IJCRR - 13(14), July, 2021
Pages: 119-127
Date of Publication: 20-Jul-2021
Print Article
Download XML Download PDF
Relationship of Diabetes-specific Knowledge, Self-care Practices with Glycaemic Control: Urban and Rural Distinction in India
Author: Sudhanshu Ashok Mahajan, Jayashree Sachin Gothankar
Category: Healthcare
Abstract:Introduction: Quintessential information on knowledge and self-care practices about diabetes is rare in India and is critical to design general wellbeing strategies planned for forestalling and controlling diabetes. Aim: The present study was undertaken to assess and compare the knowledge of diabetes and self-care practices and their association with control of blood sugar levels in urban and rural areas in the Pune district, in India. Methodology: A study was conducted at 4 sites from urban and rural areas of the Pune district, in India. One registered private physicians' clinic from each study site i. e. from 2 wards and two villages were randomly selected. Methods and Material: Considering the 69% prevalence of good self-care practices in type 2 diabetics and requiring precision of 10%, the sample size of 200 was calculated. A predesigned, pretested questionnaire was filled by interview technique. Statistical significance between the two variables was tested using the Chi-square test and Fisher's exact test. The correlation was tested by using Pearson's correlation coefficients. Results: The mean total knowledge score of urban diabetics (7.52) was more than the mean total knowledge score (6.62) of the rural diabetic. (p< 0.05). A significant difference was found between the urban and rural diabetics about the self-care practices except for compliance to drugs. No correlation of diabetes knowledge score with Glycosylated Haemoglobin was seen in an urban and rural area. Conclusion: Endeavours ought to be made to develop self-care practices of patients in shutting the hole of diabetes knowledge. Health care providers should be empowered for delivering adequate health message regarding diabetic self-care practices.
Keywords: Urban-Rural, Type 2 diabetes, Knowledge, Self-care
Full Text:
INTRODUCTION
Papyrus Ebers was the first name given to diabetes by an Egyptian physician Hey-Ra (1552 BC).1 Diabetes is the third most common health disorder worldwide and the fourth leading cause of death.2 The World Health Organization estimates that diabetes mellitus affects at least 285 million people and causes 3.2 million deaths, six deaths every minute and 8700 deaths every day, and this figure will increase by 70% in developed countries, and by 42% in developing countries by 2030.3
India with its dubious distinction of being designated, “The Diabetic Capital of the World” is presently estimated to have over 30 million individuals affected by this deadly disease.4As per the WHO report 2012 if India doesn’t wake from its slumber, by 2025, each fifth diabetic on earth would be an Indian.5The prevalence of diabetics in Indian adults was found to be 2.4% in rural and 4-11% in urban dwellers.6
Diabetes is one of the fastest-growing challenges in the 21st century and the stream of the diabetes epidemic is changing at a great rate.7 Once a disease of the West, diabetes has now spread to each nation on the planet. Once “a disease of affluence,” it is now increasingly common among the poor.8 Very high levels of diabetes have been reported in urban areas of India but little data are available for rural regions where >70% of the population lives.9Rural populations are at a high risk of developing diabetes mellitus as a result of the shift in epidemiology from communicable disease to non-communicable disease.10
Diabetes self-care is extremely complex, requires life-long commitment and modification of one’s lifestyle. Good self-care practices and adherence to the recommendations have been found to associate with good blood sugar control.11
Despite the abundance of studies on diabetes, there is limited information available on the knowledge and self-care practices with comparison in urban and rural areas. To address this demand, the present study was undertaken with the aims and objectives of
-
To assess and compare the knowledge of diabetes and self-care practices in urban and rural areas in Pune district and
-
To determine the association of knowledge and self-care practices of diabetes with control of blood sugar levels.
MATERIAL AND METHODS
An OPD-based, cross-sectional study was executed amongst type 2 diabetes mellitus inside the urban and rural district, Pune, to evaluate their knowledge regarding the disease and the self-care practices that have been followed by them and those have been correlated with their control of diabetes (Hba1c). Considering the 77%12 prevalence of self-care practices in type 2 diabetics and requiring precision of 12%, the sample size of 82 was calculated using the formula, 4 pq/l2. Thus, the study was conducted among 200 patients (100 from urban and 100 from rural) with a known history of type 2 diabetes, who were 30 years of age and above and residing in that locality for more than a year. The type 2 diabetics excluded those who were pregnant, had steroid-induced hyperglycaemia and were unable to give informed consent.
Selection of study population from urban and rural areas
Selection of study population from urban areas:
There are 15 regional ward offices under Pune Municipal Corporation.13 Out of the 2 wards viz. Bibwewadi and Dhankawdi were selected by random sampling technique. A list of registered private physician’s clinic/s from each selected ward was obtained. One registered private physician’s clinic from each Bibwewadi and Dhankawdi ward was selected purposively.
Selection of study population from rural areas:
There are 15 talukas in the Pune district.14 Out of 15, 1 taluka viz. Bhor was selected by random sampling technique. There are 194 villages under Bhor taluka.15 Out of the 2 villages viz. Nasrapur and Narhe were selected purposively as they owned a better private medical facility. A list of all registered private physician’s clinic/s was obtained from each of these selected rural villages and one registered private physician’s clinic was selected randomly from each village.
After obtaining Institutional Ethics Committee clearance BVDU/MC/61 from Bharati Vidyapeeth Deemed to be University Medical College and Hospital, the permission of consulting physician/in-charge of clinics was obtained. All the known type 2 diabetic patients coming in the selected clinics in the study period were fully informed regarding the purpose of the study. The patient information sheet was explained to each patient and written consent was obtained before data collection. Patients were examined and interviewed at the time of the respective clinic’s timings. The Interview was started with a general discussion to build rapport with the subjects and to gain confidence. A predesigned, pretested questionnaire was filled by interview technique to collect socio-demographic information, personal history, general examination, diabetes-related information, knowledge regarding diabetes, and the self-care practices that were followed by them. Anthropometry included measurement of height and weight. The questionnaire was reviewed by three experts before being utilized – a public health expert, a diabetologist, and a statistician and their proposals were used for improving the questionnaire thus ensuring consensus validity of the instrument. Initially, a pilot study was done on 10% of type 2 diabetic patients in urban and rural clinics of the Pune district outside the study area.
Knowledge was assessed using closed-ended questions, and the study subjects were classified as having adequate, inadequate-poor and no knowledge depending on the score obtained. Details regarding self-care practices were also collected.
Biochemical tests were done by organizing a health camp on a predetermined date in selected urban and rural clinics. Blood samples of all selected type 2 diabetics were collected by a trained nurse. For each patient, blood samples were obtained in the morning after 10 hours fast, from the antecubital vein in a sitting position for determination of HbA1c level. Glycosylated haemoglobin was estimated using high-performance liquid chromatography on National Glycohemoglobin Standardisation Program certified instruments16 from a registered laboratory.
The data were collected and entered in Microsoft Excel Office 2015 and SPSS statistics version 20 was used for statistical analysis. The data were expressed in suitable tabular formats. Percentage, mean and standard deviation were calculated. Statistical significance between the two variables was tested using the Chi square test and Fisher's exact test. The correlation was tested by using Pearson's correlation coefficients. p-value <0.05 was considered as significant.
RESULTS
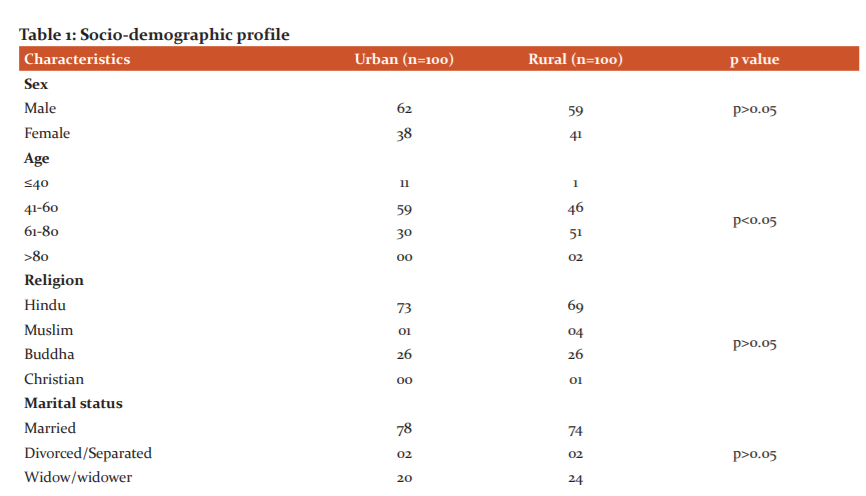
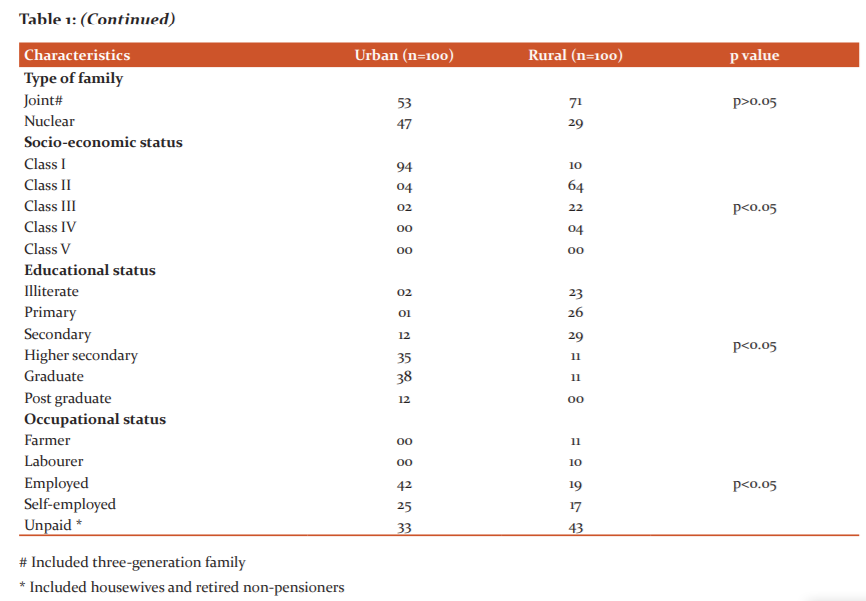
The baseline characteristics of diabetics are shown in Table 1. Majority i.e. 121 (60.5%) diabetics were male and 79 (39.5%) diabetics were female. The mean age of urban diabetics is 53.67 years as compared to 62.21 years in rural diabetics. The vast majority of people in India belong to Hinduism and current research has led to similar finding (71% were Hindus). Almost three-quarters of diabetics i.e. 152(76%) were currently married followed by 44(22%) were widow/widower. Maximum diabetics i.e. 71 from rural area belonged to either joint or three-generation families and 47 from urban area belonged to nuclear families. Similar to the standard watched these days, nuclearity is expanding and jointness is diminishing in groups of the urban area and the same may have been reflected in the present study. Most of the urban diabetics were either doing service or self-employed and the majority belonged to the upper class as per Modified B. G. Prasad Socio-economic Classification.
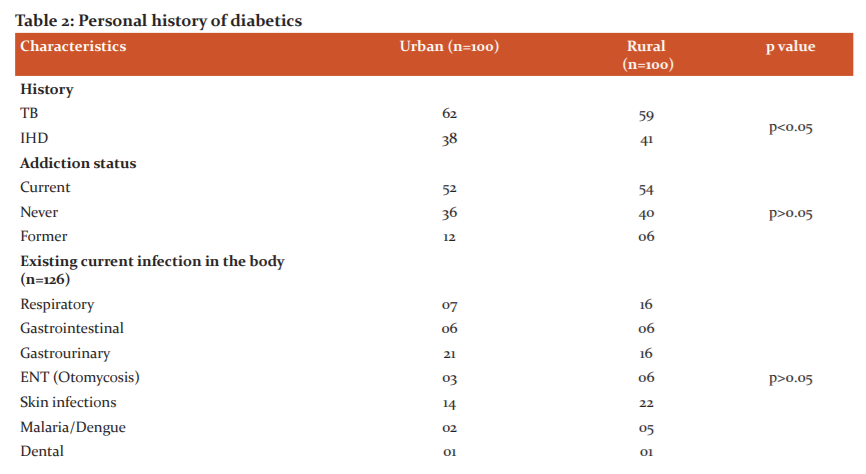
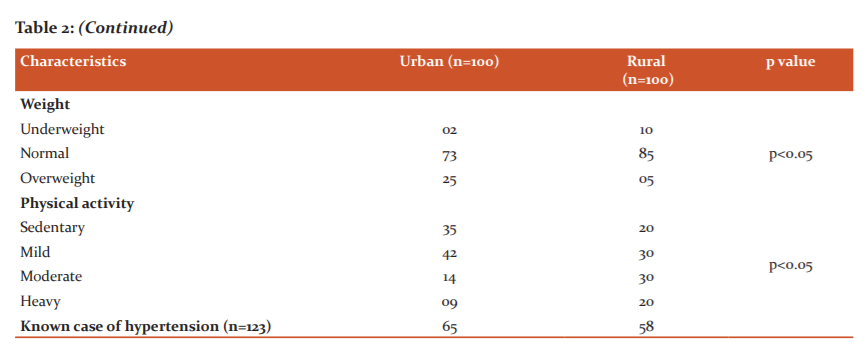
The personal history of diabetes of the study population is presented in Table 2. More than half of diabetics (53%) were currently addicted to smoking, alcohol consumption and chewing tobacco. Maximum i.e. 29.3% diabetics revealed that they were suffering from genitourinary infections that include balanitis, vaginitis, cervicitis, urinary tract infections. Results indicate that 79% of diabetics had normal weight and 15% were overweight as per National Institute of Nutrition guidelines. Physical activity shows that about one-third (29%) reported having heavy physical activity of which 20% were from rural and 9% from urban area. Among the patients, almost 61.5% accepted having comorbidity in the form of Hypertension.
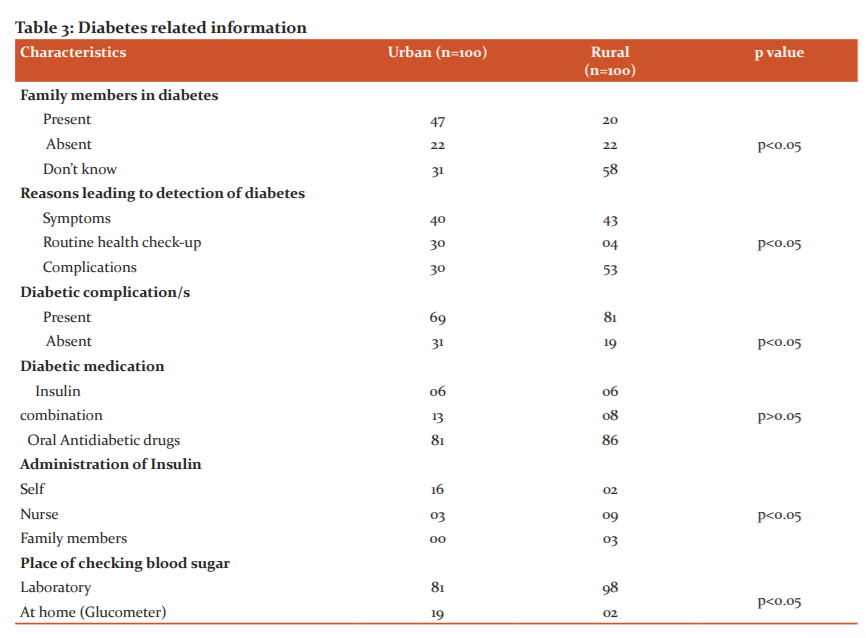
Diabetes-related information is given in Table 3. Family history of diabetes was revealed by the higher number of diabetics in an urban area (47%) than in rural area (20%). Nearly 41% of patients developed symptoms like weakness, polyuria, etc which subsequently led to the diagnosis of diabetes. The majority of diabetics i.e. 75% revealed that they were suffering some form of diabetic complications like retinopathy, neuropathy, nephropathy, diabetic foot, etc. Out of 33 insulin users, 54% administered insulin by themselves. Maximum diabetics i.e. 89.5% done their blood sugar tests at the pathology laboratory.
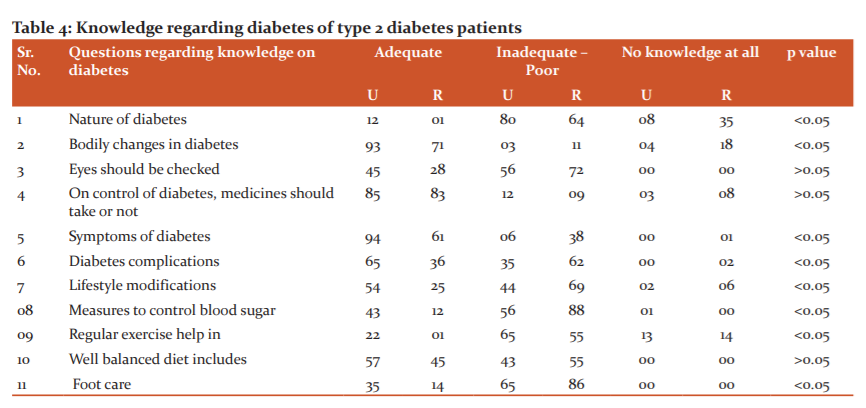
Knowledge deficit was noted in eight questions, in descending order these were related to symptoms of diabetes, nature of diabetes, measures to control blood sugar, lifestyle modifications, diabetes complications, bodily changes in diabetes and foot care. Results are shown in Table 4.
The mean total knowledge score of urban diabetics (7.52) was more than the mean total knowledge score (6.62) of the rural diabetic. (p<0.05).
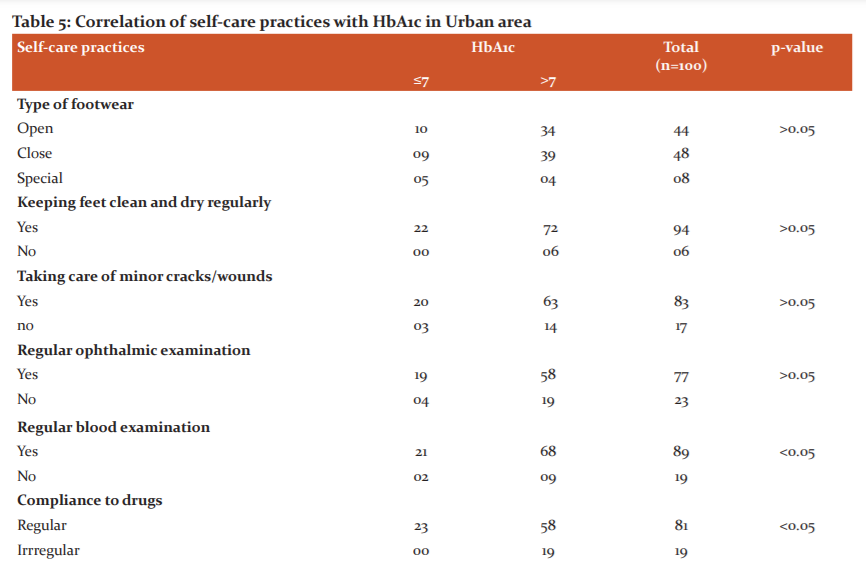
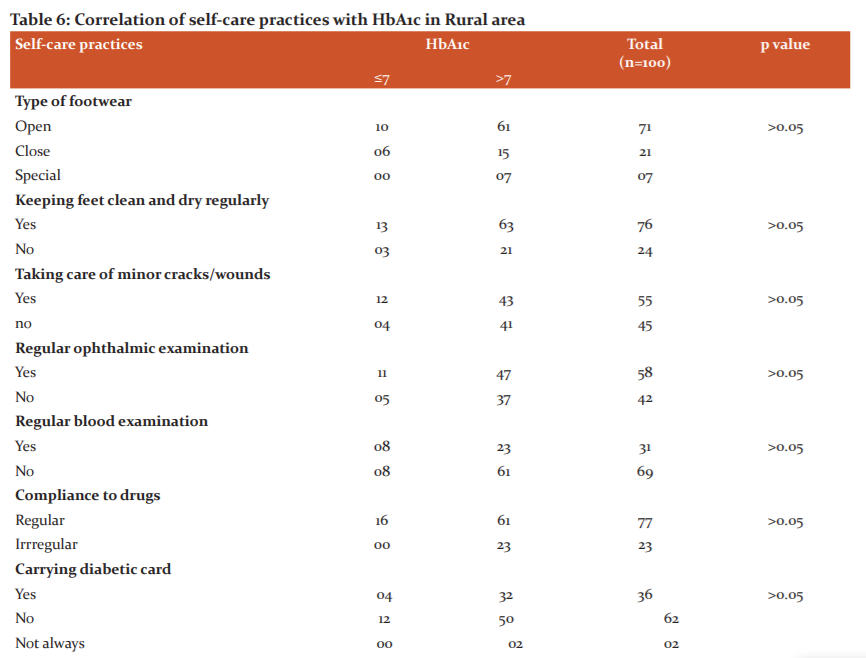
The correlation of self-care practices with HbA1c in urban and rural areas are shown in Table 5 and Table 6. No statistically significant association was found between almost all self-care practices except compliance to drugs with good control of blood sugar level in the urban area. No correlation was seen for any of the self-care practices with HbA1c levels in the rural area including compliance to drugs.
A correlation was evaluated between diabetes knowledge score with Glycosylated Haemoglobin (HbA1c) in an urban area and rural area which on analysis revealed Pearson correlation value of 0.055 for urban and 0.022 for rural diabetics. The p-value was 0.029 for urban diabetics and 0.105 for rural diabetics which were statistically non-significant indicating that diabetes knowledge score and glycosylated haemoglobin did not correlate both in urban and rural areas.
DISCUSSION
The present study was done to assess the knowledge and self-care practices in regards to diabetes and their association with control of blood sugar levels in 100 urban and 100 rural diabetics in the Pune district.
A large portion of the study participants from the urban area was underneath 40 years of age than in rural area. Young urban diabetics in the present study might be expected on account of the stationary way of life and absence of physical activity and more intake of cheap and high-calorie food and detection rate is early a direct result of higher awareness among urban people. In contrast to our study, Muninarayana C et al.17 reported that diabetes in young adults was common in less than 45 years of age. The likely purpose behind finding the more young rural diabetics was that this17 study was finished by the house to house screening and they may have been discovered undiagnosed diabetes.
In the present study, the majority of diabetics were males both from urban and rural areas. Men seem more susceptible than women to the consequences of indolence and obesity, possibly due to differences in insulin sensitivity and regional fat deposition. Men are more prone to type 2 diabetes because men develop the disease at a lower body mass index than women.18
The present study shows more than half, 52% of diabetics belonged to socio-economic class I. However urban diabetics (94%) are significantly more than rural diabetics (10%) in the same class. None of the patients was found in class V. The probable reason may be the non-affordability of the diabetic patients for taking treatment in private clinics. However, Nitendra Cet al.19, Nikhil P H et al.20, found the majority of urban diabetics in class IV and class V as their studies were done in urban slum area.
It should be noted that we found, though the farmers and labourers are engaged in physical activity they still have diabetes. This observation is in line with other study conducted in rural Maharashtra.21 Diabetes is estimated to increase the risk of TB from 1.5 to 7.8 fold 22 and this is observed in our study, as almost 15% suffered from T.B after the diagnosis of diabetes. The majority of them, i.e. 20 were from the rural area.
Addiction is always a dangerous disease, but it can be especially life-threatening for diabetics. In the present study, it is revealed that 9% of patients stopped addictions permanently after they were diagnosed with diabetes and this number was found to be double in urban diabetics (12%) as compared to rural diabetics (6%). The inducement and will strength of quitting addictions visible double in urban diabetics is may be due to the extra time given by their medical doctor and more interactive counselling sessions.
In our study, we exposed that out of 30 overweight diabetics, 25 were from urban and only 5 were from the rural area. This may be due to rural diabetics might be consuming less refined or energy-dense food and being more physically active and less sedentary than urban diabetics.
Awareness of one of the major risk factors for diabetes was poor as the majority of rural diabetics (58%) didn’t know about their diabetes family history.
It is observed that 30% of urban diabetics were diagnosed with diabetes during routine health check-up than 4% of rural diabetics, since greater awareness as well as the practice of recurring health check-up at regular intervals in the urban area leading to the detection of diabetes.
The majority of diabetics i.e. 150 (75%) revealed that they were suffering some form of diabetic complications like retinopathy, neuropathy, nephropathy, diabetic foot, erectile dysfunctions, etc. Significantly more rural diabetic (81%) with complications were found as compared to urban (69%.)
It is worrisome that only 8% of urban diabetics had adequate knowledge about diabetes being a non-communicable disease. Nearly 93 urban diabetics reported that they knew what diabetes is and the remaining were unaware of it (p<0.05).
An encouraging part of the study is that although there was, quite low diabetic score in rural area, nearly 83 rural diabetics knew that diabetes required lifelong treatment and this implies that they were ready to change if motivated or educated properly.
Lifestyle modifications like weight reduction, quitting of smoking and alcohol were essential for the control of disease was agreed by most of the urban diabetics as compared to rural (p<0.05)
It was surprising to see that rural diabetics were having inadequate knowledge of complications. It partly reflects that patients are not sensitized about the complications of diabetes which can have dreadful consequences in terms of mortality and morbidity. Several reasons have been cited for this including lack of time, an inappropriate way of providing information, lack of trained support staff like diabetic educators.
Regarding foot care, 76% of rural diabetics who wear open footwear checked their feet and inspected the inside of their shoes daily. None of them wore footwear inside their houses, both in urban and rural areas. The practices that were best followed were checking of blood sugars at least once in 3 months and as advised by the doctor which accounted for 100% of the urban diabetics.
Among all self-care practices, the patient’s compliance was found to be better despite poor educational status in rural diabetics. The old rural areas ancient thinking of considering a doctor as a God has been seen here.
In our study, the higher the education of urban diabetics, the higher was the knowledge but the lesser the blood sugar control. Despite their adequate knowledge, due to their work and other commitments, they might not be able to implement treatment or spend a long time on non-therapeutic measures.
CONCLUSION
Thus it is to conclude that the present study reflects the poor knowledge and self-care practices in rural as compare to urban diabetics but compliance is better with medical aspects of the regime than with lifestyle aspects in rural diabetics. This predisposes them to the risk of development of complications in later life. This study also demonstrated that knowledge of diabetes alone does not necessarily affect glycaemic control in urban areas.
The findings of present study were restricted to patients attending the physician’s clinic in a selected hospital and hence may not be generalized to patients from different socioeconomic backgrounds. Additional research in a larger sample size in the general study population was needed to replicate and extend these findings.
Acknowledgement: We would like to express our deep gratitude to the Principal of our Medical College for permitting us to carry out this research project. Our thanks to Mr S P Sane, statistician of the department for their help.
Conflict of interest: Nil
Source of funding: Nil


References:
-
Lakhtakia R. The History of Diabetes Mellitus. Sultan Qaboos University Medical Journal 2013;13(3): 368-370.
-
Tabish SA. Is Diabetes Becoming the Biggest Epidemic of the Twenty-first Century? Int J Health Sci. 2007 Jul;1(2): V-VIII.
-
Habtamu SM. Rehabilitative Care of Adult with Diabetes Mellitus. JOJ Case Stud. 2018; 9(2): 555758.
-
Ramachandran A. Epidemiology of diabetes in India--three decades of research. J Assoc Physicians Ind. 2005 Jan;53:34-8.
-
Sovindra KB, Avantika S, Ranjeet S. Ind J Res Pharm Biote.2014 Jan-Feb;2(1):958-964.
-
Khatib N, Qazi Z, Gaidhane A, Waghmare T, Goyal R. Risk factors of type-2 diabetes mellitus in rural Wardha: A community-based study. Int J Diab Devel Coun. 2008;28(3):79.
-
Wagh S, Bhagat S, Bankar N, Jain K. Role of Vitamin-C Supplementation in Type II Diabetes Mellitus. Int J Curr Res Rev. 2020;12(13):61-64.
-
Hu F. Globalization of Diabetes: The role of diet, lifestyle, and genes. Diabetes Care. 2011;34(6):1249-1257.
-
Chow C, Raju P, Raju R, Reddy K, Cardona M, Celermajer D et al. The Prevalence and Management of Diabetes in Rural India. Diab Care. 2006;29(7):1717-1718.
-
Mohan V, Deepa R. Risk factors for coronary artery disease in Indians. J Assoc Phys Ind. 2004;52:95–7.
-
Basu S, Garg S, Sharma N, Singh M, Garg S. Adherence to self-care practices, glycemic status and influencing factors in diabetes patients in a tertiary care hospital in Delhi. Wor J Diab. 2018;9(5):72-79.
-
Dasappa H, Prasad S, Sirisha M, Ratna Prasanna SVN, Naik S. Prevalence of self-care practices and assessment of their sociodemographic risk factors among diabetes in the urban slums of Bengaluru. J Family Med Prim Care. 2017 Apr-Jun;6(2):218-221.
-
About PMC [Internet]. Pmc.gov.in. 2021 [cited 9 February 2021]. Available from: https://www.pmc.gov.in/en/about-pmc.
-
Pune Tehsil Map, Talukas in Pune [Internet]. Mapsofindia.com. 2021 [cited 9 February 2021].
-
Villages & Towns in Bhor Taluka of Pune, Maharashtra [Internet]. Census2011.co.in. 2021 [cited 9 February 2021]. Available from: https://www.census2011.co.in/data/subdistrict/4198-bhor-pune-maharashtra.html
-
Ngsp.org. 2021 [cited 9 February 2021]. Available from: http://www.ngsp.org/docs/methods.pdf.
-
Muninarayana C, Balachandra G, Hiremath SG, Iyengar K, Anil NS. Prevalence and awareness regarding diabetes mellitus in rural Tamaka, Kolar. Int J Diabetes Dev Ctries. 2010 Jan;30(1):18-21.
-
Geer E, Shen W. Gender differences in insulin resistance, body composition, and energy balance. Gender Med. 2009;6:60-75.
-
Chaurasia N, Thapa B, Patil B, Khandekar S, Angolkar M, Narasannavar A et al. Knowledge of Urban Population Regarding Diabetes Mellitus and its Complication: A Community Based Study. J Nobel Med Coll. 2014;3(1):62-65.
-
Hawal N, Kambar S, Patil S, Hiremath M. Knowledge, attitude and behaviour regarding self-care practices among type 2 diabetes mellitus patients residing in an urban area of South India. Int Multi Res J .2013;2(12)371-374.
-
Gholap MC, Mohite VR. To assess the knowledge and practice regarding foot care among diabetes patients at Krishna hospital, Karad. Ind J Sci Res. 2013 Jul 1;4(2):69-75.
-
Niazi A, Kalra S. Diabetes and tuberculosis: a review of the role of optimal glycemic control. J Diab Metab Dis. 2012;11(1): 281-285.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





