IJCRR - 13(16), August, 2021
Pages: 179-183
Date of Publication: 30-Aug-2021
Print Article
Download XML Download PDF
Evolving Trends in Physical Therapy Management in the Prevention of Knee Osteoarthritis from Mild to Moderate Grade: A Systematic Review
Author: Sowmya Madayi Veetil, Kotteeswaran Kandaswami, Vikram Adhitya Pathamadai Selvakumar
Category: Healthcare
Abstract:Introduction: Knee osteoarthritis (KOA) affects a large number of people, the world over especially the female population in their old age. As no proper remedy is available on the date, people prefer non-invasive treatments to overcome this malady. Physiotherapy approaches have been recognized as beneficial to the affected. Though the current intervention packages offer satisfactory results, a better treatment modality is proposed in this report. The main objective is to determine the effect of Physical Therapy management in preventing Knee Osteoarthritis from mild to moderate. Aim: This study aims to evaluate the evolving trends in physical therapy management in the prevention of knee osteoarthritis from mild to moderate grade. Methods: We included systematic reviews published between December 2000 and December 2019 that examined any physical therapy intervention for patients with osteoarthritis of the knee. We included reviews on patients with osteoarthritis in general if results from patients with knee osteoarthritis could be extracted separately. We excluded reviews with major limitations. Instruments and scales for assessment of the methodological quality of Randomized Control Trials (RCT) in the reviews (Eg: Jadad scale, PEDro scale) were extracted and entered into the table of characteristics. Results: A total of 23 review articles have examined the evolving trends in Physical therapy management in the prevention of osteoarthritis of the knee. These studies show high-quality evidence that exercise improves physical function and reduces pain. The reviews did not find any effect on psychological outcomes. The overview of this review on physical therapy interventions for patients with osteoarthritis of the knee is based on a thorough literature search, assessment of study quality, and synthesis of findings. Conclusion: Exercise, including a weight reduction program for patients who are obese, seems to be a valuable treatment option for patients with pain and functional problems due to osteoarthritis of the knee
Keywords: Exercise, Laser therapy, Pain, Osteoarthritis, Ultrasound, Weight reduction.
Full Text:
INTRODUCTION
Knee osteoarthritis is the most common cause of functional limitation and pain in the knee joint which causes huge impact in human beings.1Exercise programs have been shown to be effective when patients are closely supervised by physiotherapists.27 The OA of knee joint mainly affects the active daily living activity of a person.2 Certain studies done previously suggest that there is a marked decrease in the aerobic capacity among the patients with OA knee when compared to people who are not affected by Osteoarthritis (OA) knee. The most common manifestations of OA knee are pain and muscle weakness which in turn causes decreased physical activity and results in negative health outcome. The OA knee which causes decreased physical activity may lead to many associated health problems like cardiovascular disease, chronic co-morbidity, musculoskeletal disorder, and reduced quality of life.3 Recent studies have suggested us that people with OA knee are making enough effort to execute the management with support from their health care provider. The early intervention is very important to prevent the further progression of the disease and improve the quality of life.4
Recent studies also suggest that there is a decrease in the muscle strength of hamstring and quadriceps among the patients with OA knee. The cause for the weakness is unknown but the main cause which appears is due to disuse dystrophy and activation deficits.5 This has been observed that there is more emphasize given on the quadriceps strengthening than the hamstrings. The hamstring muscle also provides the structural and functional stability to the knee joint and thus the hamstring strengthening is very important.6 There are very few studies done on the effect of the hamstring muscle strengthening among the OA knee patients and we would recommend an intensive research to be done in order to provide us a valid tool to prevent the progression of OA knee from mild grade of severity to moderate level.
There are various biomechanical factors which are involved in the progression of the disease. The major biomechanical factor which is responsible for the progression of the OA knee is the ankle rotation.7 Acute joint loading factor will cause damage to the joint tissue and lead to OA knee. External knee adduction movement during walking is one of the most correlated biomechanical factors which cause the medial compartment loading and lead to OA knee. To reduce the loading on the medial side and to overcome the pain the patient walk with externally rotated foot.8 There is another way to reduce the medial loading by increasing the lateral hamstring activation and decreasing the medial hamstring activation.9
Various treatment strategies for OA knee included pharmacological, non - pharmacological, surgical management. The physical therapy includes the treatment with the help of exercise, braces and orthosis, Transcutaneous Electrical Nerve stimulation, Thermotherapy, laser therapy, electrical stimulation, and ultrasound.10 The burden of knee OA alone is particularly high and is on the rise.11,12 There are various treatment strategies which are available for treating OA knee. This review mainly aims to find the modern and evidence based treatment strategies available for the treatment of OA knee. The main objective is to find the treatment to prevent the progression and severity of OA knee from mild to moderate.Therefore; it is of paramount importance to keep updating OA management guidelines so as to provide the best possible evidence-based management in the primary setting. This may help to delay progression into end-stage OA and thus decrease the need for arthroplasty and alleviate post-surgical complications.13,14
METHODS
ELIGIBLITY CRITERIA
We included systematic reviews published between December 2000 and December 2019 that examined any physical therapy intervention for patients with osteoarthritis of the knee. We included reviews on patients with osteoarthritis in general if results from patients with knee osteoarthritis could be extracted separately. Reviews on all types of physical therapy interventions (Eg: exercise, physical modalities, and patient education) were included. For the purpose of this overview, we have considered pain and physical function as primary outcomes, but we also have included psychological outcomes (Eg: scales of psychological disability or self-efficacy), as this information might be important to patients. The concept of “function” is based on the International Classification of Functioning, Disability and Health (ICF) where “function” is an umbrella term for body function, body structure, activities, and participation. We included only reviews published in English.
INFORMATION SOURCES
We searched the Cochrane Library (Cochrane Database of Systematic Reviews and DARE), MEDLINE, EMBASE, and PEDro for systematic reviews published from December 2000 to December 2019. In MEDLINE and EMBASE a filter based on the SIGN filters was used to identify reviews. In PEDro and the Cochrane Library, the searches were restricted to terms in the record title, abstract, or key words. In addition, we screened the reference lists of included studies. We did an updated search in the Cochrane Database of Systematic Reviews and MEDLINE in December 2019.
IDENTIFYING RELEVANT REVIEWS AND ASSESSMENT OF METHODOLOGICAL QUALITY
Two reviewers independently assessed the relevance of all references based on abstracts, read the full text of relevant reviews, and assessed the methodological quality of included reviews using a modified version of a previously validated checklist. Nine criteria related to search strategy, inclusion criteria, quality assessment, combining of studies, and conclusion were rated as “met,” “unclear/ partly met,” or “not met.” Disagreement was resolved by discussion between the 2 reviewers. Based on a summary of these 9 criteria, an overall scientific quality of each review was labelled as “minor limitations” (at least 7 of the criteria met), “moderate limitations” (at least 4 of the criteria met), or “major limitations” (fewer than 4 of the criteria met). We excluded reviews with major limitations. Data Extraction and Synthesis was done by one author. The author independently extracted data from each included review and discussed the data with the other author. Instruments and scales for assessment of methodological quality of RCTs in the reviews (Eg: Jadad scale, PEDro scale) were extracted and entered into the table of characteristics of included reviews.
PRISMA DIAGRAM
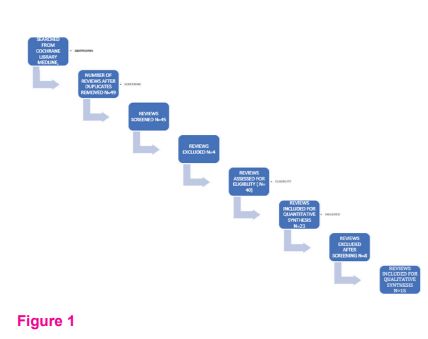
FIGURE NO:1
The literature search identified 1,027 relevant reviews (301 from MEDLINE, 552 from EMBASE, 114 from the Cochrane Library, and 60 from PEDro). After screening of abstracts, 49 reviews were retrieved in full text. Finally, 13 reviews fulfilled the inclusion criteria and were included in the overview. Characteristics and results of included reviews are presented in Table.1. The reviews covered the following topics: exercise, psychoeducational interventions, braces and orthoses, electromagnetic field, weight reduction, acupuncture, transcutaneous electrical nerve stimulation, low-level laser therapy, ultrasound, thermotherapy, electrical muscle stimulation, and balneotherapy. Sixteen of the reviews were of high quality (minor limitations), and 7 reviews were of moderate quality.
RESULTS:
Exercise
Exercise therapy can be performed actively, passively, or against resistance.15 Two reviews concluded that there was no difference in effect between aerobic exercise (including walking) and strengthening exercise. Another review included one study that compared high and low intensity exercise (stationary cycling) and found no difference in any outcome. From a descriptive summary of 7 RCTs on patients with osteoarthritis (2 studies on knee osteoarthritis), the authors concluded that interventions to enhance self-efficacy and social support are necessary to foster exercise adherence among people with osteoarthritis. All reviews concluded that exercise reduces pain and improves physical function.16 The effects are considered small to moderate in both high and moderate quality reviews. Thus, we conclude that there is high-quality evidence that exercise improves physical function and reduces pain. The reviews did not find any effect on psychological outcomes.
Weight Reduction
One recently published review evaluated the effect of weight reduction in patients with obesity who were diagnosed with osteoarthritis of the knee.The authors concluded that for obese patients with OA, a rapid reduction of atleast 10% of body weight must be prescribed. The challenge of how to maintain weight loss, and further research is required on how weight loss impacts a patient with osteoarthritis.26,17
Electromagnetic Field
The effects of pulsed electromagnetic energy and electromagnetic fields were presented in 2 reviews. These results suggest that Pulsed electromagnetic field therapy (PEMF) is effective for pain management in knee Osteoarthritis patients and also affects pain threshold and physical functioning. Current evidence suggests that electrical stimulation therapy may provide significant improvements for knee OA, but further studies are required to confirm whether the statistically significant results shown in these trials confer to important benefits.18
Transcutaneous Electrical Nerve Stimulation
One review compared transcutaneous electrical nerve stimulation with a conservative intervention. Those studies revealed a reduction in pain after transcutaneous electrical nerve stimulation compared with the conservative intervention.19 We conclude that there is moderate-quality evidence that transcutaneous electrical nerve stimulation reduces pain compared with a conservative intervention.
Balneotherapy
One review including 3 RCTs evaluated different types of balneotherapy. The authors concluded that baths seems to have a short-term benefit for pain relief compared with tap water. Based on few studies and heterogeneous results.20 We conclude that the effect of balneotherapy is unclear and has low-quality evidence.
Thermotherapy
One review included on the effects of heat packs, cold packs, or ice massage. All studies had small sample sizes and low quality. The results for pain or function are not consistent, and we conclude that Ice massage compared to control had a statistically beneficial effect on ROM, function and knee strength. Cold packs decreased swelling. Hot packs had no beneficial effect on oedema compared with placebo or cold application. Ice packs did not affect pain significantly, compared to control, in patients with OA.21
Low-Level Laser Therapy
We originally included 2 reviews on low-level laser therapy but in the updated search we found that the Cochrane Review on low-level laser therapy was withdrawn because it needed to be updated. Thus, only one review summarizing low-level laser therapy for knee osteoarthritis is included. The meta-analysis of 7 RCTs concluded that laser therapy reduced pain and improved function compared with a placebo intervention.22 We conclude that there is moderate-quality evidence that low level laser therapy reduces pain and improves function.
Psychoeducational Interventions
Three reviews summarized studies on self-management, psychoeducational interventions, and patient education. In the most updated review by R Marks and JP Allegrante. et al, The most effective psychoeducational interventions must be preceded by careful assessment of the patient, including their own goals and objectives.23 The most useful interventions are likely to be those that can influence emotional regulation and those that provide social support. We conclude that there is moderate-quality evidence that psychoeducational interventions improve psychological outcomes.
Braces and Orthoses
One review evaluated the effect of braces and orthoses. R W Brouwer 1, T S C Jakma, A P Verhagen, J A N Verhaar, S M A Bierma-Zeinstra in his review regarding the efficacy of braces and orthoses to reduce the pain. Two out of 3 studies selected were high end reviews where they concluded that NSAID intake is reduced with a laterally wedged insole compared with a neutral insole. [24]
DISCUSSION:
This overview on physical therapy interventions for patients with osteoarthritis of the knee is based on a thorough literature search, assessment of study quality, and synthesis of findings. One extensive overview of the effectiveness of exercise therapy was published earlier but to our knowledge no overview has used our explicit and systematic method. Only exercise for reducing pain and improving function and weight loss for disability were supported by high-quality evidence. Transcutaneous electrical nerve stimulation, and low level laser therapy for pain reduction were graded as moderate-quality evidence, although they were all close to high quality. For other interventions and outcomes, the quality of evidence was assessed as moderate, low, or no evidence from systematic reviews. New trials are needed within these areas. For a few interventions, no systematic review was identified.
Exercise therapy was covered in 2 reviews and it is well stated that most patients with osteoarthritis receive exercise as part of their treatment and physical therapists need updated evidence concerning type, frequency, and dose of optimal exercise. Many of the reviews concluded that both aerobic and strengthening exercise as well as individual and group exercises was effective in patients with knee osteoarthritis. One review concluded that weight reduction decreased pain and improved self-reported disability for patients who are obese. The intervention was carried out as a nutrition class and was combined with cognitive behavioural therapy. We included this review because physical therapists play an important role in supporting people to lose weight. Based on the high-quality evidence for weight loss and exercise, physical therapists should consider collaborating with dietitians in order to reduce pain and improve function in patients with osteoarthritis of knee.
It is also important for clinicians and policy makers not to interpret low-quality evidence as evidence of no effect. Low-quality evidence means unclear evidence, and findings should initiate more research and reviews. It was difficult to extract data on methodological quality and results from some reviews because of poor reporting. Authors of systematic reviews should use explicit and systematic methods for including, finding, assessing, and summarizing evidence although a meta-analysis cannot always be performed. We strongly encourage authors of systematic reviews to make a synthesis of the results instead of summarizing study by study only.
In this overview, 7 out of 15 included reviews come from 2 research teams. Whether this could introduce a source of bias is difficult to estimate, but it should be kept in mind. We included 15 reviews in this overview. Clinical guidelines often are based on evidence from systematic reviews; therefore, we need more reviews. From 1999 to 2006, the number of included reviews in the PEDro database increased from 200 to more than 1,400.
Physical therapy interventions might be useful for people with osteoarthritis of knee. This study also concluded that there was a mismatch between the amount of research and the degree of interest from consumers. A recent systematic review of the course of functional status and pain in people with osteoarthritis of the hip and knee showed increased muscle strength (force generating capacity) and better self-efficacy.
CONCLUSION
The findings and conclusions from the present overview confirm that physical therapy is beneficial for patients with osteoarthritis of the knee, but more research is needed as a means of evidence-based practice. Exercise which focus mainly on improving the muscle strength of both hamstrings, quadriceps and indirectly strengthening the ankle rotators to prevent the unwanted joint loading to the knee also proves beneficial in reducing the severity from mild grade to moderate grade of knee OA. A well-defined program such as weight reduction sessions for patients who are obese, seems to be a valuable treatment option for patients with pain and functional problems due to osteoarthritis of the knee.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Ethical Clearance: NA
Informed Consent: NA
Source of Funding: None
Conflict of interest: NIL
References:
[1] Neogi T, Magnetic resonance imaging-based three-dimensional bone shape of the knee predicts onset of knee osteoarthritis: data from the osteoarthritis initiative. Arthritis Rheum. 2013 Aug;65(8):2048-58.
[2] Covinsky K. Aging, arthritis, and disability. Arthritis Rheum. 2006 Apr 15;55(2):175-6.
[3]Bindawas SM, Vennu V, Auais M. Health-related quality of life in older adults with bilateral knee pain and back pain: data from the Osteoarthritis Initiative. Rheumatol Int. 2015 Dec;35(12):2095-101.
[4]Knoop J, Dekker J, van der Leeden M, Knee joint stabilization therapy in patients with osteoarthritis of the knee: a randomized, controlled trial. Osteoarthritis Cartilage. 2013 Aug;21(8):1025-34.
[5]Hafez AR, Al-Johani AH, Zakaria AR, Al-Ahaideb A, Buragadda S, Melam GR, et al. Treatment of knee osteoarthritis in relation to hamstring and quadriceps strength. J Phys Ther Sci. 2013 Nov;25(11):1401-5.
[6]Furu M,Quadriceps strength affects patient satisfaction after total knee arthroplasty. J Orthop Sci. 2016 Jan;21(1):38-43.
[7]Motlagh FN, Rostami M, Emrani A, Yazdi H, Keyhani M. Ankle rotation changes and its influences in knee osteoarthritis. Med J Islam Repub Iran. 2013 May;27(2):67-76.
[8]Lynn SK, Costigan PA. Changes in the medial-lateral hamstring activation ratio with foot rotation during lower limb exercise. J Electromyogr Kinesiol. 2009 Jun;19(3):e197-205.
[9]Hubley-Kozey C, Deluzio K, Dunbar M. Muscle co-activation patterns during walking in those with severe knee osteoarthritis. Clin Biomech (Bristol, Avon). 2008 Jan;23(1):71-80.
[10]Tuntland H, Kjeken I, Nordheim LV, Falzon L, Jamtvedt G, Hagen KB. Assistive technology for rheumatoid arthritis. Cochrane Database Syst Rev. 2009 Oct 7;2009(4):CD006729.
[11]Bautch JC, Malone DG, Vailas AC. Effects of exercise on knee joints with osteoarthritis: A pilot study of biologic markers. Ar- thritis Care Res 1997; 10:48–55.
[12]Bo ?rjesson M, Robertson E, Weidenhielm L, Mattson E, Ols- son E. Physiotherapy in knee osteoarthrosis: Effect on pain and walking. Physiother Res Int 1996;1:89–97.
[13]Callaghan MJ, Oldham JA, Hunt J. An evaluation of exercise re- gimes for patients with osteoarthritis. Clin Rehabil 1995;9:213– 8.
[14]Ettinger WH, Burns R, Messier SP, Applegate W, Rejeski WJ, Morgan T, et al. A randomized trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis. JAMA 1997; 277:25–31.
[15]Puett DW, Griffin MR. Published trials of non-medical and non- invasive therapies for hip and knee osteoarthritis. Ann Intern Med 1994;121:133–40.
[16]Fransen M, McConnell S, Harmer AR, Van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med. 2015 Dec;49(24):1554-7.
[17]Bliddal H, Leeds AR, Christensen R. Osteoarthritis, obesity and weight loss: evidence, hypotheses and horizons - a scoping review. Obes Rev. 2014 Jul;15(7):578-86.
[18]Hulme J, Robinson V, DeBie R, Wells G, Judd M, Tugwell P. Electromagnetic fields for the treatment of osteoarthritis. Cochrane Database Syst Rev. 2002;(1):CD003523.
[19]Cherian JJ, Harrison PE, Benjamin SA, Bhave A, Harwin SF, Mont MA. Do the Effects of Transcutaneous Electrical Nerve Stimulation on Knee Osteoarthritis Pain and Function Last? J Knee Surg. 2016 Aug;29(6):497-501.
[20]Verhagen A, Bierma-Zeinstra S, Lambeck J, Cardoso JR, de Bie R, Boers M, de Vet HC. Balneotherapy for osteoarthritis. A cochrane review. J Rheumatol. 2008 Jun;35(6):1118-23.
[21]Brosseau L, Yonge KA, Robinson V, Marchand S, Judd M, Wells G, Tugwell P. Thermotherapy for treatment of osteoarthritis. Cochrane Database Syst Rev. 2003;2003(4):CD004522.
[22]Stausholm, Efficacy of low-level laser therapy on pain and disability in knee osteoarthritis: Systematic review and meta-analysis of randomised placebo-controlled trials. BMJ Open. 9. e031142. 10.1136/bmjopen-2019-031142.
[23]Marks R, Allegrante JP. Effectiveness of psychoeducational interventions in osteoarthritis. 2002.
[24]Brouwer RW, Jakma TS, Verhagen AP, Verhaar JA, Bierma-Zeinstra SM. Braces and orthoses for treating osteoarthritis of the knee. Cochrane Database Syst Rev. 2005 Jan 25;(1):CD004020.
[25]Fransen M, McConnell S, Harmer AR, Van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee. Cochrane Database Syst Rev. 2015 Jan 9;1:CD004376.
[26]Bliddal H, Leeds AR, Christensen R. Osteoarthritis, obesity and weight loss: evidence, hypotheses and horizons - a scoping review. Obes Rev. 2014 Jul;15(7):578-86.
[27]Vandana J. Rathod Jagatheesan Alagesan, Parthipan Ramasamy. EFFECT OF SUPERVISED EXERCISE PROGRAM AND HOME BASED EXERCISE PROGRAM IN
OSTEOARTHRITIS OF KNEE JOINT International Journal of Current Research and Review. Vol 03 Issue 01, January, 18-27
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





