IJCRR - 13(15), August, 2021
Pages: 158-160
Date of Publication: 10-Aug-2021
Print Article
Download XML Download PDF
Aesthetic Rehabilitation of Ellis Class II Fracture Using the Templatetechnique: A Case Report
Author: Sanjana Soneta, Shweta Kajjari, Shivayogi M. Hugar, Chaitanya Uppin, Priya Meharwade, Pooja Malavalli
Category: Healthcare
Abstract:Introduction: Coronal fracture in permanent dentition is the most common type of dental injury in children. It creates a serious social and psychological barrier for both the child and the parent. The clinician should take into consideration aspects of esthetics and should extract the exact treatment plan. Case Report: A 10-year-old boy reported to the outpatient Department of Paediatric and Preventive Dentistry, KLE VKIDS, Beagave, Karnataka, India for the treatment of a fractured upper front tooth with aesthetic concern. Intra-orally a clinical try-in of the template was done to ensure adequate fit. After appropriate shade selection of the composite material, this crown former was used to restore the fractured tooth with minimal post-restoration finishing and polishing. Conclusion: This case report describes an aesthetic rehabilitation of fractured anterior teeth using the template technique.
Keywords: Children, Composite, Esthetics, Rehabilitation, Trauma, Template technique
Full Text:
INTRODUCTION
The second most common cause of tooth loss is orofacial trauma, it has a significant negative effect on a patient’s appearance, mastication and speech. A majority of these fractures involves the maxillary central incisors, with boys outnumbering girls almost two to one.1,2 The well-known risk factors are falls, automobile/bicycle accidents, collisions, gender and age, some behavioral characteristics, physical and sporting activity. The worldwide prevalence of traumatic dental injuries ranges between 6%-37%. Seasonal variations in the prevalence of trauma have also been reported .3
Dental trauma of the incisors and their supporting tissues, which is one of the most challenging dental emergencies, requires immediate assessment and management due to psychological and physical reasons. Treatment for trauma in young permanent teeth is crucial because of its continuing development to minimize undesired complications. The treatment of dental trauma is sometimes neglected, although it might lead to pain, difficulty in articulation and mastication as well as having considerable negative effects on the patient’s self-esteem. However, aesthetics of the anterior teeth are very important aspects of human appearance and could be affected by many factors including the presence of fillings, tooth colour, position, alignment, shape and number.3
Trauma to the anterior teeth requires proper functional and aesthetic repair.4 A complete understanding of the desire of the patient is critical for success. The treatment of a fractured tooth with the help of crown and bridge requires high financial expenses, more time consuming, needs multiple sitting and is a less conservative approach. The initial treatment option should be always the most conservative one that will achieve all the desired objectives of both the patient as well as the dentist. The treatment plan advocated in this report is the Putty index restoration technique which is minimally invasive, economical and successful in repairing the fractured teeth with excellent longevity in carefully selected cases and with superior matching ability.5,6,7 In the present article, an esthetic rehabilitation of fractured anterior teeth restored with putty index composite restoration is presented.
CASE REPORT
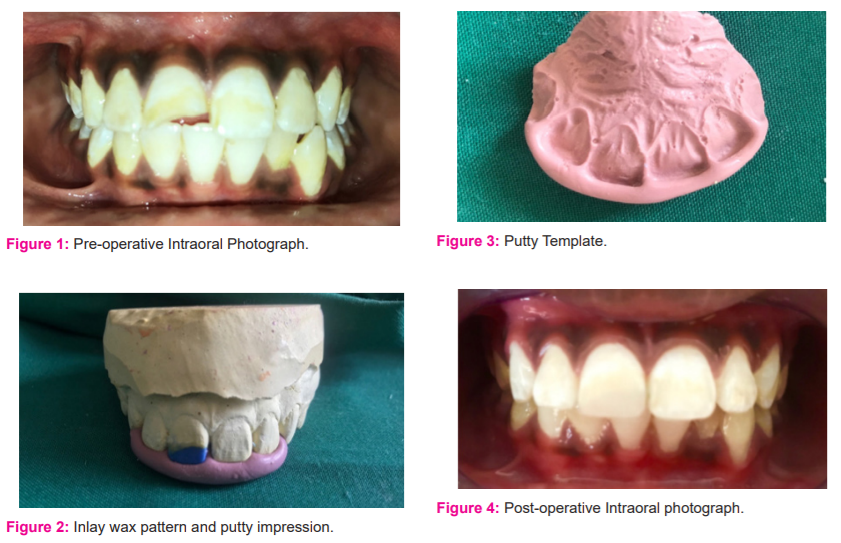
A 10-year-old boy reported to the outpatient Department of Paediatric and Preventive Dentistry, KLE VKIDS, Belagavi, Karnataka, India for the treatment of a fractured upper front tooth with aesthetic concern. A patient gave a history of trauma three months back due to hit by a pole while playing. Clinical examination revealed Ellis class II (uncomplicated) fracture irt 11 (Figure 1). The tooth was asymptomatic without any associated soft or hard tissue injuries to the supporting tissues and responded to Electric Pulp Test and Cold test. Intraoral periapical radiograph of 11 reveals the absence of pulpal or periapical pathosis. So, it was planned to restore the fractured segment with direct composite restoration using the template technique. Oral prophylaxis of the teeth was done to remove calculus and stains. A rubber dam isolation was achieved and a 45° level was given to remove the unsupported enamel and to increase the surface area of the tooth. A preliminary impression of the upper and lower arches was made using fast setting alginate and diagnostic dental stone study models were prepared. On the prepared cast, the crown build-up was done using inlay wax mimicking its natural anatomy and further, it was checked for any occlusal discrepancy. The tooth was duplicated by using Polyvinyl siloxane putty impression material, in the labial aspect the impressions were taken up to the incisal third and a template was obtained (Figure 2 and 3). Intra-orally a clinical try-in of the template was done to ensure adequate fit. After appropriate shade selection of the composite material, this crown former was used to restore the fractured tooth with minimal post-restoration finishing and polishing. (Figure 4)
DISCUSSION
Fracture of a permanent incisor is a traumatizing experience for a young patient and creates a psychological and social impact on both the parents and in children that make him target by other children. Management of patient’s with anterior tooth fracture provides a great challenge to the clinicians both from a functional and an esthetic perceptive. Treatment objectives may vary depending on the age, socio-economic status of the patient and intraoral status at the time of treatment planning.
There are various treatment options available for restoration of fractured teeth like composite restoration, fixed prosthesis, reattachment of the fracture fragment (if available)followed by post and core supported restorations.8,9 Well known treatment options such as laminated veneers or full-coverage restoration may be considered after multiple fragments rebonding/composite resin restorations have been done and this option is no longer functional. They also tend to sacrifice the healthy tooth structure and challenges the clinician to match with the adjacent unrestored teeth.10
In the present case, Considering the age of the patient where the fractured tooth is in its active eruption phase, anaesthetic direct composite restoration was planned. Various techniques were
considered to restore the tooth with the composite restoration which includes direct technique; freehand composite restorations; indirect technique; usage of preformed crowns/ thermoplastic moulds as templates. The usage of preformed crowns/thermoformed templates gave good results, but there are certain drawbacks like requirement of specialized instruments like vacuum former, availability, time-consuming and most importantly proper incremental layering of the composite material is not possible thus in the present case a novel method which includes both direct and indirect method of restoring was designed by using Polyvinyl Siloxane (PVS) Rubber base impression material (putty) as a template. This method is simple, quick and economical when compared to other invasive procedures.
The usage of the PVS template allows incremental layering of the composite material; optimal depth of cure; accurate reproducibility of the anatomic contours and minimal polishing and finishing procedures.10,11 The patient was reviewed after one week for any minimal adjustments to the restoration.
CONCLUSION
Wise use of skills, knowledge of the materials and methods should be done to achieve desired aesthetics in the patients. Esthetic Restoration of a fractured tooth is a complex procedure; this technique can prove as a simple, effective and appropriate technologies that will fulfil all the requirements of both the patient and the dentist.
Conflict of Interest: Nil
Source of Funding: Nil
Acknowledgement:
The authors are thankful to the Department of Pediatric and Preventive Dentistry, KLE VKIDS, KLE Academy of Higher Education and Research, Belagavi for the support and also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Authors’ Contribution:
1. Dr Sanjana Soneta: Designing of Manuscript
2.Dr Shweta Kajjari: Manuscript editing and plagiarism check
3.Dr Shivayogi M. Hugar: Discussion of Treatment Plan
4.Dr Chaitanya Uppin: Manuscript proofing
5.Dr Priya Meharwade: Manuscript Reframing
6.Dr Pooja L. Malavalli: Manuscript Grammar check
References:
1Andreasen JO, Ravn JJ.Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population sample. Int J Oral Surg. 1972;1(5):235-9.
2. Martens LC, Beyls HM, de Craene LG, D’Hauwers RF. Reattachment of the original fragment after vertical crown fracture of a permanent central incisor. J Pedod. 1988;13(1):53-62.
3. Azzaldeen A, Mai A, Muhamad AH, Fractured Anterior tooth using direct composite restoration: A case report. IOSR-JDMS. 2017; 16(10):61-65.
4. Baratieri LN, Monteiro S Jr, Andrada MAC. Esthetics: direct adhesive restorations on fractured anterior teeth. Chicago: Quintessence Books. 1998:3–32.
5. Chan DCN, Cooley RL. Direct Anterior Restorations. In: Schwartz RS, Summitt JB, Robbins JW, editors. Fundamentals of operative dentistry. A contemporary approach. Illinois: Quintessence Publishing; 1996:187–205.
6. Abu-Hussein Muhamad, Abdulgani Azzaldeen, Abdulgani Mai3; Step-by-Step Approaches for Anterior Direct Restorative. Int J Dent Health Sci. 2015; 2(6): 1305-1310.
7. Abu-Hussein M., Watted N., Abdulgani A; Esthetics, biological and restorative consideration in coronal segment reattachment for fractured teeth. Int J Dent Health Sci. 2015; 2(4): 998-1004.
8. Samadi F, Jaiswal JN, Pandey S, Bansal N. Restoration of fractured anterior teeth by using thermoformed templates-A Case Report. J Clin Diagn Res. 2012; 1(2): 25-8.
9. TerryDA. Adhesive reattachment of a tooth fragment: The biological restoration. Pract Proced Aesthet Dent. 2003; 15(5): 403-09.
10.K Rajavardhan, Sankar AJ, Shaik TA, V Naveen K, K Rajkumar. A novel technique in restoring fractured anterior teeth. J Clin Diagn Res. 2014 Feb;8(2):244-5.
11. Pahuja H, Mittal GK, Agarwal S, Verma A, Tomar H. Restoring esthetics in fractured anterior teeth- Template technique. Int J Cont Med Res. 2016; 3(5): 1283-84.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





