IJCRR - 13(16), August, 2021
Pages: 190-197
Date of Publication: 30-Aug-2021
Print Article
Download XML Download PDF
Effectiveness of Child-Centred Distraction in the Management of a Child's Dental Anxiety During Invasive Dental Procedures
Author: Sahithi V, Elicherla SR, Saikiran KV, Challa RR, Nuvvula S
Category: Healthcare
Abstract:Background and Aim: Distraction is the technique of diverting the patient's attention from an unpleasant procedure. It is of two type's active and passive distraction. The present study was performed to evaluate the efficacy of child-centred distraction (CCD) in alleviating dental anxiety of children using three techniques during invasive dental procedures. Materials and Methods: Sixty children (40 boys and 20 girls), aged 7 to 11 years, were randomly allocated into three groups: Group1- Mobile video games (VG), Group 2- Virtual reality (VR), and Group 3- Mobile cartoons (MC) respectively, during the treatment sessions. The anxiety of the children was assessed using physiologic measures (heart rate) at three different time points, i.e., before, during, and after the procedure, whereas RMS pictorial scale was employed as a subjective measure before and after the procedure. Kruskal Wallis- ANOVA and Wilcoxon Sign Rank Test was used to analyze the RMS Scores, and repeated measures of ANOVA was used to test the mean difference of pulse rates. Results: On intergroup comparison, there was no statistical difference among the three groups before commencing the treatment (P-value > 0.001). But, a statistical difference in all the groups (P-value ≤ 0.001) was evident after instituting the distraction techniques. Amongst all the three groups, a significant reduction in anxiety scores was elicited by the children in group 1. Conclusion: This study has attempted to enhance the salience of distraction techniques in tumbling a child's dental anxiety. Involving the child in decision making while using distraction techniques has a foremost impetus in most children, instilling a new positive attitude towards the dental procedures.
Keywords: Behaviour guidance, Dental anxiety, Distraction
Full Text:
Dental anxiety is a widespread emotional phenomenon anteceding a dental appointment. Anxiety can involve behavioral, emotional, cognitive, and physiological components, and their countenance might differ.1,2,3 [A1] Many terminologies have been used over a while to explain dental anxiety, dental fear, and dental phobia. Dental anxiety and fear are often used indistinctly in the scientific literature, but they both represent contrasting progressive degrees of the same psychological condition. Dental fear is generally associated with known stimuli such as injections or drills, whereas dental anxiety is due to an unknown threat that is not immediately present.4 Dental anxiety is the fifth-most common cause of anxiety and the prevalence of dental fear and anxiety among children ranges from 6% to 42% in different populations.5-10 Various factors and aspects are involved in the development and acquisition of dental anxiety in children. A child's first dental visit is a climacteric moment for the decline or addition of dental anxiety,11 whereas atypical dental anxiety can sometimes relate to a series of uncooperative or troublesome behaviors, given that it can limit children's access to quality oral health care.12 When clinicians treat children with dental anxiety, the former are subjected inevitably to increased stress with more time-consuming procedures, increased costs, and other difficulties encountered during their dental practice.13 Therefore, appropriate management of a child's anxiety during a dental appointment may enhance access to dental care and also subsidize a high quality of dental care, which in turn contributes to the psychological well-being of both the child patient and pediatric dentist.14
The American Academy of Pediatric Dentistry (AAPD) outlined a series of nonpharmacological techniques to deal with a child's behavior in the dental setting.15 Among those, the present trend advocates a simple, safe, cost-effective, and non-aversive approach i.e., distraction.16-19 These distraction techniques seem to can have a positive impact on young individuals' dental fear and anxiety. Robson reported the first documentation of the distraction technique in 1925. The distraction techniques aim to forestall the child's attention from what may be perceived as unpleasant stimuli and shift their focus to exciting and fascinating distractors.20-23 McCaul and Mallot's theory testified that a person's perception of pain decreases when he/ she is distracted from an unpleasant stimulus.24 Distraction techniques can be of two forms i.e., active and passive. Active methods comprise activities that entail the direct participation of the child. They often distract an additional source of sensation i.e., kinesthetic sensation e.g., playing mobile video games and toys.25-28 In contrast, passive techniques rely on practices employing music and video, deprived of involving the child directly, in which children were distracted only using their senses, i.e., vision and hearing, respectively.29,30,31 [A2] Two such widely employed forms of passive distraction in pediatric dentistry are Audio (various categories of music) and Audio-visual distraction (cartoons on TV and two-dimensional video glasses).
A systematic review and meta-analysis by Valverde et al., addressed that VR is a useful distraction technique to reduce anxiety and pain perception in children undergoing dental procedures, thus enlightening the child's behavior towards dental care.32 Ashokan S et al., reported that active distraction plays an important role compared to passive distraction in relieving pain more effectively in children.33 Likewise, Patel et al., observed that video games gained a higher acceptance than parental presence during treatment sessions.25 The accomplishment of the passive distraction technique has been affirmed in medical setups; however scanty literature is accessible to gauge the potency of these techniques in terms of the pediatric population.34 Investigations of visual and auditory distractions in the dental clinic have not reliably found reductions in pain, anxiety, or disruptive behavior.35,36 One possible explanation for these conflicting outcomes is that many of the most communal distracting stimuli (e.g., TV, music) may lack adequate salience to compete for attention as the active distractors alone did not adequately enhance the salience of distraction. One of the best ways to ameliorate the salience of distractors is the addition of a choice component to achieve a receptive child's behavior.37 Hence, the present study was contrived to evaluate the effectiveness of child-centered (choice-based) distraction using three techniques i.e., mobile video games (VG), virtual reality (VR), and mobile cartoons (MC) in the management of a child's dental anxiety during invasive dental procedures.
MATERIALS AND METHODS
Source of data and participants:
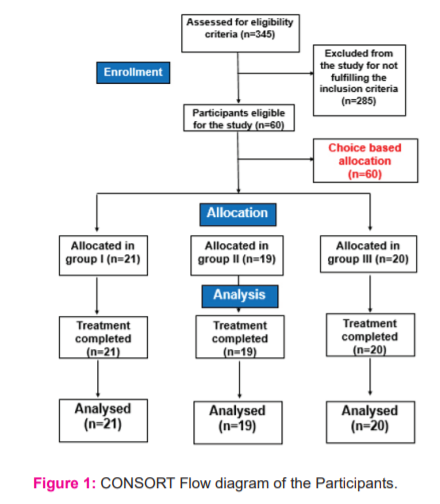
The present self-explanatory trial was conducted in the Department of Pediatric and Preventive Dentistry, Narayana Dental College and hospital, Nellore over three months (August to October of 2019). There were no gender, race, or ethnic restrictions used in the study. Signed informed consent was obtained from the parents or guardians who agreed to participate in the study after providing information regarding the procedures involved. A total of 345 children, who visited the department, were initially examined, of which 60 children who met the following selection criteria were enlisted.
• Healthy children aged 6-12 years
• Children requiring invasive dental procedures
• Children without any previous dental experience.
• Children whose behavior rated as positive (+) or negative (-) based on Wright's modification of the Frankl behavior rating scale.38
• Children who were willing to participate in the study.
Exclusion Criteria:
• Children with any disabilities and underlying systemic diseases.
• Children or parents who refused to participate in the study.
• Children whose behavior rated as definitely positive (++) or definitely negative (--) according to Wright's modification of the Frankl behavior rating scale.
• In addition, to evaluate the independent effects of the distraction, children who required nitrous oxide or general anesthesia were also excluded.
Allocations:
A total of 60 children (40 boys and 20 girls) aged 6-12 years requiring invasive dental procedures were included in the study. Children were allocated based on their choices into three groups: Group-1 mobile video games (VG), Group-2 virtual reality (VR), Group-3 mobile cartoons (MC). In all the groups, children were treated by a single trained dentist within a single appointment using either of the distraction techniques during the execution of invasive dental procedures.
Interventions:
In the VG group (group 1), we initially collected information regarding the most commonly played games by the children in our local region, and those games have installed on the mobile from the IOS store. The games used in this study were friendly, not showing any aggressive, pain, or distress-related content. Before starting the treatment, children were asked to choose their favorite video game, which aids in preventing boredom and keeping attentional by engaging them. Most girls preferred the BarbieTM Magical Fashion game by Budge Studios TM, and boys preferred Temple Run game by Imangi Studios, LLC. Later the children were asked to play the video game of their choice during the treatment sessions.
In the VR group (group 2), children were given a few minutes to get accustomed to the eyeglasses. These 3D VR eyeglasses (ALDIVO R Virtual Reality Glasses 3D VR Box headsets for 3.5- 6 "mobile phones, model no: a236, India) helps in blocking the visual field of the child entirely and had in-built headphones to deliver the sound effectively to avoid hearing any voices and helps in distraction. The children were asked to choose their favorite videos on the phone, where most of the children preferred Doraemon cartoon videos. Later, 3D VR glasses were mounted to the mobile phone (Apple iPhone 7 Plus, California) capable of playing MP4 audiovisual files. Once the VR device was secured on the child's eyes, cartoon videos are played.
In the MC group (group 3), children were provided with a mobile phone and headset for better audio as a means of distraction, where they opted to view their favorite cartoon videos in the regional language.
Materials for measuring a child's anxiety:
RMS Pictorial Scale (RMS-PS): The RMS-PS is anxiety measuring scale consists of original photographs of both boy and a girl child. RMS-PS consist of five faces from very happy to very unhappy. The children were asked to choose a face that closely resembles how they feel like at that moment. This was recorded by giving a value one to the very happy face and five to very unhappy face.39 Pre and Post-operative anxiety were measured using an RMS pictorial scale. Anxiety levels before, during, and after the treatment procedure was assessed by recording the heart rate (physiologic measurement) using a Portable Non-Invasive Fingertip pulse oximeter device (EZ- LIFE Professional PD- 10*7*5 cm. ASIN B084TQQTVN).40 A single dentist who was blinded to the allocation procedure recorded both the heart rate and the RMS scores for all the children.
Outcomes measures:
1. The primary outcome measure considered was the Pulse (heart) rate, which is a physiological parameter
2. The secondary outcome measured was pre and post-operative anxiety using the RMS pictorial scale.
Statistical methods:
All statistical analyses were performed using standard software (SPSS 20.0 for Windows, SPSS Inc., Chicago, USA). Kruskal Wallis- ANOVA and Wilcoxon Sign Rank Test was used to analyze the Intergroup and Intragroup comparison of pre-op and post-op RMS Scores.
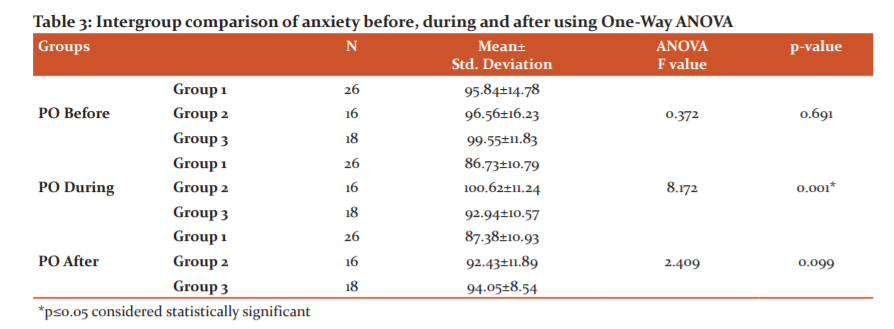
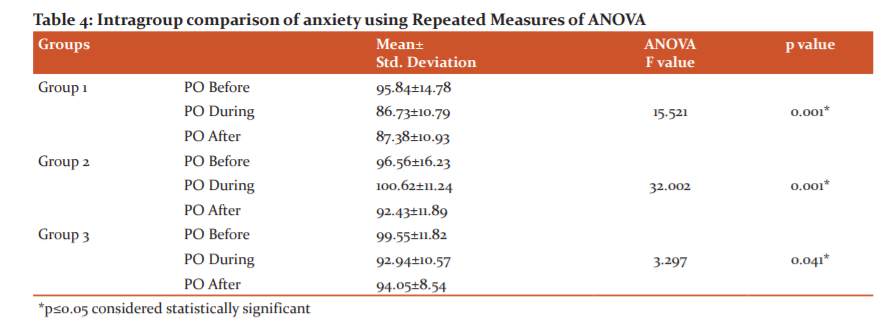
Intergroup comparison of anxiety before, during, and after was analyzed using One-Way ANOVA. Whereas, for Pair-wise comparison of Anxiety in Group I, II, III LSD Bonferroni Test was used. Intragroup comparison of anxiety was assessed using Repeated Measures of ANOVA, and for Pair-wise comparison of Anxiety Tukey's Post Hoc Analysis was used.
P-value < 0.05 was considered statistically significant.
RESULTS:
The recruitment, randomization, allocation, and completion of children in different groups were represented in the flow diagram.
Intervention Effectiveness:
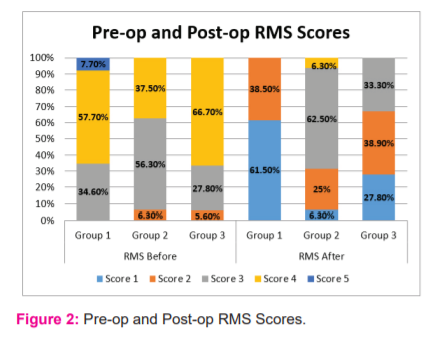
Intergroup Pre-operative anxiety measured for children in all the groups on a subjective scale, i.e., RMS pictorial scale, showed no significant differences among them. However, a significant difference was elicited for post-operative anxiety among all the three groups, children in the first group exhibited fewer anxiety scores than the counterpart. (Table 1)
Intragroup comparison of pre and post-operative anxiety scores showed a significant difference for the children in group I and group III. It was not significant for the children in group II (P-value ≤ 0.004). (Table 2)
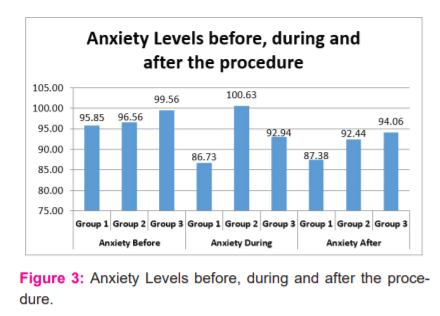
The children's intergroup comparison of pre and post anxiety scores didn't illustrate any statistically significant difference among them. In contrast, a significant difference was exhibited for the anxiety scores during the procedure. (Table 3)
For the Intragroup comparison of anxiety scores, a significant difference was elicited for all the children in three groups. But upon keen evaluation of the Mean +- SD values, there was more decrease in the mean +-SD. Values compared to other groups. (Table 4)
Discussion
Anxiety and fear due to dental treatment, affect 15% - 20% of the population, being recognized by the World Health Organization (WHO).41, 42 It poses a significant problem for children who are affected by it, resulting in avoidance of even the most primary dental treatments, such as simple dental check-ups or cleanings.43 Thus, its management is essential to enhance the child's oral health quality of life.44 The dentists and the parents accepted variety of behavior guidance techniques adopted by American Academy of Pediatric Dentistry, among that distraction is one of the contemporary technique which is capable reducing anxiety by engaging the child most effectively during their first dental visit.45 Ideal distracters would require an optimal amount of attention involving multiple sensory modalities (kinesthetic, visual, and auditory), active emotional involvement, and participation of the child to compete with the signals from the noxious stimuli.46,47 The most common distracting stimuli (e.g., TV, music, mobile) may lack adequate salience to compete for attention. In other words, common distracters may not be loud enough, close enough, or interesting enough to hold a child's attention in distracting him/her from the dental environment. Thus, one way to improve the effectiveness of Distraction may be to increase the salience of the distractors.37 Mainly the value of the distracting stimulus is linked closely to its quality, which usually is determined by the preference of the participant.48 Thus, one means of enhancing the effectiveness of a distracter may be to stick on the preference of the children by providing choices pertaining to the available distracters.49 This necessitates the need for research that improve insights to existing distraction techniques. Hence, present study was aimed to evaluate the effectiveness of child centered distraction (choice based) techniques in the management of a child's dental anxiety and fear based on their preferences. None of the children in the present study had previous exposure to dental treatment, and high levels of anxiety was observed before commencing the procedure it was consistent with the study reported by Alvin et al., Mason et al.50,51 Primarily, anxiety and fear of unknown situations predispose children to consider dental circumstances to be challenging.
In the present study, irrespective of the distraction methods used, there was an overall reduction in the reported Raghavendra Madhuri Sujatha (RMS) scores, which indicates a decline in the anxiety levels of children after the dental procedures. Two forms of distraction i.e., active and passive which include playing video games on a mobile phone, and Audio-visual distraction with/without VR glasses respectively were used in this study. Although it has hypothesized that active strategies are more effective than passive, other studies suggest that passive distraction was useful or even better since the active forms are too demanding for children.52, 53
Likewise, in this study, playing a Mobile phone video game, which acts as an active distraction technique, reduces a child's anxiety better than passively watching the cartoon with or without VR glasses. This reduction in anxiety scores can be explained as stated by Koepp et al.,54 that endogenous dopamine is released and bound to receptors in the human striatum during a goal-directed motor task like VG playing. Dopaminergic neurotransmission might be involved in learning reinforcement of behavior, attention, and sensorimotor integration. Likewise, a randomized cross-over trial by Shah et al.,55 concluded that pre-procedural gaming resulted in a statistically significant difference in hemodynamic parameters of 60 children between 5 and 10 years old. Coinciding with this, we witnessed a substantial reduction in mean pulse rates in children who had their treatments while playing mobile video games.
As per the findings of the present study, anxiety scores in children have also been reduced using audiovisual distraction (AVD), which might be due to the partial visual obstruction of the operating environment.56 There were few adverse effects of AVD in literature stating their concerns towards pain experience during dental visits of children.57,58 The anxiety scores of mobile gaming has shown high significance when compared to AVD which was reflected not only in the Heart rate scores (physiological) but also in the RMS scores. These results were consistent with Attar et al.,59 who suggested that passive distraction, such as watching a film, is not as effective as an active distraction (e.g., playing a video game) in reducing patient anxiety. In this study, we found that there seems no significant difference in anxiety found between both boys and girls. This is because of the reason that we ensured the availability of games that girls would find interesting. These findings are similar to Nuvvula et al.,60 but Khotani et al.,61 reported that girls showed a more significant reduction in anxiety when compared with the boys. Virtual reality immersion was shown to be somewhat more effective than audiovisual distraction because it augments detachment from viewing and hearing what is happening in the environment.62,63 In this study, mobile phone video games were mostly preferred instead of virtual reality eyewear as most of the children in the study population had not exposed to a sophisticated device. VR glasses are not well known among kids of all age ranges and socioeconomic groups. Even though there was a reduction of postoperative anxiety in a child using VR, procedural anxiety was increased in the VR group as these had blocked the vision of the child, making him/ her anxiety about not knowing what was going around them during the dental procedures. Nausea, headache, and interference to communicate with the children were some of the other problems encountered.
Sullivan et al.,64 discovered that although VR had no significant effect on children's behavior or anxiety during dental treatment, VR did considerably lower their pulse rates. Since, the children in the present study had the opportunity of choosing their preferred cartoon and games, one can believe that this can compensate for the lack of salience in distractors. Nevertheless, asking the child to choose the distraction can provide him/her in having a sense of control during dental treatment, which in turn assists in reducing the chance of uncooperative behavior. This coincides with a study by Filcheck et al.,65 where the authors concluded that choice-based distraction is a relatively practical method to implement, a valuable alternative technique to the health care professionals and parents in reducing the distress of children who visit the dentist. Most children were satisfied and comfortable with the distractors provided and used in this study, which are safe, clinically feasible, and easy to operate without any prior training for the clinicians.
But certain limitations were noted in this study, primarily regarding with the usage of same sized VR glasses for children with small face/head size, because of their unavailability of different sizes and a small sample size.
CONCLUSION:
From the above observations, the following findings were drawn:
1. Primarily, distraction techniques of choice-based could be an effective method in reducing a child's dental anxiety. Allowing the child to choose the distraction technique by him/herself instills a positive attitude in a child's mind that he/she actively participates in the dental procedure, thus reducing dental anxiety.
2. Secondly, Mobile video gaming, which is an active, cost-effective and readily available technique, also well known among children in all socioeconomic groups, could be a better alternative to all other distraction techniques used in the dental operatory.
Conflict of interest: NIL
Source of funding: NIL
Author contribution:
-
Varada Sahithi (Conceptualization; Writing – original draft)
-
Sainath Reddy Elicherla (Data curation; Writing – original draft)
-
Kanamarlapudi Venkata Saikiran (Data curation; Writing – review & editing)
-
Ramasubba reddy Challa (Formal analysis; Supervision)
-
Sivakumar Nuvvula (Writing – review & editing)

References:
-
Armfield JM, Heaton LJ. Management of fear and anxiety in the dental clinic: a review. Aust Dent J. 2013;58:390?407.
-
Edition F. Diagnostic and statistical manual of mental disorders. Am Psychiatric Assoc. 2013; 23: 63-67.
-
Serra?Negra J, Paiva SM, Oliveira M, Ferreira E, Freire?Maia F, Pordeus I. Self?reported dental fear among dental students and their patients. Int J Environ Res Public Health. 2013;9:44?54.
-
Nigam AG, Marwah N, Goenka P, Chaudhry A. Correlation of general anxiety and dental anxiety in children aged 3 to 5 years: A clinical survey. J Int Oral Health. 2013; 5:18.
-
Agras S, Sylvester D, Oliveau D. The epidemiology of common fears and phobia. Compr Psychiatry. 1969;10:151-156.
-
Akbay Oba A, Dulgergil CT, Sonmez IS. Prevalence of dental anxiety in 7? to 11? year?old children and its relationship to dental caries. Med Princ Pract. 2009;18:453?457.
-
Kakkar M, Wahi A, Thakkar R, Vohra I, Shukla AK. Prevalence of dental anxiety in 10–14 years old children and its implications. J Dent Anesth Pain Med. 2016;16:199?202.
-
Silveira ER, Goettems ML, Demarco FF, Azevedo MS. Clinical and Individual Variables in Children’s Dental Fear: A School? Based Investigation. Braz Dent J. 2017;28:398?404.
-
Soares FC, Lima RA, Barros M, Dahllöf G, Colares V. Development of dental anxiety in schoolchildren: a 2?year prospective study. Community Dent Oral Epidemiol. 2017;45: 281-288.
-
Berge M, Veerkamp J, Hoogstraten J, Prins PJ. Childhood dental fear in the Netherlands: prevalence and normative data. Community Dent Oral Epidemiol. 2002;30:101?107.
-
Elicherla SR, Bandi S, Nuvvula S, Saikiran KV, Priyanka VJ. Comparative evaluation of the effectiveness of a mobile app (Little Lovely Dentist) and the tell-show-do technique in the management of dental anxiety and fear: a randomized controlled trial. J Dent Anesth Pain Med. 2019;19:369-378.
-
Moore R, Brodsgaard I. Dentists’ perceived stress and its relation to perceptions about anxious patients. Community Dent Oral Epidemiol. 2001;29:73-80.
-
Rafique S, Banerjee A, Fiske J. Management of the petrified dental patient. Dent Update. 2008;35:196-207.
-
Bankole OO, Aderinokun GA, Denloye OO, Jeboda SO. Maternal and child’s anxiety – effect on child’s behaviour at dental appointments and treatments. Afr J Med Med Sci. 2002; 31:349–352.
-
American Academy of Pediatric Dentistry. Behavior guidance for the pediatric dental patient. Reference Manual of Pediatric Dentistry. Chicago, Ill: Pediatr Dent. 2019:266-279.
-
Al- Khotani A, Bello LA, Christidis N. Effects of audiovisual distraction on children’s behaviour during dental treatment: A randomized controlled clinical trial. Acta Odontol Scand. 2016;74:494-501.
-
Singh D, Samadi F, Jaiswal JN, Tripathi AM. Stress reduction through audio distraction in anxious pediatric dental patients: an adjunctive clinical study. Int J Clin Pediatr Dent. 2014;7:149?152.
-
Asl Aminabadi N, Erfanparast L, Sohrabi A, Oskouei SG, Naghili A. The impact of virtual reality distraction on pain and anxiety during dental treatment in 4–6-year-old children: a randomized controlled clinical trial. J Dent Res Dent Clin Dent Prospect. 2012;6:117?124.
-
Srouji R, Ratnapalan S, Schneeweiss S. Pain in children: assessment and nonpharmacological management. Int J Pediatr. 2010;20(11):474-483.
-
Robson CH. Anesthesia in children. Anesth Analg. 1925;7:235-237.
-
Pinkham JR. Behavior management of children in the dental office. Dent Clin North Am. 2000;44:471?486
-
Lambert SA. Distraction, imagery, and hypnosis. Techniques for management of children’s pain. J Child Fam Nurs. 1999;2:5-15.
-
Kleiber C, McCarthy AM. Evaluating instruments for a study on children’s responses to a painful procedure when parents are distraction coaches. J Pediatr Nurs. 2006;21:99-107.
-
McCaul KD, Malott JM. Distraction and coping with pain. Psychol Bull. 1984;95:516-533.
-
Patel A, Schieble T, Davidson M, Tran MC, Schoenberg C, Delphin E, Bennett H. Distraction with a hand?held video game reduces pediatric preoperative anxiety. Paediatr Anaesth. 2006;16:1019-1027.
-
Weydert JA, Shapiro DE, Acra SA, Monheim CJ, Chambers AS, Ball TM. Evaluation of guided imagery as treatment for recurrent abdominal pain in children: a randomized controlled trial. BMC Pediatr. 2006;6:29-38.
-
Peretz B, Gluck GM. Assessing an active distracting technique for local anesthetic injection in pediatric dental patients: repeated deep breathing and blowing out air. Int J Clin Pediatr Dent. 1999;24:5-8.
-
Nilsson S, Finnstrom B, Kokinsky E, Enskar K. The use of Virtual Reality for needle-related procedural pain and distress in children and adolescents in a paediatric oncology unit. Eur J Oncol Nurs. 2009;13:102-109.
-
Marwah N, Prabhakar AR, Raju OS. Music distraction-its efficacy in management of anxious pediatric dental patients. J Indian Soc Pedod Prev Dent. 2005;1;23:168.
-
Aitken JC, Wilson S, Coury D, Moursi AM. The effect of music distraction on pain, anxiety, and behavior in pediatric dental patients. Pediatr Dent. 2002;24:114-118.
-
Prabhakar AR, Marwah N, Raju OS. A comparison between audio and audiovisual distraction techniques in managing anxious pediatric dental patients. J Indian Soc Pedod Prev Dent. 2007;25:177-182.
-
Lopez-Valverde N, Muriel Fernández J, Lopez-Valverde A, Valero Juan LF, Ramírez JM, Flores Fraile J, et al. Use of Virtual Reality for the Management of Anxiety and Pain in Dental Treatments: Systematic Review and Meta-Analysis. J Clin Med. 2020;9:1025.
-
Asokan S, Geetha Priya P R, Natchiyar S N, Elamathe M. Effectiveness of distraction techniques in the management of anxious children – A randomized controlled pilot trial. J Indian Soc Pedod Prev Dent. 2020;38:407-412.
-
Naithani M, Viswanath D. Child’s Dental Anxiety: Management by Audio and Audiovisual Distraction Technique - A Comparative Study. Univ Res J Dent. 2014; 4:101-107.
-
Ingersoll BD, Nash DA, Blount RL, Gamber C. Distraction and contingent reinforcement with pediatric dental patients. J Dent Child. 1984;51:203-207.
-
Venham, LL, Goldstein M, Gaulin-Kremer E, Peteros K, Cohan J, Fairbanks J. Effectiveness of a distraction technique in managing young dental patients. Pediatr Dent. 1981;3:7-11.
-
Hoge MA, Howard MR, Wallace DP, Allen KD. Use of video eyewear to manage distress in children during restorative dental treatment. Pediatr Dent. 2012;34:378?382.
-
Townsend JA. Behavior guidance of the pediatric dental patient. Pediatric Dentistry: Infancy through Adolescence. 5th ed. Philadelphia: Elsevier Saunders. 2013:358.
-
Aitken RC. A growing edge of measurement of feelings using visual analog scales. Proc Roy Soc Med. 1969;62:989-993.
-
Yelderman M, New W Jr. Evaluation of pulse oximetry. Anaesthesiology. 1983;59:349-352.
-
Seligman LD, Hovey JD, Chacon K, Ollendick TH. Dental anxiety: An understudied problem in youth. Clin Psychol Rev. 2017;55:25-40.
-
Hill KB, Chadwick B, Freeman R, O’Sullivan I, Murray JJ. Adult Dental Health Survey 2009: Relationships between dental attendance patterns, oral health behaviour and the current barriers to dental care. Br Dent J. 2013;214 :25-32.
-
De Stefano R. Psychological Factors in Dental Patient Care: Odontophobia. Medicina. 2019;55: 678.
-
Fiorillo L. Oral Health: The First Step to Well-Being. Medicina. 2019;55:676.
-
Nunna M, Dasaraju RK, Kamatham R, Mallineni SK, Nuvvula S. Comparative evaluation of virtual reality distraction and counter-stimulation on dental anxiety and pain perception in children. J Dent Anesth Pain Med. 2019;19:277-288.
-
Peretz B, Efrat J. Dental anxiety among young adolescent patients in Israel. Int J Paediatr Dent. 2000;10:126-132.
-
Rantavuori K, Lahti S, Seppa L, Hausen H. Dental fear of Finnish children in the light of different measures of dental fear. Acta Odontol Scand. 2005;63:239-244.
-
Neef NA, Mace FC, Shea MC, Shade D. Effects of reinforcer rate and reinforcer quality on time allocation: Extensions of matching theory to educational settings. J Appl Behav Anal. 1992;25:691-699.
-
Kazdin AE. Progression of therapy research and clinical application of treatment require better understanding of the change process. Clin Psychol: science and practice. 2001;8:143-151.
-
Rodolfa ER, Kraft W, Reilley RR. Etiology and treatment of dental anxiety and phobia. Am J Clin Hypn. 1990;33:22-28.
-
Alwin NP, Murray JJ, Britton PG. An assessment of dental anxiety in children. Br Dent J. 1991;17:201-207.
-
Mason S, Johnson MH, Wooley C. A comparison of distractors for controlling distress in young children during medical procedures. J Clin Psychol Med. 1999;6:239-248.
-
Dahlquist LM, McKenna KD, Jones KK, Dillinger L, Weiss KE, Ackerman CS. Active and passive distraction using a head-mounted display helmet: effects on cold pressor pain in children. Health Psychol. 2007;26:794-801.
-
Koepp MJ, Gunn RN, Lawrence AD, Cunningham VJ, Dagher A, Jones T, Brooks DJ, Bench CJ, Grasby PM. Evidence for striatal dopamine release during a video game. Nature. 1998;393:266-268.
-
Shah HA, Nanjunda Swamy KV, Kulkarni S, Choubey S. Evaluation of dental anxiety and hemodynamic changes (Sympathy- Adrenal Response) during various dental procedures using smartphone applications v/s traditional behavior management techniques in pediatric patients. Int J Adv Res. 2017;3:429-433.
-
Ram D, Shapira J, Holan G, Magora F, Cohen S, Davidovich E. Audiovisual video eyeglass distraction during dental treatment in children. Quintessence Int. 2010;41:673-679.
-
Mitrakul K, Asvanund Y, Arunakul M, Paka-aka Kapha S. Effect of audiovisual eyeglasses during dental treatment in 5?8-year-old children. Eur J Pediatr Dent. 2015;16: 239- 245.
-
Fakhruddin KS, El Batawi H, Gorduysus MO. Effectiveness of audiovisual distraction eyewear and computerized delivery of anesthesia during pulp therapy of primary molars in phobic child patients. Eur J Dent. 2015;9:470?475.
-
Attar RH, Baghdadi ZD. Comparative efficacy of active and passive distraction during restorative treatment in children using an iPad versus audio-visual eyeglasses: a randomized controlled trial. Eur Arch Paediatr Dent. 2015;16:1-8.
-
Nuvvula S, Alahari S, Kamatham R, Challa RR. Effect of audio-visual distraction with 3D video glasses on dental anxiety of children experiencing administration of local analgesia: a randomized clinical trial. Eur Arch Pediatr Dent. 2015;16:43-50.
-
Al-Khotani A, Bello LA, Christidis N. Effects of audiovisual distraction on children’s behavior during dental treatment: a randomized controlled clinical trial. Acta Odontol Scand. 2016;74:494-501.
-
Leibovici V, Magora F, Cohen S, Ingber A, Effects of virtual reality immersion and audiovisual distraction techniques for patients with pruritus. Pain Res Manag. 2009;14: 283-286.
-
Shafi S, Manzoor S, Kaushik N. Distraction using virtual reality technology: A review. Int J Curr Adv Res. 2015;3:1465-1468.
-
Sullivan C, Schneider PE, Musselman RJ, Dummett CO, Gardiner D. The effect of virtual reality during dental treatment on child anxiety and behavior. ASDC J Dent Child. 2000;67:193-196.
-
Filcheck HA, Allen KD, Ogren H, Darby JB, Holestin B, Hupp S. et al. The use of choice-based distraction to decrease the distress of children at the dentist. Child Fam Behav Ther. 2005;26:59-68.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





