descriptive set of observations, the results from our study have few limitations. The retrospective nature of data collection and unavailability of consistently available uniform guidelines for diagnosis, admission and management across the course of study are likely to weaken the strength of the information. However, the novel COVID 19 global pandemic posed similar challenges for health care facilities all around the world. Despite these limitations, our observations are likely to have important implications for planning further health care services and allocation of resources during the ongoing pandemic situation (Table 3).
CONCLUSION
Children are primarily getting COVID infection from household contacts and have a relatively better prognosis. The clinical outcomes observed in India are comparable to those reported from other regions of the world.
DECLARATIONS:
Ethical Approval was taken from the institutional ethical committee. IEC Letter no 2020/17/IM/02
Funding support of any form/source – Nil
Conflict of interest – Nil
Author Contribution:
All authors contributed equally. The manuscript has been read and approved by all the authors and each author believes that the manuscript represents honest work. Requirements for authorship meet the stated criteria.
References:
1: Hoang A, Chorath K, Moreira A, Evans M, Burmeister-Morton F, Burmeister F, Naqvi R, Petershack M, Moreira A. COVID-19 in 7780 pediatric patients: A systematic review. E Clin Med. 2020 Jun 26;24:100433.
2. Zhang L, Peres TG, Silva MVF, Camargos P. What we know so far about Coronavirus Disease 2019 in children: A meta-analysis of 551 laboratory-confirmed cases. Pediatr Pulmonol. 2020 Aug; 55(8):2115-2127.
3: Kuttiatt VS, Abraham PR, Menon RP, Vaidya PC, Rahi M. Coronavirus disease 2019 in children: Clinical & epidemiological implications. Indian J Med Res. 2020 Jul & Aug;152(1&2):21-40.
4. Liguoro I, Pilotto C, Bonanni M, Ferrari ME, Pusiol A, Nocerino A, Vidal E, Cogo P. SARS-COV-2 infection in children and newborns: a systematic review. Eur J Pediatr. 2020 Jul; 179(7):1029-1046.
5: Mustafa NM, A Selim L. Characterisation of COVID-19 Pandemic in Paediatric Age Group: A Systematic Review and Meta-Analysis. J Clin Virol. 2020 Jul;128:104395.
6: Patel NA. Pediatric COVID-19: Systematic review of the literature. Am J Otolaryngol. 2020 Sep-Oct;41(5):102573
7. Saleem H, Rahman J, Aslam N, Murtazaliev S, Khan S. Coronavirus Disease 2019 (COVID-19) in Children: Vulnerable or Spared? A Systematic Review. Cureus. 2020 May 20; 12(5):e8207.
8. Ludvigsson JF. A systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 2020 Jun; 109(6):1088-1095.
9. Revised guidelines for Home Isolation of very mild/pre-symptomatic COVID-19 cases. https://www.mohfw.gov.in/pdf/Revised guidelines for Home Isolation of very mild presymptomatic COVID 19 cases 10May2020.pdf
10. Sankar J, Dhochak N, Kabra SK, Lodha R. COVID-19 in Children: Clinical Approach and Management. Indian J Pediatr. 2020 Jun;87(6):433-442.
11. Mahajan P, Kaushal J. Epidemic Trend of COVID-19 Transmission in India during Lockdown-1 Phase. J Community Health. 2020 Jun 23:1-10.
12. Dong Y, Mo X, Hu Y, Qi X, Jiang F, Jiang Z, Tong S. Epidemiology of COVID-19 Among Children in China. Paediatrics. 2020 Jun;145(6):e20200702
13. Götzinger F, Santiago-García B, Noguera-Julián A, Lanaspa M, Lancella L, Calò Carducci FI, et al. COVID-19 in children and adolescents in Europe: a multinational, multicentre cohort study. Lancet Child Adolesc Health. 2020 Sep; 4(9):653-661.
14. CDC COVID-19 Response Team. Coronavirus Disease 2019 in Children - United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep. 2020 Apr 10;69(14):422-426.
15. Kim L, Whitaker M, O'Halloran A, Kambhampati A, Chai SJ, Reingold A, et al, COVID-NET Surveillance Team. Hospitalization Rates and Characteristics of Children Aged <18 Years Hospitalized with laboratory-confirmed COVID-19 - COVID-NET, 14 States, March 1-July 25, 2020. MMWR Morb Mortal Wkly Rep. 2020 Aug 14;69(32):1081-1088.
16. Liu C, He Y, Liu L, Li F, Shi Y. Children with COVID-19 behaving milder may challenge the public policies: a systematic review and meta-analysis. BMC Pediatr. 2020 Sep 1;20(1):410.
17. Fang F, Lu X. Facing the pandemic of 2019 novel coronavirus infections: the pediatric perspectives [published online ahead of print February 2, 2020]. Chinese J Ped.2020 Feb;58(2):81-85.
18. Xiong X, Chua GT, Chi S, Kwan MYW, Wong WHS, et al. Haematological and immunological data of Chinese children infected with coronavirus disease 2019. Data Brief. 2020 Jun 30;31:105953
19. Wang Y, Zhu F, Wang C, Wu J, Liu J, Chen X, Xiao H, Liu Z, Wu Z, Lu X, Ma J, Zeng Y, Peng H, Sun D. Children Hospitalized With Severe COVID-19 in Wuhan. Pediatr Infect Dis J. 2020 Jul;39(7):e91-e94.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





