IJCRR - 13(15), August, 2021
Pages: 100-105
Date of Publication: 10-Aug-2021
Print Article
Download XML Download PDF
Risk of Developing Knee Medial Compartment Osteoarthritis in Subjects with Piriformis Tightness
Author: M Jinil, Mohanty P, Pattnaik M
Category: Healthcare
Abstract:Introduction: This study was conducted to examine the association between knee osteoarthritis and hindfoot angle, medial tibiofemoral angle, piriformis tightness and hip internal rotation. Aims: To examine the association between knee osteoarthritis and hindfoot angle, medial tibiofemoral angle, piriformis tightness and hip internal rotation. Methodology: A quantitative study with a non-experimental relational design was conducted on a total sample consist of 132 knees of 89 subjects ( 31 males and 58 females) age range (45\? 70). Result: On multiple regressions with entering model (R=.708, R2= .501 and p=.000), a good (R=.655) and significant correlation (p.000) lead to linear regression analysis between medial tibiofemoral angle and hindfoot angle. Pearson correlation between hindfoot angle and medial tibiofemoral angle was R=.655, R2 =.429, p=.001, beta= -.822. Pearson chi-square (p=.000), likelihood ratio (p=.000) and Fisher's exact test (p=.000) show that there is a significant association between piriformis tightness and OA grade, phi coefficient was .595 and Cramer's V was .343 which shows the association is strong. Conclusion: Medial compartment osteoarthritis of the knee joint is characterised by genu varum. It is often associated with hindfoot varus. Both genu varum and hindfoot varum can biomechanically be linked with the tightness of the piriformis muscle.
Keywords: Knee osteoarthritis, Piriformis, Genu varum, Hindfoot varus, Hip internal rotation, Tibiofemoral angle, Grades of osteoarthritis
Full Text:
INTRODUCTION
Osteoarthritis is characterized by progressive degeneration of articular cartilage and subchondral bone that involves the weight-bearing joint with the knee being more prevalent. There develop synoptic to clean the necrosed cartilage. Osteoarthritis poses a significant personal and global economic burden.1 The pathogenesis of OA is characterized by the destruction of cartilage and subchondral bone and by synovial inflammation.1 Osteoarthritis typically presents in the weight-bearing joints of the lower limb, with knee osteoarthritis being the most prevalent.1Pain and difficulty in ADL are the main symptoms in patients with OA.2 The medial compartment of the knee is the most commonly affected. 3 Varus malalignment is seen most commonly in knee OA.4The femoral and tibial longitudinal axes normally form an angle medially at the knee joint of 180° to 185°. If the medial tibiofemoral angle is greater than 185°, an abnormal condition called genu valgum (“knock knees”) exists. If the medial tibiofemoral angle is 175° or less, the resulting abnormality is called genu varum (“bow legs”) .5 Risk factors of osteoarthritis were described in various researches. These include both generalized constitutional factors (age, female sex, obesity, family history) and local adverse mechanical factors (trauma, occupational and recreational wear, malalignment, generalized laxity).4 But no studies described specifically the cause of varus knee alignment. Neutral lower limb alignment a vertical line drawn from the center of the head of the femur passes through the centre of the knee and centre of the ankle joints. In the case of Genu-varus, this line passes through the medial compartment of the tibiofemoral joint thus medial compartment is loaded more, predisposing to degeneration of articular cartilage. External rotation of the hip, both in weight-bearing and non-weight-bearing, results in genu varum and foot supination.6
The exact cause of OA is not known, however, increased loading, malalignment, altered biomechanics, nature of functional activities etc. contribute significantly to the development of degeneration. Though primarily it involves the articular cartilage, secondarily joint capsules ligaments, ligaments, muscles synovium and bone get affected.7The six “short external rotators” of the hip are the piriformis, obturator internus, gemellus superior, gemellus inferior, quadrates femoris, and obturator externus. Piriformis tightness results in external rotation of hip.8
Deformities of the hip, knee, and/or ankle all play a role in determining overall lower extremity alignment. As alignment shifts either toward varus or valgus at the knee, the hindfoot may compensate to restore neutral hip-knee-ankle coronal plane alignment.9 It is not fully understood how the foot and ankle compensate for a given varus or valgus deformity of the knee.10 So the objective of the study is to find out the association of biomechanical factors at the hip(internal rotation range, piriformis tightness) and ankle(hindfoot alignment and angle) to the genu varum and grades of knee osteoarthritis.
AIM AND OBJECTIVES
Aim of the study:
To examine the association between knee osteoarthritis and hindfoot angle, medial tibiofemoral angle, piriformis tightness and hip internal rotation
Objectives:
-
To find out the association between hip internal rotation, hindfoot angle & piriformis tightness with genu varum in subjects with knee osteoarthritis
-
To find out the association between piriformis tightness and OA grade, the relationship between genu varum and hindfoot angle, between genu varum and hip internal rotation, genu varum and piriformis tightness.
METHODOLOGY
Type of study: Quantitative study
Research design: Non-experimental relational study
Research setting: The study was conducted at the department of physiotherapy, SVNIRTAR, Olatpur, Cuttack.
Sample: A total sample consisted of 89 subjects ( 31 males and 58 females) age range (45– 70) years with Osteoarthritis
Inclusion criteria: A diagnosis of Primary osteoarthritis according to ACR criteria.Age between 45 and 70 years.
Exclusion criteria: Secondary osteoarthritis, Surgical conditions, Inflammatory arthritis, Congenital deformity
Institutional ethical clearance
Instruments:
Universal Goniometer: According to a study, a universal goniometer is moderate to excellent reliable to measure the joint range of motion.11Aluminium wire was used to measure the angle to quantify piriformis tightness.
Procedure: 132 knees (89 subjects) of both males and females (31 males and 58 females) were selected for study based on American college of rheumatology criteria to diagnose Knee Osteoarthritis. Medial tibiofemoral angle: In standing position subject’s anterior superior iliac spine(ASIS), the centre of patella and midpoint between two malleoli are marked, goniometer fulcrum placed on the centre of the patella, one arm placed towards ASIS and another arm placed towards midpoint between two malleoli and angle is noted.12
Hip internal rotation: Hip internal rotation was measured subject in the prone position with both knee flexed to 90°, hip in 0° abduction and adduction and flexion. Centre the fulcrum over the anterior aspect of the patella. Both arms of the instrument are together vertically. At the end of the hip, the internal rotation mobile arm move using the crest of the tibia and a point midway between the two malleoli for reference.13
Hindfoot angle: The first subject was brought into the measurement area by an assistant and stepped onto the measurement area. The subject was then instructed to march in place approximately 10 steps to assume a comfortable, natural position while aligning the heels with the posterior edge of the area. The midpoint between medial and lateral malleoli was determined. Goniometer fulcrum was placed on that mark. Hindfoot angle was measured as the angle between the bisectors of the calf and the calcaneus using a goniometer.14
Piriformis test: Subject in crook lying. Affected limb crossed over other limb and hip flexed to 60° and knee in flexion. Then it is adducted in an externally rotated position while the therapist keeping sound limbs in adduction to avoid pelvic rotation by the therapist’s knee. If there is pain over the piriformis muscle at the end of the range suggestive of piriformis test positive.15 Angle to quantify piriformis tightness: As mentioned above in the same position of piriformis test subject positioned close to the wall where greater trochanter of affected limb touching the mark drew on the wall. A 60° line was already marked on the wall for hip joint keeping accurately, Hip is flexed to 60° by following the line drew on the wall, hip is adducted in external rotation. The angle between wall and thigh measured using aluminium wire which will be in “V” shape. It was measured by a protractor and noted.
KneeOA grade: Kellegren Lawrence scale is used to grade OA knee from X-RAY.16
-
Grade 1: doubtful narrowing of joint space and possible osteophytic lipping.16
-
Grade 2: definite osteophytes, definite narrowing of joint space.16
-
Grade 3: moderate multiple osteophytes, definite narrowing of joints space, some sclerosis and possible deformity of bone contour.16
-
Grade 4: large osteophytes, marked narrowing of joint space, severe sclerosis and definite deformity of bone contour.16
DATA ANALYSIS
Statistical analysis was performed using SPSS version 23.0. Multiple regressions with entering model were done with medial tibiofemoral angle as the dependent variable and hip internal rotation, hindfoot angle, angle to quantify piriformis tightness as independent variables Pearson correlation was done for medial tibiofemoral angle and hindfoot angle. A good and significant correlation leads to linear regression analysis. Chi-square tests were done between piriformis tightness and OA GRADE. Symmetric measures Phi coefficient and Cramer’s V were also calculated. All variables were analyzed using a 0.05 level of significance.
RESULTS
Multiple regressions
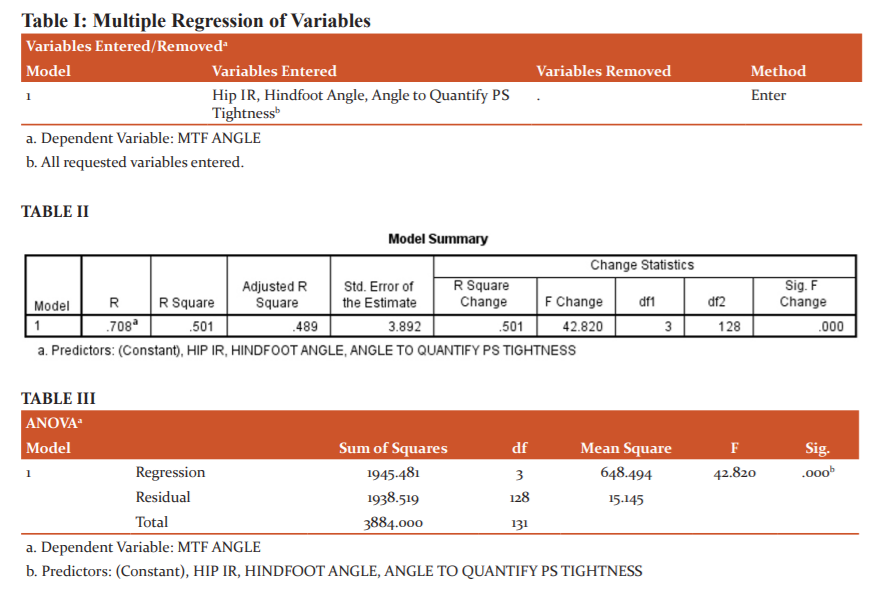
As a table, I show multiple regressions with entering model was done with medial tibiofemoral angle as the dependent variable hip internal rotation, hindfoot angle, angle to quantify piriformis tightness as independent variables. R=0.708, R2= 0.501 and p=0.000 .As R2 is 0.501 approximately half of the variation of dependent (medial tibiofemoral angle) can be explained by the independent variables (hip internal rotation, hindfoot angle, angle to quantify piriformis tightness). It may be because only hindfoot angle shows a significant relationship with medial tibiofemoral angle (p=0.000); hip internal rotation (p=0.113) and angle to quantify piriformis tightness (p=0.088) doesn’t show a significant relationship with medial tibiofemoral angle.
Relationship between hindfoot angle and medial tibiofemoral angle
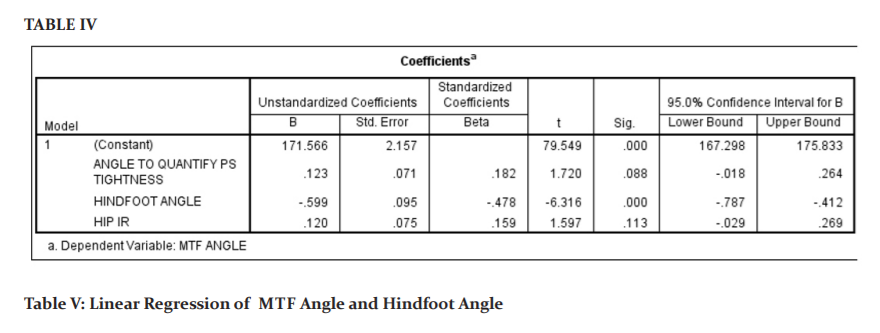
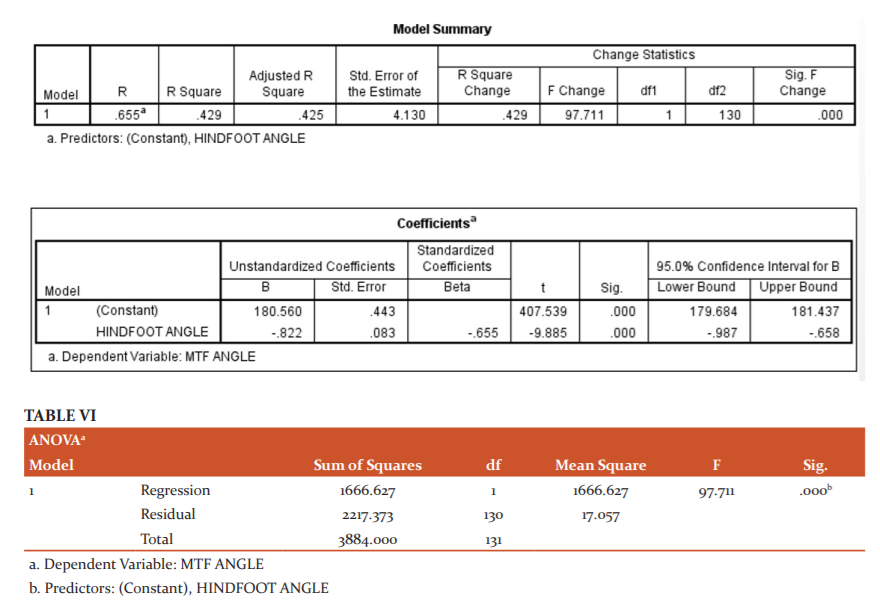
Pearson correlation was done for medial tibiofemoral angle and hindfoot angle. A good (R=0.655) and significant correlation (p=0.000) lead to linear regression analysis between medial tibiofemoral angle and hind foot angle. Pearson correlation between hindfoot angle and medial tibiofemoral angle was R=0.655, R2 =0.429, P=0.001, beta= -0.822(Table II). Linear regression with medial tibiofemoral angle as dependent variable and hindfoot angle as independent variable shows that when there is a 1° change in the hindfoot angle there are -0.822 changes in medial tibiofemoral angle.
Relationship between and piriformis tightness and osteoarthritis of the knee
Table III shows Chi-square tests were done to find an association between piriformis tightness and OA Grades. Pearson chi-square (p=0.000), likelihood ratio (p=0.000) and Fisher’s exact test (p=0.000) show that there is a significant association between piriformis tightness and OA grade. Symmetric measures were calculated to find the strength of association. Phi coefficient was 0.595 and Cramer’s V was 0.343 which shows the association is strong (Table IV).
DISCUSSION
The overall results of this study with multiple regressions with entering model showed that as r2 is 0.501 approximately half of the variation of dependent variable medial tibiofemoral angle can be explained by the independent variables angle to quantify piriformis tightness, hindfoot angle, hip internal rotation.
Medial tibiofemoral angle and hindfoot angle
In the present study, the Pearson correlation between hindfoot angle and medial tibiofemoral angle was R=0.655, R, p=0.000. Linear regression with medial tibiofemoral angle as dependent variable and hindfoot angle as independent variable shows that when there is a 1° change in the hindfoot angle there is a -0.822 change in medial tibiofemoral angle. It means that when there is a 1° increase in the hindfoot angle (varus) there will be a 0.822° decrease in the medial tibiofemoral angle (varus), which may result in genu varum.
According to Otis A-C, the motion of the hindfoot is coupled to the motion of the leg and the forefoot. Hindfoot varus is a component of supination hence supination of the subtalar joint with the foot on the ground produces lateral rotation of the tibia with inversion of the calcaneus, cuboid, and navicular. Lateral rotation of the tibia causes lateral rotation of the femur which eventually results in the shift of the mechanical axis medially which results in a decrease in the medial tibiofemoral angle. Inadequate or excessive pronation or supination may contribute to complaints of the knee, hip, and even back pathologies by interfacing with the coupling between the foot and rest of the lower extremity during weight-bearing.17
The study carried out by Chang C. B., Jeong, J. H., Chang, M. J., Yoon, C., Song, M. K., & Kang, S. B.hypothesized that most patients who undergo TKA have varus malalignment of the lower limb, which, theoretically, may exert a force that tilts the ankle joint line into varus. The ankle joint and/or hindfoot, therefore, have to compensate for the varus malalignment of the lower limb to obtain a plantigrade foot.18
Piriformis tightness and OA
In this study Pearson chi-square (p=0.000), likelihood ratio (p=0.000) and Fisher’s exact test(p=0.000) show that there is a significant association between angle to quantify piriformis tightness and OA grade. In the symmetric measures, the phi coefficient was 0.595 and Cramer’s V was 0.343 which shows the association is strong. It means that while piriformis tightness increases the severity of OA may increase.
It may be because according to Norman, T. L., Hutchison, J. D., & Gardner, M. R external rotation of the hip and knee compared to the direction of gait is a form of malalignment. External rotation may be caused by piriformis tightness. The centre of the knee joint, corresponding to the tibial fossa, is displaced laterally when the hip is in external rotation.19 In external rotation, the knee displaces from the midline at the stance phase. According to Kapandji varus or valgus deviations of the knee are harmful as they cause osteoarthritis with time, in effect, the mechanical loads are not evenly spread over the lateral and medial two compartments of the knee joint, leading to premature erosion of their respective articular surfaces and culminating in medial femorotibial osteoarthritis in the presence of genu varum or lateral femorotibial osteoarthritis in the presence of genu valgum.6
CONCLUSION
Medial compartment osteoarthritis of the knee joint is characterised by genu varum. It is often associated with hindfoot varus. Both genu varum and hindfoot varus can biomechanically be linked with the tightness of the piriformis muscle. Stretching of the piriformis may be included in the management of osteoarthritis of the knee joint.
LIMITATION
To quantify piriformis tightness an innovative method with aluminium wire was used. Inter and interrater reliability of the measurement tool was not done.
ACKNOWLEDGEMENT
The authors express their sincerest gratitude and warm appreciation to the patients who participated in this study. Authors acknowledge immense help received from the scholars whose articles are cited and included in the manuscript. The authors are grateful to all the authors/ editors/publishers of those articles, journals, and books from where the literature of this article has been reviewed and discussed.
NO CONFLICT OF INTEREST AND SOURCE OF FUNDING
References:
-
Deasy M, Leahy H, Semiciv A I. Hip Strength Deficits in People With Symptomatic Knee Osteoarthritis: A Systematic Review With Meta-analysis. J Orthop. Sports Phys. Ther; https://doi.org/10.2519/jospt.2016.6618: 2016, 46(8), 629–640.
-
R K Mahato, D Panchal, Vyas N J. Exercise interventions in Knee Osteoarthritis in Aging adults: A Systematic Review of Randomized Clinical Trials, Int J Curr Res. Rev. 2019: 11(23)
-
Vincent KR, Conrad BP, Fregly BJ, Vincent HK. The pathophysiology of osteoarthritis: a mechanical perspective on the knee joint. PM R. 2012 May;4(5 Suppl):2012,S3-9. doi: 10.1016/j.pmrj.2012.01.020. PMID: 22632700; PMCID: PMC3635670.
-
Hussain SM, Neilly DW, Baliga S, Patil S, Meek R. Knee osteoarthritis: a review of management options. Scott Med J. 2016 Feb;61(1):7-16. doi: 10.1177/0036933015619588. Epub 2016 Jun 21. PMID: 27330013.
-
Snyder-Macker L, Lewk M, Joint structure and function; a comprehensive analysis, fourth edition; 2005, 396-397
-
Kapandji AI. The kinesiology of joints; the lower limb. 2011; 2:70-71;
-
Egloff C, Hügle T, Valderrabano V. Biomechanics and pathomechanisms of osteoarthritis. Swiss Med Wkly. 2012 Jul 19;142:w13583. doi: 10.4414/smw.2012.13583. PMID: 22815119.
-
Neuman DA. Kinesiology of the musculoskeletal system: Foundation for rehabilitation,second edition, 2010: 520-523.
-
Norton J. J., Amendola, A., Ba, C. F . Correlation of Knee and Hindfoot Deformities in Advanced Knee OA?: Compensatory Hindfoot Alignment and Where It Occurs, Clin Orthop Relat Res. 2015:166–174. https://doi.org/10.1007/s11999-014-3801-9; 2015,166–174.
-
Kim, C., Gwak, H., Kim, J., Lee, C., Kim, J., Oh, M., Park, J. Radiologic Factors Affecting Ankle Pain Before and After Total Knee Arthroplasty for the Varus Osteoarthritic Knee. J Foot Ankle Surg. 2018Oct;57(5):865-869,https://doi.org/10.1053/j.jfas.2018.02.002;
-
Gogia PP, Braatz JH, Rose SJ, Norton BJ. Reliability and validity of goniometric measurements at the knee. Phys Ther. 1987 Feb;67(2):192-5. doi: 10.1093/ptj/67.2.192. PMID: 3809242.
-
Singh, O., Sharma, B., Ramphal, S. K. A Study of Tibiofemoral angle among Healthy Female Maharashtrian Population, Int J Res Med Surg. 2018; 17(5): 12–18; https://doi.org/10.9790/0853-1705021218
-
Norkin C.C. Measurement of joint motion; A guide to goniometry,fourth edition, 2011; 210-211.
-
Donatelli RA., The biomechanics of the foot and ankle. 2nd ed.Philadelphia: FA Davis; 1996;178–9
-
Mohanty PP, Pattnaik M. Effect of stretching of piriformis and iliopsoas in coccydynia, J Bodyw Mov Ther. 2017;03:024;
-
Kohn, M.D., Sassoon, A.A., Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin Orthop Relat Res. 2016;474: 1886–1893. https://doi.org/10.1007/s11999-016-4732-4
-
Oatis CA, Kinesiology; the mechanics and pathomechanics of human movement, Second edition. 2009: 808-832
-
Chang CB, Jeong JH, Chang MJ, Yoon C, Song MK, Kang SB. Concomitant Ankle Osteoarthritis Is Related to Increased Ankle Pain and a Worse Clinical Outcome Following Total Knee Arthroplasty. J Bone Joint Surg Am. 2018 May 2;100(9):735-741. doi: 10.2106/JBJS.17.00883. PMID: 29715221.
-
Norman TL, Hutchison J, Gardner MR, Knee Loading due to Varus and External Rotation in Gait Supports Medial Compartment Wear in Total Knee Arthroplasty. J Orthop Rheumatism. 2017; 1(1):8-18.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





