IJCRR - 13(16), August, 2021
Pages: 94-98
Date of Publication: 30-Aug-2021
Print Article
Download XML Download PDF
Comparative Study on Maternal and Child Health Services Utilization among Rural Women of Varanasi and Jaunpur
Author: Dubey AK, Singh R.
Category: Healthcare
Abstract:Introduction: Maternal and child health facilities are the leading significances of community health programs. According to In Indian culture, the mother is the underpinning of the family and children are upcoming of the country. According to WHO maternal and child health services can be defined as \"promoting, preventing, therapeutic or rehabilitation facility or care for the mother and child.\" Aim: This study is to assess the utilization of antenatal care services in two divisions of Uttar Pradesh Varanasi (Chitaipur) Jaunpur (Rehati). Methodology: Cross-sectional study, sampling technique- simple random sampling using interview schedule questionnaire. Chitaipur, Rehati, statistical test i.e., Z test is used for the comparison between two districts of Uttar Pradesh. Result: This study indicates that between two districts of village i.e. Chitaipur, Rehati. Chitaipur is a better utilization of ANC care Comparison than Rehati. Conclusion: Uttar Pradesh has hugely proceeded in terms of maternal health in recent times, motionless some key areas require prompt attention. Spreading of information and assistance regarding the utilization of ANC services should be stimulated to achieve a reduction in maternal mortality.
Keywords: Antenatal checkup (ANC), Utilization, Married women, Pregnant women, Comparative, Maternal Health Services
Full Text:
Introduction: “Women’s health issues from Womb to tomb.’’ Maternity is the most important position a women can have in her life but can be a life frightening event as well. Complications of pregnancy and child birth are major cause of death and disability among of reproductive age leading to high maternal mortality in India. During pregnancy any women can develop serious complications that require medical care. In the International Statistical classification of diseases and related health problems. Tenth revision, 1992(ICD-10), WHO defines maternal death as “The death of women while pregnant or within 42 days of termination of pregnancy, regardless of the duration site of the pregnancy or its management but not from accidental or incidental cause .1
For all women who dies, 30-50 women suffer from injury, infection, or disease. Pregnancy-related complications are among the leading causes of death and disability for women aged 15-49 in developing countries. The desired outcome of pregnancy is always a healthy mother and healthy baby. Because there is no reliable way to predict which women will develop pregnancy complications is essential that all pregnant women have access to high quality obstetric care throughout their pregnancies. Maternal complication and poor perinatal outcome are highly associated with non-utilization of antenatal and distribution care services and poor socioeconomic conditions of the patients. Poorer results are seen in undid than booked patients.2
In low and middle – Income countries, less than half of all pregnant women have a minimum of four antenatal care visit .3
In India, the reproductive and child health programme aims at providing at least three antenatal checkup which should include a weight and blood pressure check, abdominal examination against tetanus and iron and folic acid prophylaxis, as well as anemia management.4
The National maternity benefit scheme has been modified Janani Suraksha yojana (JSY). It was launched on 12th April 2005. It is a 100 percent centrally sponsored scheme under national rural health mission. The scheme focuses on poor pregnant women with special attention. Tracking each beneficiary each beneficiary registered under this yojana should have a Janani Suraksha Yojana (JSY) card along with a Maternal and child health (MCH) card. Accredited Social Health Activist, Anganwadi worker ASHA /AWW any other identified link worker under the overall supervision of the Auxiliary Nurse Midwife, Medical Officer, Primary Health Centre ANM and MO, PHC should mandatary prepare a micro -plan. This will effectively help in monitoring antenatal checkup, and standing delivery care. Uttar Pradesh is a low performing state under Janani Suraksha yojana.5
Hence, it becomes essential to analyze and study the utilization of maternal health services in Uttar Pradesh and identified districts with poor performance. This will provide track to the policy makers and Government to effectively employ its programmes under Janani Shishu Suraksha Karyakram (JSSK).
The present study focuses on developing indicators to measure the adequacy of antenatal care. In particular, this study aims to describe the adequacy of antenatal care for women in the context of a population in two different districts of Uttar Pradesh;( Varanasi) chitaipur and (Jaunpur) Rehati.
Objectives -To compare the data on maternal and child health care services two district wise Varanasi and Jaunpur in rural areas.
2- To compare the maternal and child health utilization among two districts of village chitaipur in (Varanasi), Rehati in (Jaunpur) in rural areas.
Methodology: A cross sectional study, Random sampling techniques, population – The total population 1343 (rural Chitaipur) Varanasi and 1143 (rural Rehati) Jaunpur among married women (15-49) maternal health utilization I selected randomly 60 married women in (Varanasi) chitaipur village ,60 married women in (Jaunpur) Rehati total married women in 120 selected during 15 January 2019 to 18 March 2019.
Tools: Interview Schedule questionnaire.
Statistical Analysis: The z-test for two population proportion has been applied to compare various study indicators. The hypothesis is given by:
Ho: There is no difference in study variable in the two regions.
H1: There is significant difference in study variable in the two regions.
The test statistic is given by:
Where, p1= proportion of first population
p2=proportion of second population
n1= sample size of first population
n2= sample size of second population and
The corresponding P value is calculated and if p>0.01, Ho is accepted otherwise rejected at 1% level of significance.
Result- Figure-1 describes that almost 11.6% are graduate in Varanasi (Chitaipur) compared to Jaunpur (Rehati) 50% of rural subjects were illiterate. Varanasi is better educational level compared than Jaunpur. Incidence of early marriage (below 18 years) was high in Jaunpur in rural area. In this study majority of subjects were. In this study, majority of Subject were age group 20-24 years, that is, 50% in Jaunpur compared than Varanasi 33.3%in rural area. In the study participants 61.66 were housewives and only 23.33 % did the job tailoring at home. Comparatively, In Varanasi 57.67% were housewives and only 16.63% did the job of ornament making at home. In the present study in Varanasi 93.3% Hindu, 6.7% Muslim. Comparatively in Jaunpur 68.3% Hindu, 31.7% Muslim women. In the present study in Varanasi (Chitaipur) 83.3% joint family, 16.7% Nuclear family. Comparatively in Jaunpur (Rehati)81% of joint family ,18.3% Nuclear family.

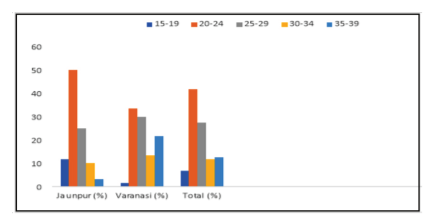
Figure-2 shows that the percentage of mothers who did not get registration within twelve weeks of pregnancy is higher in Varanasi (65%) than Jaunpur (42.5%) which is statistically significant at 1% level of significance. p-value for the indicator is 0.0082 which is less than 0.01 thus the difference between Varanasi(chitaipur) and Jaunpur (Rehati) is statistically at 1% level of significance.
Shows that the percentage of Mothers who got registered with Auxiliary nurse midwife, commonly known as (ANM) with in twelve weeks of pregnancy is higher in Varanasi (60%) then Jaunpur (30%) which is statistically significant at a 1% level of significance. P value for the indicator is 0.0005 which is less than 0.01 thus the difference between Varanasi(chitaipur) and Jaunpur (Rehati) is statistically at 1% level of significance.

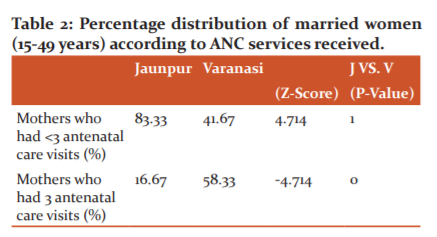
Shows that percentage of mother who had three antenatal care visits in pregnancy is higher in (Varanasi) Chitaipur (58.33%) than (Jaunpur) Rehati (16.67%) which is statistically significant at 1% level of significance p value for the indicator is 0 which less than 0.01% thus the difference between (Varanasi) Chitaipur and Jaunpur (Rehati) is statistically significant at 1% level of significance.
shows that percentage of mother who consumed iron and folic acid for 100 days when they were pregnant is higher in Varanasi (Chitaipur) (53.33%) than Jaunpur (Rehati) 23.33 which is statistically significant at 1% level of significance p value for the indicator is 0.0004 which less than 0.01thus the difference between Varanasi (Chitaipur) and Jaunpur (Rehati) is statistically at 1% level of significance.

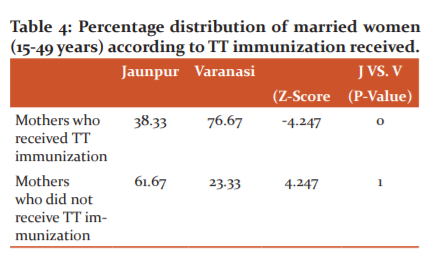
shows that percentage of mother who received Tetanus toxoid (TT) immunization in pregnancy is higher in Varanasi (Chitaipur) (76.67%) than Jaunpur (Rehati) (38.33 %) which is statistically significant at 1 % level of significance p value for the indicator 0 which less than 0.01 thus the difference between Varanasi (Chitaipur) and Jaunpur (Rehati) statistically significant at 1% level of significance.
Discussion: The results indicates that there were significant differences in utilization of maternal health care services between the two districts of Uttar Pradesh Varanasi (Chitaipur), and Jaunpur (Rehati). Overall Varanasi is better utilization of maternal and child health care services. Comparison then other similar study of Uttarakhand, Almora, Champawat, Nainital and Udham Singh Nagar had better usage of maternal health care facilities.6 Shows that the percentage of mothers who did not get registration within 12 weeks of pregnancy is higher in Varanasi (Chitaipur), 65% then Jaunpur (Rehati), 42.5% which is statistically significant at 1% level of significance p value for the indicator is 0.0082 which less than 0.01 thus the difference between Varanasi (Chitaipur) and Jaunpur (Rehati) is statistically significant at 1 % level of significance. The similar study, A greater percentage (85%) of women were registered early, according to a study in Rajasthan (Ramakant Sharma, 2006-07.6 Mother who had antenatal visit in pregnancy is higher in Varanasi (Chitaipur)58.33% than the percentage of women who went for three or more than three ANC checkups was also reported to be high in West Bengal, Assam and Orissa i.e., 97.8%,89.6% and 83% i.e., 83%,97.8% and 89.6% respectively and comparatively low in U.P, M.P and Rajasthan i.e72.8%,65.5% and 65.4% respectively (MOHFW,2007). According to NFHS-3, almost half the women (52%) received three or more antenatal checkups across India. As compared to our country E. Materia et al. (Ethiopia,1993) reported that a greater proportion (61%) of the women received antenatal care reported having had 3 or more visits according to a study regarding MCH service utilization.8 In the present study, only 53.33 % women consumed hundred IFA tablets in Varanasi (Chitaipur) than Jaunpur (Rehati 23.33%. A smaller proportion of women in our Nation. Similar study consumed hundred IFA tablets as per NFHS-III data i.e., 26% and 23% respectively. The percentage of women who consumed hundred IFA tablets was found to be very high i.e., 98% in Kerala (Sumitra, 2006).9 In the present study, Mother who had received in Varanasi (Chitaipur) 76.67% TT vaccination is higher than Jaunpur (Rehati) 38.33%. Mothers whose last birth was protected against neonatal tetanus 93.2% in Varanasi comparison than Jaunpur 90.9%. Varanasi is better than Jaunpur utilization of maternal and child health care. (NFHS4).10 In the present study Mother who had received financial assistance under Janani sukkahs yojana (JSY) for birth delivered in an institution 76.67% in Jaunpur (Rehati) comparison than Varanasi (Chitaipur) 46.67%. The Similar study According to (NFHS-4 2015-16) Mother who received financial assistance under (JSY) for birth delivered in an institution 56.3% in Varanasi in rural area 53.7% in Jaunpur in rural area.11 In this study, good awareness level is identified about the facilities provided by the scheme Mamoni as compared to other schemes. In other part of India different studies are conducted to asses the level of awareness regarding Maternal and child health care schemes. According to study by Kannan et.al awareness level about JSY is about 62.3%.12 Overall, ASHA/ ANM is very important role for pregnant women in village level.
Conclusion: Utilization of maternal and child health care MCH services was poor in both rural area in Jaunpur (Rehati), Varanasi (Chitaipur). Awareness of women concerning her health assumes special implication in the Indian context because the maternal health problems are mainly due to ignorance, poverty, and lack of knowledge regarding the issue. It is therefore very important to first focus on services for the increasing awareness level of the mother. A special attention in rural area of Jaunpur. A sustained and attentive information education and communication campaign to improve the awareness amongst community on MCH will help in improving the quality, accessibility, and utilization of maternal health care services provided by the government agencies in both rural areas. Maternal women are belonging to vulnerable group because every people are able to be easily physically, emotionally or mentally hurt or influenced in the society. But communication is a good platform to aware the pregnant women in our health. In rural area so many modes of communication to aware the health-related information for pregnant women. So, there is need of effective communication strategy to improve the quality of life of pregnant women.
Acknowledgement: We acknowledge the respondent Village level Medical staff Asha, ANM, and Dr Alok Kumar Pandey (Assistant professor in IRDC, BHU) for the total support and necessary permission Required for the article.
Conflict of Interest: Nil
Funding: Self finance Study no second party funding involved. The authors alone are responsible for the writing of this article.
References:
1-Alkema L, Chou D, Hogan D, Zhang S, Moller A-B, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. Lancet. 2016;387(10017):462–74.
2-Owolabi AT, Fatusi AO, Kuti O, Adeyemi A, Faturoti SO, Obiajuwa PO. Maternal complications and perinatal outcomes in booked and unbooked Nigerian mothers. Singapore Med J. 2008;49(7):526–31.
3-Multimedia [Internet]. Who.int. [cited 2021 Mar 19]. Available from: http://www.who.int/media
4-Özlü F, Erdem S, Göçen U, Demir F, Atalay A, Akçal? M, et al. What are the non-cardiac prognostic factors affecting mortality in neonates with aortopulmonary shunt J Matern Fetal Neonatal Med. 2021;34(3):416–21.
5-Kumar P, Chauhan S, Patel R, Srivastava S, Bansod DW. Prevalence and factors associated with triple burden of malnutrition among mother-child pairs in India: a study based on National Family Health Survey 2015-16. BMC Public Health. 2021;21(1):391.
6-Nic.in. [cited 2021 Mar 19]. Available from: https://jalan.nic.in/scheme/janani-surksha
7-Sharma R. Janani Suraksha Yojana: a study of the implementation status in selected districts of Rajasthan. 2007.
8-Kalam MA, Sharma SK, Ghosh S, Roy S. Change in the prevalence and determinants of consanguineous marriages in India between National Family and Health Surveys of 1992-1993 and 2015-2016. Hum Biol. 2021;92(2):93–113.
9-Materia E, Mehari W, Mele A, Rosmini F, Stazi MA, Damen HM, et al. A community survey on maternal and child health services utilization in rural Ethiopia. Eur J Epidemiol. 1993;9(5):511–6.
10-Sumitra S, Awasthi S, Sandeep S, Shobha P, Johnson AJ, Ls V. Maternal and child health services utilization in married women of age 15-45 years. J Commun Dis. 2006; 38:102–5.
11-Dhirar N, Dudeja S, Khandekar J, Bachani D. Childhood morbidity and mortality in India — analysis of national family health survey 4 (NFHS-4) findings. Indian Pediatr. 2018;55(4):335–8.
12-A study on awareness of maternal and child health care schemes under national health mission in Majuli, Assam. Int J Curr Res Rev [Internet]. 2017; Available from: http://dx.doi.org/10.7324/ijcrr.2017.9161
Total number of pages – 11
Total number of figure - 2
Total number of tables - 4
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





