IJCRR - 13(14), July, 2021
Pages: 224-229
Date of Publication: 20-Jul-2021
Print Article
Download XML Download PDF
Evaluate the Effect of Tapered Canal Preparation on the Retention of Posts Cemented with Resin Cement - An in vitro Study
Author: Tarun Kumar Singh, Govind Lal Meena, Amit Chhaparwal, Manish Kumar, Prashant Jadhav, Ranjan Mani Tripathi
Category: Healthcare
Abstract:Introduction: In endodontically treated teeth with less remaining tooth structure posts are inserted to provide stability and retention for a core. The posts retention is dependent on various factors related to post like- cement post and cement dentine interaction, type of luting cement, and taper of the post. Aim: This in-vitro study aimed to evaluate the effect of endodontic taper on post retention using parallel-sided prefabricated posts luted with dual-cure resin cement. Methodology: Sixty freshly extracted human maxillary central incisors of approximately the same sizes were selected for this study. The Crown of these teeth was separated at the cementoenamel junction and divided randomly into six groups of ten teeth each. Biomechanical preparation was carried out using different tapered Ni-Ti file systems ranged as 0.02, 004, 0.06, 0.08, 0.10, and0.12 taper. Root canal obturation was done with gutta-percha using the lateral condensation method. Results: Taper 0.02 represents the taper size where a smaller average force was required to remove the post from the root canal. The average force required to remove the post from the root in taper group 0.02 was statistically different from all other taper sizes. Taper size 0.04 required highest average force to remove the post. Average force for size 0.04 was statistically different from the taper size 0.02, 0.06, 0.08, 0.10, 0.12 tapers. Conclusion: The result of the present study indicates that increasing taper of root canal adversely affect the post retention. The findings of this study indicate that instrument taper size preparation of the canal makes a difference to resistance to post dislodgement.
Keywords: Post Retention, Prefabricated Post, Polymerization shrinkage, Resin Cement, Fracture, C-Factor
Full Text:
Introduction:
Endodontics has become an increasingly routine facet of patient care in general dental practice. Success in endodontic treatment depends almost completely on how well the root canal is shaped and cleaned. Principles of root canal preparation are to remove all organic debris and microorganism from the root canal system and shape the walls of the root canal to facilitate cleaning and subsequent obturation of entire root canalsystem.1
Parallel sided posts are more retentive than tapered post and serrated or grooved posts are more retentive than smooth posts. Cement thickness is a very important factor as parallel sided post relies on even thickness of cement throughout the length of the post to overcome the inherent weaknesses of the cementing medium. With greater taper file systems root canal walls are prepared to divergent. Parallel sided post placement in a highly divergent canals lead to uneven thickness of luting cement throughout the post length. Thus highly tapered root canal preparation may have an adverse effect on postretention.2
The purpose of this study was to evaluate the effect of tapered canal preparation on the retention of posts cemented with resin cement. Retention of post in canal prepared using 0.04 to 0.12 taper instruments were compared for retention against canal preparation using the traditional 0.02 taper instrument as a positive control. Sixty human maxillary central incisors were used and divided into six groups with different tapered root canal preparation. Prefabricated parallel sided grooved posts were cemented in prepared post channels with resin cement. Retention of these posts was checked using tensile testing machine. Hypothesis was that an increase in the taper of root canal results in a lowering of post retention.
Material and Methods:
Sixty Caries free, unrestored human maxillary central incisors recently extracted for periodontal reason were used for this study. Storage, handling, and Sterilization of extracted teeth were used in this study followed the occupational safety and health administration and the Centre for the Disease Control guidelines.
Selection, preparation and storage of specimens-
All teeth were approximately of similar size and free of caries. Care was taken to select teeth to obtain 12 to 13 mm root length after crown removal at Cemento- Enamel Junction (CEJ). All teeth were free of open apices, fracture lines, resorptive areas.
Clinical crowns of teeth were removed at CEJ using high speed air- rotor hand piece and diamond taper fissure burs. Teeth were observed at cross sectional view of root canal at CEJ and selected according to the internal diameter of uninstrumented root canal so that the intracanal variation can be minimized.
Now total 60 teeth were selected and randomly divided into six groups consisted 10 teeth in each group.
Instrumentation of root canal-
After removal of the pulp tissue remnants by barbed broach, # 10 K-file was inserted into each root canal until it could be seen through the apical foramen. The working length was established by reducing this length by 0.5mm.
Group I- (Taper 0.02 Group) /control group
10 teeth in this group were prepared with hand Ni-Ti files (Dentsply/ Tulsa Dental), using RC Help (EDTA Gel) for lubrication and 2.5% NaOCl for irrigation. Teeth were instrumented using step back technique upto apical size # 30 and upto # 60 coronally according to the technique proposed by Walton.
Group II- (Taper 0.04 Group)
10 teeth in this group were prepared using 0.04 taper rotary Profile Ni- Ti files (Dentsply/ Tulsa dental)by using Crown down preparation using RC Help and 2.5% NaOCl solution. Files were used in contra angle Gear Reduction handpiece (Tecnika, Dentsply/Maillefer) and torque control motor.
Group III- (Taper 0.06 Group)
10 teeth were prepared using 0.06 taper rotary Profile Ni-Ti files (Dentsply/ Tulsa Dental), in crown down manner in gear reduction handpiece with RC Help and 2.5% NaOCl solution.
Group IV- (Taper 0.08 Group)
10 teeth were prepared using 0.08 taper rotary NRT files (Mani/Prime dental products), in crown down manner in gear reduction handpiece with RC Help and 2.5% NaOCl solution.
Group V- (Taper 0.10 Group)
10 teeth were prepared using 0.10 taper rotary NRT files (Mani/ Prime dental products), in crown down manner in gear reduction handpiece with RC Help and 2.5% NaOCl solution.
Group VI- (Taper 0.12 Group)
10 teeth were prepared using 0.12 taper rotary NRT files (Mani/ Prime dental products), in crown down manner in gear reduction handpiece with RC Help and 2.5% NaOCl solution.
All teeth were thoroughly irrigated with 10 ml of 2.5% NaOCl solution and dried with paper points.
Obturation of teeth
The root canals were dried thoroughly with appropriately sized paper points. All root canals were obturated with suitable gutta percha points and AH Plus Sealer. Sealer was mixed according to the manufacturer’s directions and applied into the root canals with lentulospiral attached to a slow speed Micromotor handpiece. Roots were left undisturbed for 48 hours for thorough setting of sealer.
Preparation of the post space
All roots were marked at 8mm downward from the CEJ to produce a constant depth of post space preparation. It allowed about 3-5 mm gutta percha seal apically after post space preparation in the root canals. Gutta percha was removed by using heated pluggers. Then post channels were prepared using Peesoreamers. Size of final Peesoreamers was selected after evaluation of prepared root canal size. After post space preparation corresponding sized EG posts (Effective Groove post) were checked inside the prepared post space for closest fit and to assure 8 mm embedment depth and passivity of fit in to the post space.
Cementation of posts-
Step I- Etching
-
37% phosphoric acid gel was applied to root canal for 30 seconds.
-
Canals were rinsed for 10 seconds with distilled water.
-
Root canals were dried with paper points.
Step II- Bonding
-
Bonding agent was applied to the canals.
-
Excess was removed with dry paper points.
-
Dried for 5 seconds.
-
Light curing was carried out for 10 seconds.
Step III- Cementation
-
3M RelyX ARC was dispensed on the mixing pad, mixed for 10 seconds and applied to root canal walls with lentulospiral.
-
A thin layer of cement was placed on the posts and posts were seated slowly in the prepared post channels and held vertically by exerting slight pressure at the post head.
-
Excess cement was removed and light curing of cement was carried out for 40 seconds from occlusal direction.
Preparation for testing-
Roots of all teeth were embedded in acrylic resin blocks, parallel to the long axis of the root. Then they were stored in saline solution until tensile testing. All the specimens of six groups were subjected to Scientific Tensile Testing Machine at the crosshead speed of 2 inch/min. the load was gradually increased and the tensile force required to initially break the cement bond and partially or totally remove the post was recorded.
Observations:
In this study, influence of tapered canal preparations on post retention was evaluated using Scientific tensile testing machine.This study was conducted in vitro using 60 extracted human maxillary central incisors. Six groups were created and ranged as 0.02, 0.04, 0.06, 0.08, 0.10, and 0.12. Each group comprises of ten teeth.
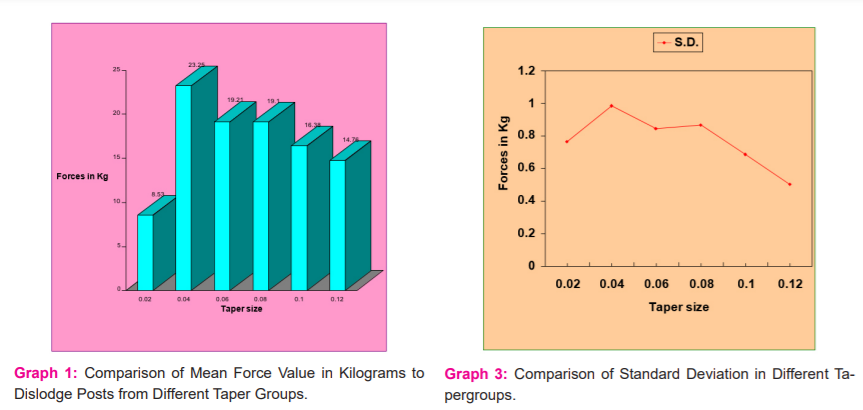
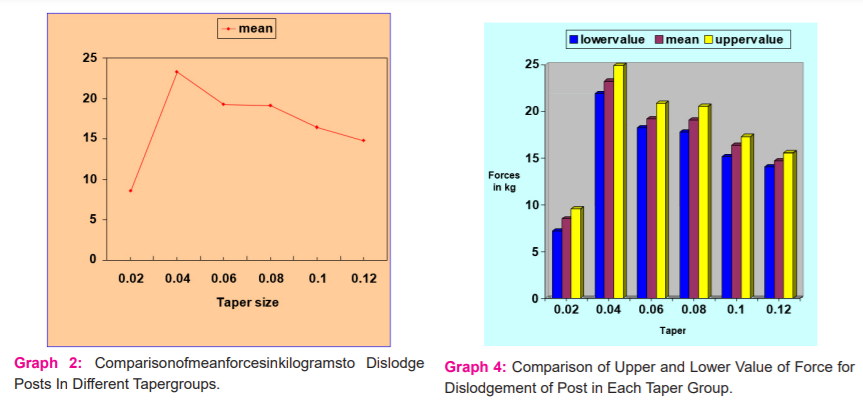
The required force to dislodge posts from the specimens were recorded in kilograms and summarized in (Table-1) (Graph1&2). Following observation was made with each experimental group-
GROUP I (Control group)/ 0.02 taper Group-
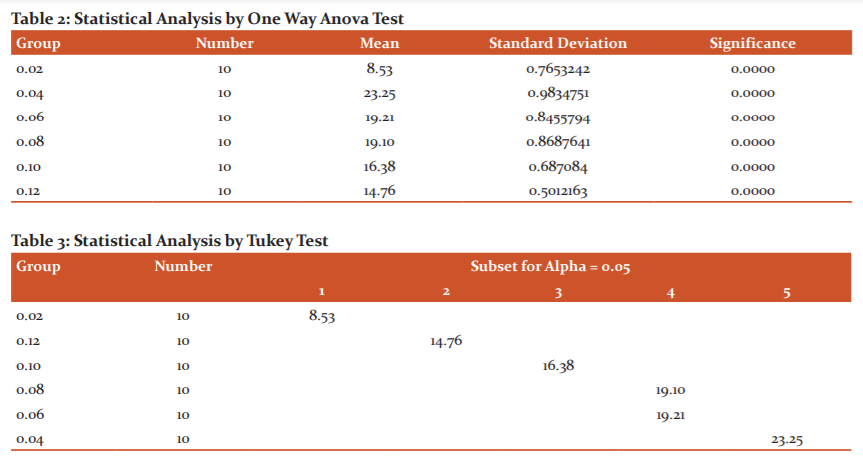
Mean force required to dislodge posts was 8.53 Kg. Minimum value of force required was 7.23 Kg and maximum value of force was 9.58 Kg.
GROUP II / 0.04 taper Group-
Mean force required to dislodge posts was 23.25 Kg. Minimum value of force required was 21.91 Kg and maximum value of force was 24.97 Kg.
GROUP III /0.06 taper Group-
Mean force required to dislodge posts was 19.21 Kg. Minimum value of force required was 18.24 Kg and maximum value of force was 20.89 Kg.
GROUP IV /0.08 Taper Group-
Mean force required to dislodge posts was 19.10 Kg. Minimum value of force required was 17.84 Kg and maximum value of force was 20.59 Kg.
GROUP V / 0.10 Taper Group-
Mean force required to dislodge posts was 16.38 Kg. Minimum value of force required was 15.18 Kg and maximum value of force was 17.33 Kg.
GROUP VI / 0.12 Taper Group-
Mean force required to dislodge posts was 14.76 Kg. Minimum value of force required was 14.07 Kg and maximum value of force was 15.59 Kg.
Dislodged posts were observed after tensile testing for failure mode. In all groups failure was noted at the resin cement-dentin interface i.e. adhesive failure. Most of the resin was adhered to the post with little remaining on root canal. No root fracture was noted in any group. Thus failure noted was due to the loosening of posts in all groups with increasing tensile forces.
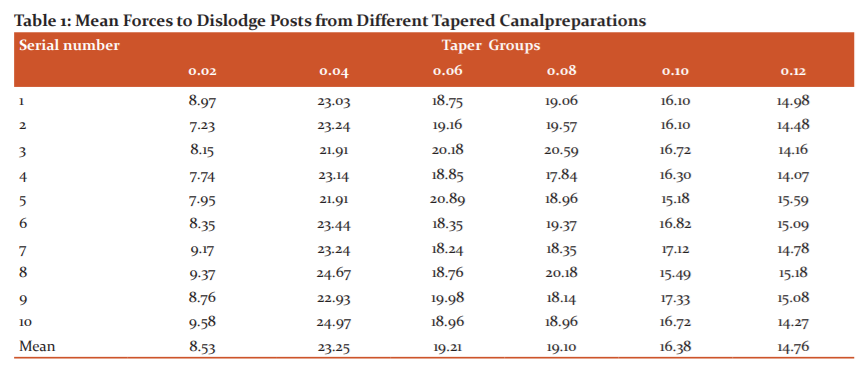
Statistical analysis-
Statistical analysis was conducted by using one-way ANOVA test. Results are summarized in table. One-way ANOVA indicated very highly significant difference between means of all groups, i.e. p = 0.0000 (p < 0.0001). (Table 2) (Graph 3)
Tukey HSD (Honestly significant test) test was conducted to find out homogeneity between groups. Only 0.06 and 0.08 taper groups were found homogenous. (Table 3) (Graph 4)
Results-
Taper 0.02 represents the taper size where smaller average force was required to remove the post from the root canal. Average force required to remove the post from the root in taper group 0.02 was statistically different from all other taper sizes.
Taper size 0.04 required highest average force to remove the post. Average force for size 0.04 was statistically different from the taper size 0.02, 0.06, 0.08, 0.10, 0.12 tapers. All taper sizes were different from each other except 0.06 and 0.08 taper sizes were found homogenous as per Tukey HSD test.
Discussion:
In this study six groups of ten teeth each were prepared with tapers of 0.02, 0.04, 0.06, 0.08, 0.10, 0.12 and parallel sided grooved posts were cemented in prepared post space with the help of dual cure resin cement.3,4,5,6 Resin based AH plus sealer is used as eugenol based sealers are reported to inhibit polymerization of the composite resin.
Depth of the post preparation was 8 mm in all teeth to produce a constant post embedment depth. Dentin smear layer produced during endodontic procedure is removed during etch and rinse process. Infiltration of exposed collagen fibrils network with resin permits the formation of resin dentin interdiffusion zone with resin tags and adhesive lateral branches, thus creating the micromechanical retention of the resin to the demineralized substrates. Post cementation was carried out using dual cure resin luting cement (Rely X ARC, 3M, ESPE). Composite material is suggested as a luting agent for endodontic posts because it allows latitude of 500µ during the adaptation of root canal.7 Advantage of dual cure cement is in areas deep inside the post space which are not accessible to light curing, thus requiring chemical cure.8,16
All specimens were subjected to tensile force using Scientific Tensile testing Machine after embedding in acrylic blocks. Increasing tensile force was applied at constant speed until post dislodgement occurs. Forces are recorded in kilograms.
All failures were noted at the cement-dentin interface which is usually noted with post luted with resin luting cement. Bonding of resin cements is mainly impaired by unfavorable root canal configuration, related to a high C- factor (cavity configuration factor), which may be up to 40 times higher compared to direct intracoronal restorations with similar cement thickness.9 The C-factor indicate the ratio between the bonded and non-bonded surface areas. It allows resin flow with consequent reduction in polymerization shrinkage stress.10,11,12 With the reduced non-bonded area inside the root canals, reduces stress is not enough and polymerization shrinkage is higher than the bond strength, give rise to the formation of voids at the cement-dentin interface.13, 14,15.
This in-vitro study has limitations as the tests were carried out in uniradicular teeth with specific dimensions and post preparations, under static tensile loading. Diverse retention values in the present study may be attributed.
- Various quantities of dentin particles in the prepared canal after cleaning and in smeared layers.
-
-
Absence of control to ensure the identical position of all posts in the channel center for uniform width of the cement layer surrounding the posts.
-
Differences in the dentin of teeth resulting from moisture content, pulpal condition at the time of extraction, age of patient, and direction of dentin tubules.
-
Inconsistent and unpredictable cementing pressure during the setting process.
-
Another factor of importance to consider is the shape of the root canal. Since root canals are seldom entirely conical, there will likely be uneven film thickness and possible voids.
Conclusion:
The result of the present study indicates that increasing taper of root canal adversely affect the post retention. The findings of this study indicate that instrument taper size preparation of the canal makes a difference to resistance to post dislodgement. Therefore it seems that the taper size is important in restoration of endodontically treated teeth. More studies are needed to see how taper preparation size affects the strength of the remaining root structure.
Acknowledgement: Authors acknowledge the enormous help received from the authors whose articles are cited and included in references to the manuscript.
Conflict of interest: Nil
Financial support: Nil
Ethical Clearance: Not required (In-Vitro study)
Patient consent: Not required (In-Vitro study)
Individual Author’s contribution: All authors have equally contributed in the writing and formatting of manuscript of this article.
References:
1. Hunter A.J, Feiglin, Williums. J. F. Effects of post placement on endodontically treated teeth. J Prosthet Dent. 3013 Aug; 62(2):166-72.
2. Buchanan LS. The standardized taper root canal preparation – Part-1. Concepts for variably tapered shaping instruments. Int Endod J. 2000 Nov; 33(6):516-29.
3. Fernandes A., Rodrigues S., Sardesai G & Mehta. Retention of endodontic post- A Review. Endodontology 2001; 13:11-18.
4. Bonfante G, Kaizer OB, Luiz Fernando Pegoraro Accácio Lins do Valle. Tensile bond strength of glass fiber posts luted with different cements. Braz Oral Res 2007;21(2):159-64.
5. Ferrari M, Vichi, Grandini, Goracci. Efficacy of a self-curing adhesive resin cement system on luting glass fiber posts into root canals: an SEM investigation. Int J Prosthodont 2001;14:543–549.
6. Purton DG, Love RM. Rigidity and retention of carbon fiber versus stainless steel root canal posts. Int. Endod. J. 1996; 29: 262-5.
7. Mark S. Hagge, Ralan D. M. Wong, James S. Lindemuth. Composite cement thickness on retention of a prefabricated dowel. J Prosthodont. 2002 Mar; 11(1):19-24.
8. Schwartz RS, Robbins JW. Post placement and restoration of endodontically treated teeth: A literature review. J Endod 2004; 30:289?301.
9. Zandbiglari T, David H, Schafer E. Influence of instrument taper on the resistance to fracture of endodontically treated roots, Oral Surg Oral Med Oral Pathol Oral Radiol, Endod 2006; 101:126-31).
10. Richard S. Schwartz, James W. Robbins- Post placement and restoration of endodontically treated teeth: A Literature Review. J Endod. 2004 May; 30(5):289-301.
11. Stegaroiu, Yamada. Retention and failure mode after cyclic loading in two post & core system. J Prosthodont. 2006 May-Jun;15(3):172-9.
12. Dominici JT, Eleazer PD, Clark SJ, Staat RH, Scheetz JP. Disinfection/ sterilization of extracted teeth for dental student use. J Dent Educ 2001; 65:1278?80.
13. Anderson GC, Perdigao J, Hodges JS, Bowles WS, Effeciency and effectiveness of fiberpost removal using three techniques. Quintessence Int. 2007; 38: 663-70.
14. Rundquist BD, Versluis A. How does canal taper affect root stresses? Int Endod J. 2006;39(4):226–237
15. Thompson SA. An overview of Nickel Titanium alloys used in dentistry. Int Endod J. 2000 Jul;33(4):297-310.
16. Ashok NG, Sangeetha S. Evaluation of post-operative complaints in fixed partial denture wearers and thoses with crowns: A questionnaire based study. Int J Cur Res Rev. 2016; 16(8):30-34.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





