IJCRR - 13(14), July, 2021
Pages: 142-147
Date of Publication: 20-Jul-2021
Print Article
Download XML Download PDF
Comparative Efficacy of Regular and Musical Toothbrush in Supragingival Plaque Removal in Children - A Randomized Clinical Trial
Author: Sarojini Ramya Pillay, Jessy P, Subhabrata Maiti
Category: Healthcare
Abstract:Background: Children routinely present with unsatisfactory oral hygiene due to a lack of interest in brushing twice daily. Motivation serves to be an integral part of health promotion to children at the learning phase of their life. Aim: The purpose of this study was to clinically evaluate and compare the efficacy of musical toothbrush over regular toothbrush in supragingival plaque removal among children of age 6-11years Materials and Methods: 42 children aged 6-11 years who fulfilled the criteria enrolled on a single-blind, randomized study. The Eligible subjects were randomly assigned into two groups by a second examiner one group used a musical toothbrush and another group used a regular toothbrush for the duration of the study. Subjects were instructed to brush their teeth at home twice daily for 2 minutes each day for the 45-day study period. At 0 day and after 15, 30 and 45days, the plaque was assessed following 24 hrs of no oral hygiene. At each visit plaque removal was evaluated using disclosing solution before and after subjects had brushed their teeth for 2 minutes under supervision. The plaque build-up was noted using the Quigley-Hein plaque index. Independent 'T'test and paired T-test was used to compare the outcome variables within and across the two groups. Results: Greater mean changes in whole mouth plaque reduction were seen for Group 2 (musical group) when compared to that of Group 1(regular group) at days 15, 30 and 45 (P< 0.05). Conclusions: The present study showed significant improvements in supragingival plaque control in the musical brushing group. The features of the musical toothbrush compared with a regular toothbrush may increase motivation and compliance, thus helping to establish the habit of regular daily brushing of the teeth.
Keywords: Children, Motivation, Musical toothbrush, Plaque Removal, Tooth brushing, Supragingival plaque
Full Text:
INTRODUCTION:
School going age is regarded as the influencing stage in a child’s life where lifelong sustainable oral health-related behaviour, belief, and attitude can be established with a long-lasting impact.1 Effective plaque control and good oral hygiene maintenance play a solid role in maintaining oral health and prevention of these diseases which can be achieved primarily by effective tooth brushing.2,3,4 Also regular removal of supragingival plaque has been shown to reduce counts of pathogenic species both supra- and sub-gingivally.5,6 Various chemical and other mechanical methods have been advocated for this purpose, but tooth brushing has been cited as the gold standard and most commonly used effective and safest therapeutic method in removing plaque.7,8,9
It is generally known that tooth brushing by young children under the age of 10 years is inefficient due to lack of motivation and poor manual dexterity at this age.10-13 It has been shown that tooth brushing practised by the majority of the population is unsatisfactory. De La Rosa suggested that an average child removes only about 50% of the plaque present on teeth.14 Therefore poor oral hygiene occurring due to increased plaque and calculus deposits with increasing age has been reported among children and adolescents.15,16,17 This could be attributed to the fact that there is a lack of motivation among them to follow the practice of brushing as a regular habit and also they consider it as tedious.18 Majority of children show noncompliance towards brushing and they try to hide themselves from daily brushing task because they consider it as a tedious procedure which makes them dislike the brushing habit. At one point they tend to fail in developing a child’s interest in brushing. The level of oral hygiene achieved by an individual is dependent on a variety of factors such as motivation, duration &frequency.19,20 It is important to gain a child’s interest in brushing by introducing some new devices that the child can enjoy brushing. To make the tooth brushing habit more interesting to children and to gain their attention, a toothbrush with a music system has been used in this study. The use of musical talking toothbrush in children helps to overcome the problem of lack of motivation. The musical toothbrush has been developed specifically to appeal to children, with appropriately sized brush heads and features to introduce a “fun” aspect to tooth brushing. With this brush, the music plays when the child starts brushing and continues for up to 2 minutes until the music stops. This method is proposed to inculcate a habit of 2 minutes of tooth brushing among them. The previous literature says that music among children while brushing creates a positive mood, attention, and learning practices in the children. 21 Also to date few reported studies have been done to compare musical and regular toothbrush. Keeping this in mind, our objective of the study was to clinically evaluate and compare the efficacy in the plaque scores among the musical toothbrush over the regular toothbrush group among 6–11?year?old children.
MATERIALS AND METHODOLOGY
Study population: This study comprises 42 healthy kids (17 boys and 25 Girls) who fulfilled the inclusion criteria along with parental consent formed the sample for the study.
Approval: The study was undertaken with the understanding and written consent from the parents of each participant. The study design was approved by the Institutional Ethical Review Board, Saveetha Dental College, Chennai (IHEC/SDC-UG-1558/19/175).
Inclusion criteria:
-
Children between 6 to 11 years of age were selected for the study.
-
Children who were interested to participate in the study.
-
Cooperative children were included.
-
Patients who never used any other form of toothbrush before were included.
-
Patients with a minimum of twenty teeth present in their oral cavity.
Exclusion criteria:
-
Patients with poor oral hygiene with extrinsic stain and/or calculus deposits.
-
Evidence of major oral hard or soft tissue lesions.
-
History of a significant adverse event, allergy, or irritation that was due to oral hygiene products was eliminated.
-
Fixed or removable orthodontic appliances.
-
Medically compromised patients and disabled patients were excluded.
-
Subjects with severe crowding.
-
Children under any form of regular drug therapy were excluded from the study.
Experimental procedure:
Based on eligibility criteria, 42 participants were divided into two groups. The subjects were randomly assigned into two groups by a second examiner; Group 1 assigned a regular toothbrush (oral B-Chhotabheem) and Group 2 were assigned musical tooth (Aqua white musical chhotabheem). Group 1 brushed used regular toothbrush and Group 2 used a musical toothbrush. Only the second examiner knew which child had been given which brush, and was not involved in the recording of clinical parameters. And all clinical parameters were recorded by the first examiner. The children were taught the proper technique (horizontal scrub technique), and instructed on the proper use of their respective toothbrushes and performed their first brushing at the study site under supervision. They were then instructed to brush at home for two minutes twice daily for 45 days. They were also provided with standard fluoride toothpaste (Cheerio) and a diary to note any comments about their brushing experience. To achieve a standardized condition, each participant was provided with a common dentifrice. Also, their parents underwent training session on the brushing technique, using demonstration models. The children were familiarized with the disclosing agent, before the commencement of the study with the help of demonstrations. The subject’s parents were instructed to monitor tooth brushing and advised not to use another form of oral hygiene measures.
Instructions:
-
Subjects were asked to use only the given brushes following the specified taught technique.
-
Subjects were instructed to refrain from using any other oral hygiene products during the study.
-
Informed to brush twice daily each time for 2 min with the given dentifrice only.
-
Return for regular periodic examination on 15th day,30th and 40th day.
-
Advised not to use any medication which could have an inhibitory effect on plaque.
-
Refrain from brushing or any other forms of oral hygiene measures 24 hr before every recall visit.
Clinical Assessments
The clinical parameters were measured at 0 days, 15th day and 30th day and 45th day by the first examiner using Plaque Index (Quigley and Hein), The children were asked to refrain from all oral hygiene procedures for 24hr before every recall visit. The subjects brushed their teeth for 2 min under supervision using the assigned toothbrush and toothpaste. This was an examiner blinded study, so the brushing occurred at the study site in a separate room. Whole mouth plaque was assessed as described above, before and after the supervised 2min tooth brushing at each visit. Pre and post brushing plaque was scored using the Quigley Hein Plaque Index. Subjects swished with 5 ml of disclosing solution for 15 seconds, expectorated, and then rinsed with 10 ml of water for 10 seconds and expectorated. Plaque removal was assessed at each visit (day 0, day 15, day 30, day 45) following 24 hrs of no oral hygiene.
On day “0”
All the individuals who participated in the study were advised to refrain from brushing their teeth for 24 hr before their appointment on the day “0”. The plaque was disclosed by using a disclosing solution in the form of a rinse for all individuals. The pre brushing plaque score was recorded in the prepared pro forma by using the Quigley-Hein plaque index. Following this, the individuals were instructed to brush with the allocated toothbrush and toothpaste and the brushing technique in which they were instructed (Group 1 and Group 2) for 2 min. Re-examination was done after disclosing plaque, and the plaque score was recorded using the Quigley-Hein Plaque index. Further, the individuals were instructed to use the allocated toothbrushes using the prescribed brushing technique at home daily for 2 min and were given appointments on the 15th, 30th, and 45th days.
On the 15th day, 30th day, and 45th day:
The same investigational measures were carried out, and the Plaque index was evaluated and measured as that has done on the day “0”. Long term efficacy was evaluated by recording plaque scores following 24hrs of no oral hygiene at day 0 to day 45 and the values were obtained
STATISTICAL METHODS:
.The data collected were entered in the Microsoft Excel sheet following which statistical analyses were carried out using SPSS (Statistical Package for Social Sciences) Version 24.0 (IBM Corporation, Chicago, USA). The mean plaque scores were calculated using descriptive statistics. To assess variance in performance between 0, 15, 30 and 45 days, an independent t-test was carried out for comparing the plaque index among the two groups at each measurement day. Paired t-test was used to analyse the mean plaque score between visits. The level of statistical significance was set at 5% (p<0.05) with a 95% confidence interval.
RESULTS
The study was conducted in a single-blind manner with the first examiner being unaware of which subject was using which toothbrush. There were no dropout cases and all the subjects maintained their recall appointments. Comparison of the plaque index among the two groups at each measurement day was done by Independent t-test. Comparison within the groups of pre and post plaque index at each measurements day for Group 1 and Group 2 was performed by using Paired t-test. The results were interpreted as follows.
Mean Pre and Post brushing plaque index scores of Group 1 Individuals:
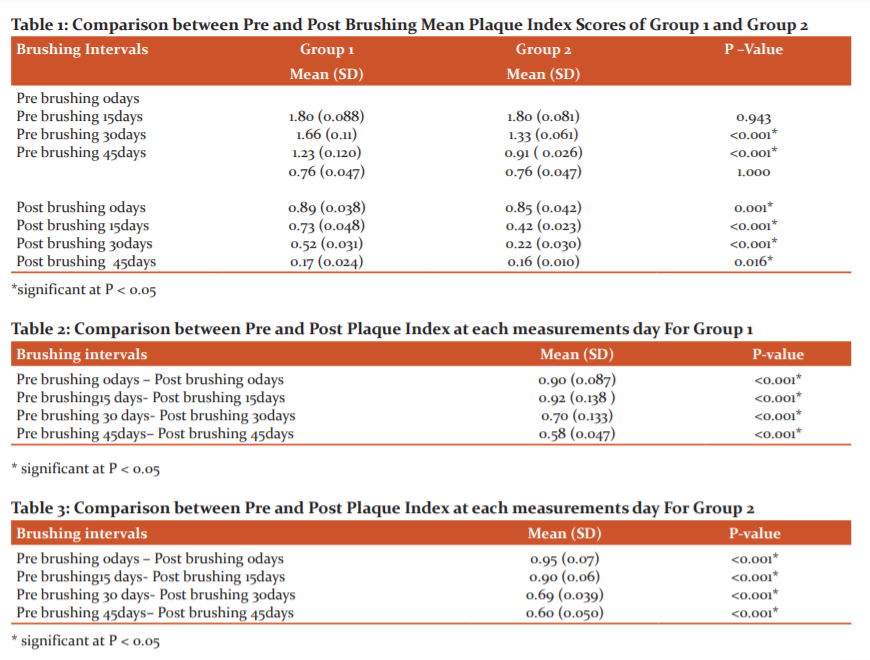
Mean Pre and post brushing Plaque index scores for Group 1 were 1.80,1.66,1.23,0.76 and 0.89,0.73,0.52,0.17 on 0,15,30 and 45th day respectively.
Mean Pre and Post brushing plaque index scores of Group 2 Individuals:
Mean pre and post brushing Plaque index scores for group 2 were 1.80, 1.33, 0.91, 0.76 and 0.85, 0.422, 0.22, 0.16 on 0, 15, 30 and 45th day respectively.
Comparison between Pre and post brushing mean plaque index scores of Group 1 and Group 2:
It shows the pre brushing mean plaque score for group 1 was 1.80, 0.7 and for group 2, it was 1.80, 0.70 on 0 and 45th days, respectively. The post brushing mean Plaque score for Group 1 was 0.89 and 0.17 and for Group 2 were 0.85 and 0.16 on 0 and 45th days, respectively. It proves at the 0 days the plaque score was fairly the same for both groups. On the 15th day and 30th day, there was a drastic drop in the plaque scores in group 2 (Table 1). When comparing pre brushing between group 1 and group 2 there was a statistically significant difference between the two groups on 0,15, and 30th day, there is a marked decrease in the plaque scores. On the 45th day of pre brushing between two groups, it was found to be not significant. When comparing the post brushing plaque scores of group 1 and group 2 there was a statistically significant result between two groups (p<0.05) on 0, 15, 30 and 45th day.
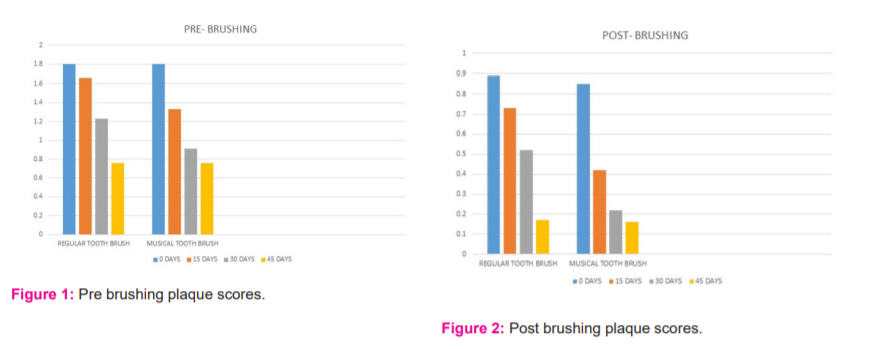
Intra-group comparison between pre and post brushing plaque index scores for group 1 and group 2:
The mean reduction in the Plaque score on intra-group comparison was, the difference at 0, 15, 30 and 45th day is represented in Table 2 & 3 it was found to be statistically significant when comparing between pre and post brushing. (Figure 1 and Figure 2)
DISCUSSION:
This study was conducted to assess the plaque removal potential of two different types of toothbrushes. When a new toothbrush is developed and introduced in the market, it is important to evaluate its efficacy in terms of plaque removal. Tooth brushing is the most common method of achieving and maintaining good oral hygiene. The use of good dentifrices does not assure proper removal of plaque; proper brushing technique plays an important role in oral health maintenance. The horizontal scrub method is more commonly used by children as it is easily learned. Several studies reported that horizontal scrubbing was the method of choice among young children and that they were unable to use other tooth brushing methods. 22,23,24 Mescher et al. 25 reported that 6 to 8-year-old children had difficulty performing sulcular brushing and that hand function was age-related. The development of motor skills associated with tooth brushing behaviour in children seems to be age-related. Horizontal scrubbing is a suitable technique when motor skills development is considered. Hence in this present study horizontal scrub method was used.
For clinically evaluating the cleaning efficacy of toothbrushes many indices have been developed, Quingleyhein has been suggested as a suitable one because of its ability to better assess the plaque build-up. The strength of this index is its application in clinical trials of preventive and therapeutic agents is well noted and also the same index was used in previously conducted studies.26-29 Hence choice of plaque index chosen was Quigley-Hein plaque index in the present study.
Post-brushing means Plaque index scores for Group 1 and Group 2 were evaluated and compared on days 0, 15, 30, and 45; it was found to be significant (P < 0.05) thus implying that the musical toothbrush cleaned supragingival plaque better than regular toothbrush over the 45 days, pre brushing comparison too showed statistically significant difference except at 45th day which was not significant due to Hawthrone effect. This proved that the toothbrush was effective in plaque removal for 6 to11-year-old children. However, the initial enthusiasm of getting a new type of toothbrush may also have encouraged the children to brush more frequently and regularly, later there was a likelihood of the ‘Hawthorne effect’. It’s a type of reactivity in which subjects modify or improve an aspect of their behaviour being experimentally measured in response to the fact that they are being studied or observed.30 Therefore results of this study indicated that the musical toothbrush has the potential to improve oral hygiene in children because it significantly reduced plaque accumulation.
It is well known that children generally do not spend enough time or care brushing their teeth. Methods that motivate children to adopt regular and effective oral hygiene practices, which improve their tooth brushing technique and effectiveness, are therefore extremely important. One way of improving both efficacy and motivation is by the use of a musical toothbrush which can be more fun to use than a regular toothbrush. The musical toothbrush is a smart toothbrush designed to teach and encourage tooth brushing in young children. To enhance compliance brush is designed with a musical timer for 2mins. It also has a bright, colourful design and features popular cartoon characters. When the sensors are activated, a music clip is played to encourage the user to toothbrush for at least two minutes. The desire of children to hear music while brushing makes effective motivation in children to learn and practice cooperative social skills. In this age group, play-based methods are the most effective means of solving behavioural problems. The feature in the musical toothbrush may all have contributed to the good compliance with tooth brushing seen in this study.
The musical toothbrush shows a pronounced reduction in plaque build-up in our study which correlates to studies by Ganesh et al. 31 and Nivetha et al. 32 In this brush, music starts while the child starts brushing, it continuous during the brushing and when this ends child should end the brushing. In addition, the toothbrush has a timer feature in and the brush is turned off after two minutes. Thus, this gives them a sense of happiness, fantasy, arousal, and energy to perform any work.
A study reported that parents identified the lack of time and the uncooperative behaviour of their children as the most common barriers toward brushing. To encourage the same and to improve their children’s cooperation toward brushing, the most common method was to make it “fun.” Children considered the musical toothbrush as an object of fantasy. Exposure to music show improves the child’s motor functioning and thereby enhances their transfer of learning task.33 Hence Parental involvement, in terms of monitoring and encouraging their children to maintain good oral hygiene practices, may also have increased compliance. Both parents and children considered musical toothbrush to be more fun to use than regular ones. Limitations of the study include individual pathogenicity of plaque formation.
CONCLUSION:
Although both the musical and the regular toothbrush effectively reduced the plaque scores to a greater extent, a highly statistically significant difference was noticed in post brushing 0 to 45th day and pre brushing 0 to 30th day except 45th day of pre brushing which can be due to outcome of “Hawthorne effect” cannot be overlooked. However, the musical toothbrush group had a better reduction in the scores during the study period on comparison also it has increased compliance with daily brushing which may improve overall hygiene.
ACKNOWLEDGEMENT:
The First author, Sarojini Ramya Pillay performed the analysis, and interception and wrote the manuscript. The second author, Dr.Jessy P, contributed to the conception, data design, analysis interpretation and critically revised and wrote the manuscript. The third author, Dr Subhabrata Maiti, revised the manuscript as per guideline, alignments and formatting.
CONFLICT OF INTEREST: The authors declared that they had no conflict of interest
ETHICAL CLEARANCE: The study design was approved before the commencement of the study by the Institutional Ethical Review Board (IHEC/SDC-UG-1558/19/175)
FINANCIAL SUPPORT: Nil
References:
1.Kwan SY, Petersen PE, Pine CM, Borutta A. Health?promoting schools: An opportunity for oral health promotion. Bull World Health Org. 2005;83:677?85.
2.NageshwarIyer, ShaluChandna, AshishLoomba. Plaque removal efficacy of Colgate 360 toothbrush: A clinical study. Contemp Clin Dent.2016; 7:317-21.
3. Petersen PE. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century--the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003; 31(Suppl 1): 3-23.
4. Macpherson LM, Anopa Y, Conway DI, McMahon AD National supervised tooth brushing program and dental decay in Scotland. J Dent Res. 2013; 92(2): 109-113.
5.Haffajee AD, Thompson M, Torresyap G, Guerrero D, Socransky SS. Efficacy of manual and powered toothbrushes. Effect on clinical parameters. J Clin Periodontol. 2001;28:937-46.
6. O'Leary TJ, Drake RB, Naylor JE. The plaque control record. J Periodontol. 972;43:38.
7. Sicilia A, Arregui I, Gallego M, Cabezas B, Cuesta S. A systematic review of powered vs. manual toothbrushes in periodontal cause-related therapy. J Clin Periodontol. 2002;29 (Suppl. 3):39-54.
8 . Hayaski H, et al. Tooth brushing for oral prophylaxis.Jpn Dent Sci Rev. 2014; 50:69-77.
9. Sharma NC, Qaqish J. A Clinical Evaluation of the Plaque Removal Efficacy of Five Manual Toothbrushes. J Clin Dent.2010; 21:8-12.
10. Grossman E, Proskin H. A comparison of the efficacy and safety of an electric and a manual children’s toothbrush. J Am Dent Assoc.1997;128:469-74.
11. Unkel JH, Fenton SJ, Hobbs G Jr, Frere CL. Tooth brushing ability is related to age in children. ASDC J Dent Child.1995; 62:346-348.
12. Bastiaan RJ.The cleaning efficiency of different toothbrushes in children. J Clin Periodontol. 1986;13:837?40
13. Benson BJ, Kenyon G, Grossman E. Plaque removal efficacy of two children’s toothbrushes: A one-month study. J Clin Dent. 1993;4:6-10
14. De la Rosa M, Zacarias Guerra J, Johnston DA, Radike AW. Plaque growth and removal with daily tooth brushing. J Periodontal. 1979;50:661-4.
15. Mbawalla HS, Masalu JR, Astrøm AN. Socio-demographic and behavioural correlates of oral hygiene status and oral health-related quality of life, the Limpopo?Arusha school health project (LASH): A cross-sectional study. BMC Pediatr. 2010;10:87.
16. Saied?Moallemi Z, Virtanen JI, Vehkalahti MM, Tehranchi A, Murtomaa H. School-based intervention to promote preadolescents’ gingival health: A community trial. Community Dent Oral Epidemiol. 2009;37:518?26.
17. World Health Organization. Information Series on School Health: Oral Health Promotion Through Schools. Geneva: World Health Organization. 2003.
18. Sandström A, Cressey J, Stecksén-Blicks C . Tooth-brushing behaviour in 6-12year olds.Int J Paediatr Dent. 2011;21(1): 43-49.
19. Sharma S, Yeluri R, Jain A, Munshi A. Effect of toothbrush grip on plaque removal during manual tooth brushing in children. J Oral Sci 2012; 54(2):183-190.
20.Stecksén-Blicks C, Sunnegårdh K, Borssén E (2004). Caries experience and background factors in 4-year-old children: Time trends 1967-2002. Caries Res. 38(2): 149-155
21. Stacey R, Brittain K, Kerr S. Singing for health: An exploration of the issues. Health Educ. 2002;102:156?62.
22.Claydon N, Addy M. Comparative single-use plaque removal by toothbrushes of different designs. J Clin Periodontol.1996; 23:1112-1116.
23.Sharma NC, Goyal CR, Qaqish JG, Cugini MA, Thompson MC, Warren PR, et al. Single-use plaque removal efficacy of three power toothbrushes. Journal of the dent.2005; 33:11-15.
24. Sharma NC, Goyal CR, Qaqish JG, Cugini MA, Thompson MC, Warren PR, et al. Plaque removal efficacy of two electric toothbrushes with different brush head design. J dent.2005; 33:17-21.
25.Mescher KD, Brine P, Biller I. The ability of elementary school children to perform sulcular tooth brushing as related to their hand functionality. Pediatr Dent. 1980; 2:31-36
26. Agerholm DM. A clinical trial to evaluate plaque removal with a double-headed toothbrush. Br Dent J. 1991;170:411–3.
27. Silverstone LM, Tilliss TS, Cross-Poline GN, Van der Linden E, Stach DJ, Featherstone MJ. A six-week study comparing the efficacy of a rotary electric toothbrush with a conventional toothbrush. ClinPrev Dent. 1992;14:29–34.
28. Tritten CB, Armitage GC. Comparison of a sonic and a manual toothbrush for efficacy in supragingival plaque removal and reduction of gingivitis. J Clin Periodontol. 1996;23:641–8.
29. Shibly O, Schifferle RE, Ciancio SG, Tarakji M, Mather ML. A clinical comparison of 2 electric toothbrush designs. J Clin Periodontol. 1997;24:260–3.
30. Killoy WJ, Love JW, Love J, Fedi PF, Tira DE. The effectiveness of a counter-rotary action powered toothbrush and conventional toothbrush on plaque removal and gingival bleeding. A short term study. J Periodontol. 1989;60:473–7.
31.Ganesh M, Shah S et al The effectiveness of a musical toothbrush for dental plaque removal: A comparative study. J Ind Soc Pedod Prev Dent.2012; 30(2):139-45
32. Nivedha S, Parangimalai D, Madan K. Effectiveness of Musical Toothbrush on Oral Debris and Gingival Bleeding among 6–10-Year-Old Children: A Randomized Controlled Trial. Indian J Den Res. 2019;30(2):196-99
33. Hogenesa M, Oersb BV, Diekstrac RF. The impact of music on child functioning. Eur J Soc Behav Sci. 2014;10:1507-26.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





