IJCRR - 13(14), July, 2021
Pages: 85-92
Date of Publication: 20-Jul-2021
Print Article
Download XML Download PDF
Platelet and Coagulation Parameters in Pregnancy Induced Hypertension and Eclampsia - A Tertiary Hospital Based Study
Author: Sharma B, Arora S, Kumar R, Bali IK
Category: Healthcare
Abstract:Introduction: Pregnancy-induced hypertension (PIH) is defined as newly diagnosed hypertension that occurs in pregnancy after 20 weeks of gestation and disappears following delivery of the baby. The inclusion of platelet and coagulation parameters along with routine investigations helps in the early prediction of the severity of PIH and Eclampsia. Aim: To know the changes in platelet and coagulation parameters in PIH and Eclampsia which can help in timely treatment and thus can help in the reduction of maternal and perinatal deaths associated with PIH and eclampsia. Material and Methods: The study was undertaken at the Department of Pathology, Shree Guru Gobind Singh Tricentenary Medical College and Hospital, Gurugram for 1 year on 56 patients diagnosed with PIH and Eclampsia. Results were compared with 56 normotensive pregnant females. Results: Mean Bleeding Time, Clotting Time was found to be normal in all patients of PIH and Eclampsia; but Prothrombin Time, activated partial thromboplastin time were significantly found to be higher and decreased platelet counts were observed with increasing grades of PIH and Eclampsia. Conclusion: Platelet and Coagulation Parameters In Pregnancy-induced hypertension and Eclampsia \? A Tertiary Hospital Based Study.
Keywords: Coagulation profile, Platelet parameters, Pregnancy-induced hypertension
Full Text:
INTRODUCTION
Pregnancy-induced hypertension (PIH) is defined as newly diagnosed hypertension that occurs in pregnancy after 20 weeks of gestation and disappears following delivery of the baby. Out of all the haematological changes that happen in PIH associated cases, thrombocytopenia is the most widely recognized haematological abnormality. The degree of thrombocytopenia increases with the severity of the disease.1
The most common medical disorder associated with pregnancy is Pregnancy-induced hypertension which leads to multi-organ failure in the mother and the hallmark placental lesion in preeclampsia is acute atherosclerosis of the decidual arteries which leads to poor placental perfusion causing intrauterine growth restriction, fetal distress which can ultimately result in fetal death. Worldwide, PIH is considered a leading cause of maternal and perinatal morbidity and mortality.2
Thrombocytopenia is more commonly seen in women who develop severe preeclampsia and eclampsia and women with the underlying disease of the chronic vascular system are more commonly affected with thrombocytopenia. Pre-eclampsia is an important health issue that needs to be dealt especially in developing countries.3-6
Preeclampsia can be diagnosed by persistently increased blood pressure during pregnancy and also during the postpartum period with associated proteinuria associated with thrombocytopenia and kidney or liver functions derangements etc.8
As per recent data according to National Health Portal, In India, the prevalence of hypertensive disorders of pregnancy was reported in 7.8% cases whereas 5.4% of the study population had associated preeclampsia. HELLP (hemolysis, elevated liver enzymes and low platelet count) syndrome and Eclampsia are the serious complications of pre-eclampsia. Preeclampsia and later development of eclampsia results in the most serious outcomes in mother and baby and are associated with vasospasm, vascular lesions in multiple organs, increased activation of platelets and subsequently cause coagulation system activation in the microvasculature.
Hypercoagulability is constantly associated with hypertensive disorders of pregnancy and particularly associated with pre-eclampsia. Thus, routine coagulation profile testing is commonly required in these patients to look for any evidence of Disseminated intravascular coagulation (DIC) and HELLP syndrome.8
MATERIALS AND METHODS
A Prospective Observational study was done on a total of 112 pregnant females with 56 Normotensive Pregnant females were taken as controls and 56 patients diagnosed with Pregnancy Induced Hypertension (PIH) as cases. Investigations were done in the Department of Pathology, FMHS, SGT Hospital, Gurugram on the cases who were admitted for delivery in the department of Obstetrics and Gynecology. The data was collected from the patients’ records.
Approval for waiver of patients consent and patient information sheet was obtained from Institutional Ethical Committee since the study involved the data available in the record that were anonymized and coded to delink with any identity of the patient. 10-15
Patients were divided into a total of 5 study groups: Normotensive Pregnancies Group, Gestational hypertension group, Mild Preeclampsia Group and Severe Preeclampsia Group as per Williams Obstetrics Textbook 25th edition 2018 table 40-1 classification given by American College of Obstetricians and Gynecologists and the fifth group as Eclampsia. Eclampsia is defined as preeclampsia complicated by seizures -
1. Gestational Hypertension: Diagnostic criteria:
New-onset hypertension developing after 20 weeks of gestation in a previously normotensive woman having BP 140/90 mmHg and without proteinuria.
2. Pre-eclampsia: Diagnostic criteria:
1. 20 weeks of gestation
2. Blood pressure of 140/90 mmHg or greater when readings are taken twice, six hours apart.
3. Proteinuria of 1+ or greater by dipstick method or ≥ 300mg/24h or Urine protein: creatinine ratio ≥0.3.
Preeclampsia is further categorized into- Mild Pre-Eclampsia with Systolic BP between 140-160 mmHg and Diastolic BP 90-110 mmHg and Severe Pre-Eclampsia with Blood Pressure greater than 160/110 mmHg and other associated signs and symptoms. 16-19
Eclampsia: Preeclampsia associated with seizures.
1) PERIOD OF STUDY: 1 year.
2) INCLUSION CRITERIA:
i) Pregnant women with more than 20 weeks of gestation with pregnancy-induced hypertension.
ii) Normotensive pregnant women with more than 20 weeks of gestation.
3) EXCLUSION CRITERIA:
Pregnant women--
i) With Pre-existing/Chronic Hypertension cases.
ii) With known bleeding disorders.
iii) On anticoagulant therapy.
iv) In Labor.
v) With established DIC.
vi) Pre-existing Renal Disease.
Following Routine Blood investigations were done-
1. Platelet Count- By using Sysmex XN 550 Six-part Hematology analyzer.
2. MPV (Mean platelet volume) – By using Sysmex XN 550 Six-part Hematology analyzer.
3. PDW (Platelet distribution width) – By using Sysmex XN 550 Six-part Hematology analyzer.
4. Bleeding time (BT) - By Duke’s method.
5. Clotting time (CT) - By Wright’s capillary tube method.
6. Prothrombin time (PT) – By using ERBA Manhelm ECL 412.
7. Activated partial thromboplastin time (aPTT) – By using ERBA Manhelm ECL 412.
STATISTICS:
Statistical analyses were compiled by using Excel sheets and the data collected was transferred to the latest version of Statistical Package for Social Services (SPSS) software and the Chi-square test was used as a test of significance for categorical variables. A P-value less than 0.05 was considered statistically significant. 19,20,21
RESULTS
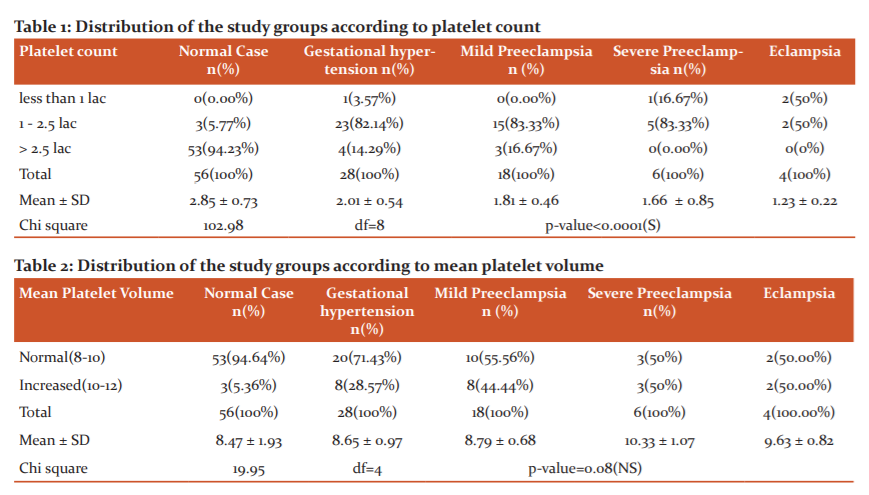
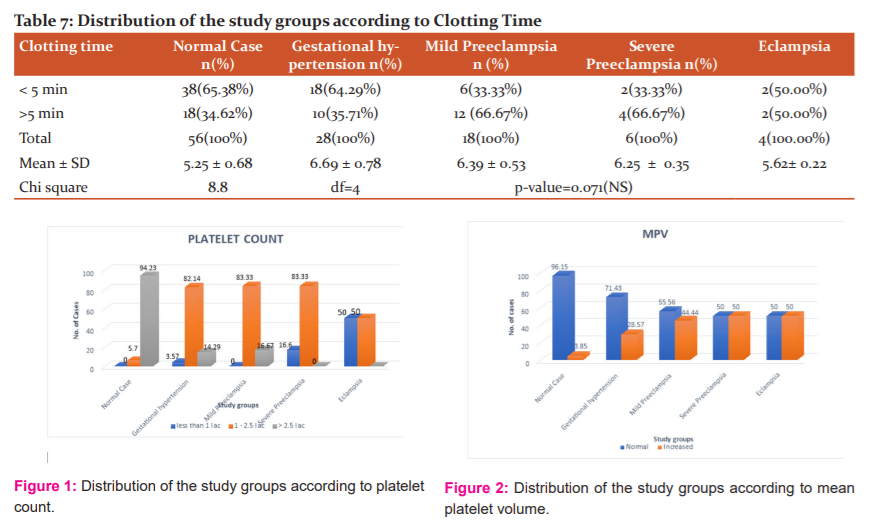
Platelet count was found to be less than one lakh in about 3.5% of gestational hypertension patients, 16.6% cases of severe preeclampsia and was found to be less than 1 lakhs in 50 per cent of eclampsia cases. Maximum cases of gestational hypertension 82.1% and 83.3% of cases of both mild and severe preeclampsia showed platelet count between 1.0 -2.5 lakhs. The result was statistically significant as shown in Table 1 and Figure 1.
Mean platelet volume (MPV) was found to be increased in 28.5% cases of gestational hypertension and increased in 44.4% of the mild preeclampsia patients and 50% of severe preeclampsia and eclampsia patients, but this increase in mean platelet volume was not found to be statistically significant as shown in Table 2 and Figure 2.
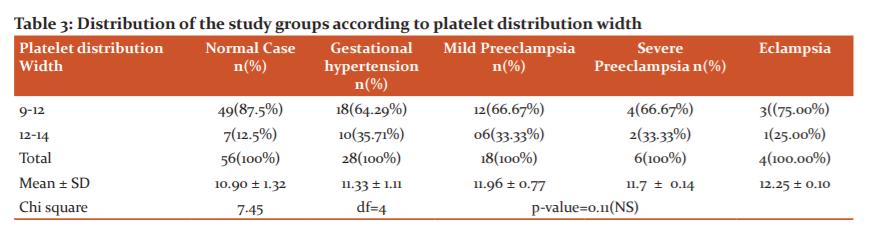
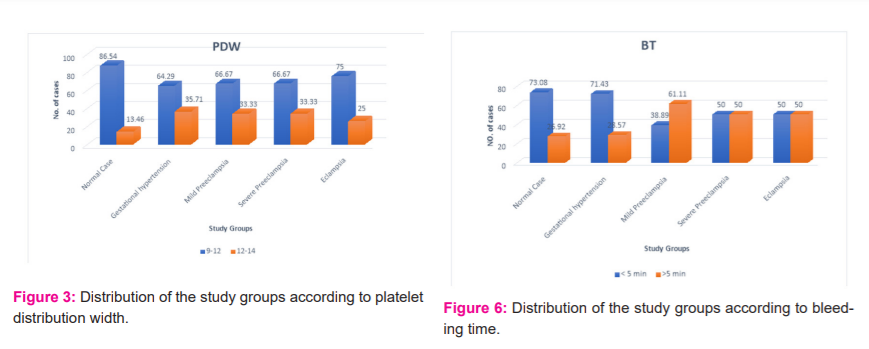
Platelet distribution width (PDW) - 35.7% of cases with gestational hypertension, 33.3% of the cases with mild preeclampsia and 33.3% cases of severe preeclampsia and 25% of eclampsia cases showed results range between 12 to 14 fl. Results were not significant as shown in Table 3 and Figure 3.
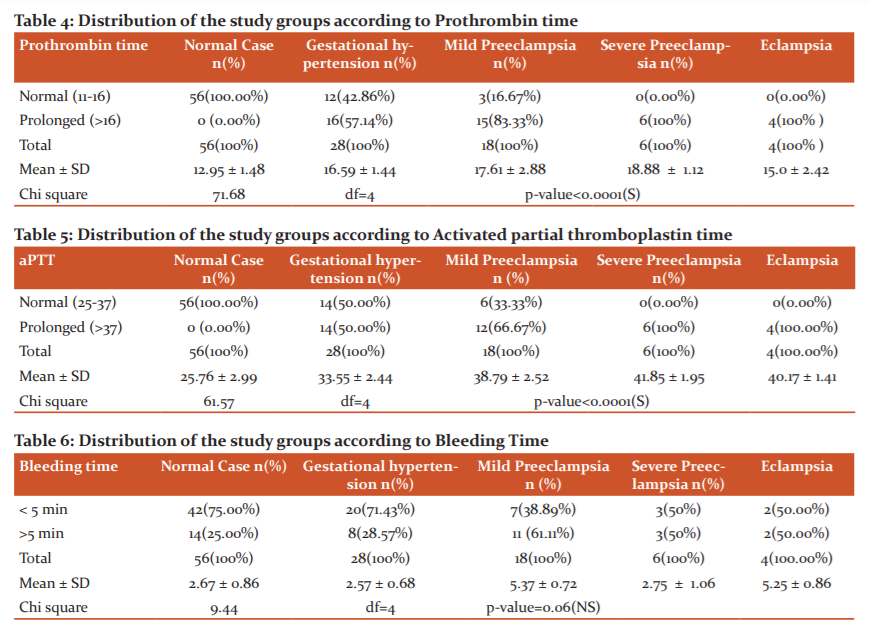
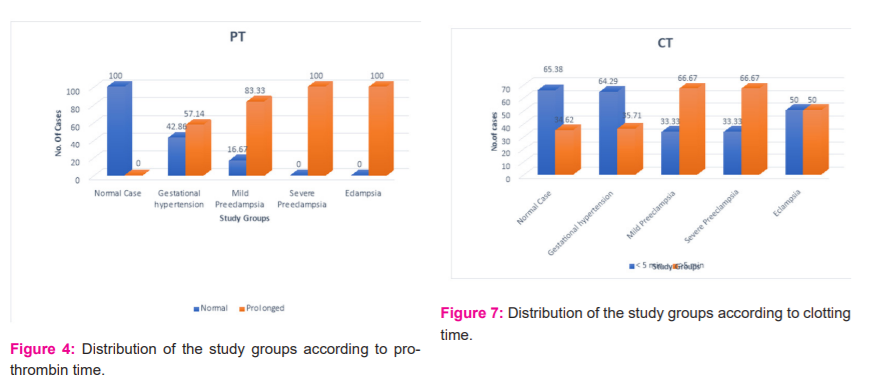
Prothrombin time (PT)- The mean prothrombin time of patients with gestational hypertension was 16.5 secs, mild preeclampsia patients were 17.6 secs and severe preeclampsia patients was 18.8 secs and 15 secs in the eclampsia group. 57.1% of cases with gestational hypertension, 83.3% of cases with preeclampsia and 100% cases of severe preeclampsia and eclampsia showed prolonged prothrombin time. Results were statistically significant as shown in Table 4 and Figure 4.
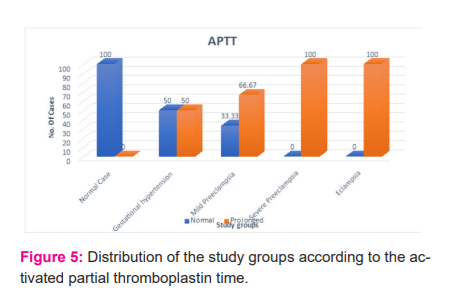
Activated partial thromboplastin time (APTT) - The mean activated partial thromboplastin time in patients with gestational hypertension was 33.5 secs, mild preeclampsia patients were 38.7 secs and severe preeclampsia patients was 41.8 secs and 40 secs in the eclampsia group. 50% of gestational hypertension cases, 66.7% of the mild preeclampsia cases and 100% cases of both severe preeclampsia and eclampsia showed prolonged prothrombin time. There was a statistically significant difference between study groups as shown in Table 5 and Figure 5.
Bleeding time (BT)- The Bleeding time was prolonged for more than 5 min in 28.5% of the gestational hypertension patients, 61.1% of the mild preeclampsia patients and 50% of the patients with severe preeclampsia and eclampsia. Results were not statistically significant as shown in Table 6 and Figure 6.
Clotting time (CT) - The clotting time was more than 5 mins in 35.7% of cases of gestational hypertension and was found to be 66.67% of the mild preeclampsia patients and severe preeclampsia patients and 50% of the eclampsia study group. Results were not found to be statistically significant as shown in Table7 and Figure 7.
DISCUSSION -
Hypertensive disorders are the most important cause of perinatal and maternal mortality and morbidity. Cases of Pregnancy-induced hypertension develop a variety of haematological changes with thrombocytopenia being the most common haematological abnormality.
The mean platelet count in our study in normal cases at term pregnancy was found to be 2.85 lakhs/cumm, in the Gestational hypertension study group was 2.01 lakhs/cumm and was 1.81 lakhs/cumm in mild preeclampsia and 1.66 lakhs/cumm in severe eclampsia cases and 1.23 lakhs/cumm in eclampsia group, indicating a significant decrease in mean platelet counts with the increasing grades of pregnancy-induced hypertension cases. Our observations were consistent with the following studies. 22-26
Shete et al.22 studies done in 2013 showed the mean platelet count in normal pregnancy to be 3.41 lakhs/cumm and in severe PIH and Eclampsia cases, it was 1.27 lakhs/cumm with a significant P-value <0.05.
Chauhan et al3 in a 2013 study exhibited the mean platelet count in normal pregnancy was 2.47 lakhs/cumm, in non-severe PIH was 1.62 lakhs/cumm and in severe PIH was 1.63 lakhs/cumm. The P-value was found to be significant (<0.001)
Mohapatra et al.1 exhibited the mean platelet count in normal pregnancy was 2.38 lakhs/cumm, in preeclampsia, it was 1.82 lakhs/cumm, and in the Eclampsia study group, it was found to be 1.21 lakhs/cumm with a P-value of <0.1.
The studies above mentioned correlated well with the present study for the mean platelet count with the significant P-values.
Few studies are done regarding the probability of using Mean Platelet Volume as an adverse outcome indicator in PIH cases and have shown variable results
Mean MPV in the normotensive pregnant females in our study at term was observed to be 8.47 fl (Range of 8-12) and showed an increase in mean values with increasing grades in mean values with the mean of 8.65 fl in gestational hypertension cases and 8.79 fl in mild preeclampsia and 10.33 fl in severe preeclampsia and 9.63 fl in eclampsia cases indicating an increase till severe preeclampsia group but was found to be not significant (p=0.07)
Our study correlated with Ceyhan et al.30 studies who did not find a significant difference in MPV between preeclampsia and the normal pregnant group.
Altibas et al.32 reported an increase in MPV with increasing grades of PIH, but the increase in MPV was not found to be a significant predictor of preeclampsia severity.
Annam et al.25 studied the platelet indices in PIH cases and reported the Mean platelet volume of 10.38 fl in 82 subjects of the preeclampsia subgroup which is comparable to our study.
However further studies with large study populations are required to generalize the MPV findings as an aid in predicting the severity of PIH cases.
Various studies have been done to validate Platelet Distribution width (PDW) as a good marker of platelet dysfunction in Pregnancy-induced hypertension cases with variable results.
In our study, the mean Platelet distribution width (PDW) in normal cases was 10.90 fl and showed an increase with the progression of disease in PIH cases with a value of 11.33 fl in gestational hypertension cases and 11.96 fl in mild preeclampsia and with a mean of 11.7 fl in severe eclampsia cases and 12.25 fl in the eclampsia study group. Although the mean PDW values increased with the increasing grades of PIH it was not found to be statistically significant. 27,28
Bhavna Thakur et al.9 also studied PDW in PIH cases and observed the mean of 13.7fl in Gestational hypertension cases and stated mean of 15.66 fl in preeclampsia cases. In gestational hypertension cases, PDW was found to be non-significant but was found to be significant in the pre-eclampsia group.
The non-significant difference in PDW in the present study correlated well with Dogan et al.29 study which also found a non-significant difference in PDW among women in study groups of severe preeclampsia, mild preeclampsia, and healthy controls. 29
In the present study, the mean prothrombin time of patients with gestational hypertension was 16.59 secs, in mild preeclampsia, it was 17.61 secs and in severe eclampsia it 18.88 secs and in the Eclampsia group it was 15.0 secs. 57.14% of gestational hypertension, 83.33% of mild preeclampsia cases and all cases of severe eclampsia and eclampsia had prolonged prothrombin time with a significant P-value <0.0001. Our study data correlated well with the following statistically significant studies for Prothrombin time.31,32, 33
Similarly, the study by Mushtaque et al.28 studies revealed the mean prothrombin time in three study groups for normal pregnancy, non-severe PIH and severe PIH patients were 10.9 seconds, 10.1 seconds and 9.8 seconds respectively, with a significant P-value less than 0.0001.
Shetty et al.26 studied haematological changes in pregnancy-induced hypertension and observed that 28.57% cases of mild PIH and 82.86% of severe PIH had prolonged PT (>14 s). The PT in severe PIH was found to be significantly prolonged (P < 0.05)
Abdulla et al.10 studied Prothrombin time in 100 PIH cases and found that 50% of cases have prolonged PT with a significant p-value of (0.000) indicating that a highly significant difference in prothrombin time occurs between cases and their control.
In the present study, the mean Activated partial thromboplastin time for normal pregnancy, gestational hypertension and mild preeclampsia and severe eclampsia were 25.76 sec, 33.55 sec, 38.79 sec and 41.85 sec respectively with Eclampsia group showed it to be 40.17 secs, with a significant P-value <0.0001 indicating an increase in APTT levels with increasing severity of PIH.
Study done by Mushtaque et al.28 revealed the mean activated partial thromboplastin time for normal pregnancy, non-severe PIH and severe PIH patients were 26.68 seconds, seconds 26.71 and 26.25 seconds respectively, with P value less than 0.005 was statistically significant. The present study correlated well with our study.
Nirmala et al.13 in their study showed that the mean activated partial thromboplastin time among the patients with mild Gestational Hypertension was 25.11 secs, severe GH was 25.97 secs, Mild preeclampsia cases was 26.74 secs and in severe preeclampsia, cases was 27.33 secs.
Bleeding time in mild preeclampsia cases the majority of 61.11% of cases showed an increase towards the upper limit of the normal with 50% of the cases showed an increase in BT in severe preeclampsia and eclampsia study groups, although the BT levels showed an increase in levels towards increasing grade of hypertension the results were found to be statistically insignificant.30
Our study results were similar to the study by Chaware et al.16 which showed that the bleeding time in mild preeclampsia was 1.93 secs and it was found to be 2.02 secs in the severe preeclampsia group and the values observed were not found to be significantly increased.
Our study results were consistent with Chavan et al.12 studies which showed that the bleeding time in mild preeclampsia was 2.45 secs and it was found to be 2.66 secs in the severe preeclampsia group and the values observed were found to be not statistically significant.
Our study was consistent with Sonal et al.6 study which observed that the bleeding time was found to be more than 5 min in 38.1% of gestational hypertension patients, 58.1% of the preeclampsia cases and 80% of cases with eclampsia but the results were not found to be statistically significant.
Clotting time - In gestational hypertension study groups the majority of cases 64.29% showed the normal bleeding time of below 5 mins but in both mild and severe preeclampsia cases study groups the majority of 66.67% of cases showed an increase towards the upper limit of the normal with 50% of Eclampsia cases showed an increase in clotting time, although the Clotting time levels showed an increase in levels towards increasing grade of hypertension the results were found to be statistically insignificant.
Our study results were similar to the study by Chaware et al.16 which showed that the clotting time in mild preeclampsia was 4.20 secs and they observed it to be 4.25 secs in the severe preeclampsia group and the values observed were not found to be significantly increased.
Anjali et al.22 also showed in their study that clotting time was observed to be 6.74 min normal cases and 4.07 min in Pregnancy-induced hypertension cases and the observed values were found to be not statistically significant change.
Significant prolongation of Prothrombin Time, activated partial thromboplastin time and significant fall in platelet counts was observed in PIH study groups indicating derangements in platelet counts and coagulation cascade with increasing grades of pregnancy induced hypertension study groups.7,8,9
CONCLUSION -
• Platelet counts showed an inverse relationship with the increasing severity of pregnancy-induced hypertension.
• Prothrombin time and Activated Partial Thromboplastin time showed prolonged values with increasing grades of pregnancy-induced hypertension.
• Data observed from the present study can help identify the abnormalities in platelet parameters and coagulation profile about pregnancy-induced hypertension cases at an earlier stage and can prove to be helpful in the management of complications associated with pregnancy-induced hypertension, thus can help in the reduction of maternal and fetal mortality.
Further studies with large sample size and serial assessment of coagulation parameters are required to corroborate these findings and their relationship with the progression and severity of PIH.
ACKNOWLEDGEMENT - Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of funding: None
Conflicts of interest: None
References:
-
Mohapatra S, Pradhan BB, Satpathy UK, Mohanty A, Pattnaik JR. Platelet estimation: Its prognostic in pregnancy induced hypertension. Ind J Phy Phar. 2007;51:160-4.
-
Meshram DP, Chavan YH, Kadam PN, Panchal MG, Ramteke DJ. Maternal and foetal outcomes in pregnancy induced hypertension -A hospital based study. Int J Phar Sci Invention. 2014;3:23-6.
-
Chauhan P, Rawat U, Bisht V, Purohit RC. Comparison of coagulation profile in pre-eclamptic and eclamptic patients with normotensive pregnant patients. J Evol Med Dent Sci. 2014;3:3208-15.
-
Veena HC, Manjunatha S, Itagi V, Taklikar RH, Patil RS. The hemostatic mechanisms in PIH. Indian J Appl Basic Med Sci. 2015;17:40-4.
-
Leduc L, Wheeler JM, Kirshon B, Mitchell P, Cotton DB. Coagulation profile in severe preeclampsia. Obstet Gynecol. 1992;79:14-8.
-
Sonal, Mathur S. The Coagulation Profile on Pregnancy Induced Hypertensive Patients in Third Trimester of Pregnancy – The Prospective and Observational Study. Ann. Int. Med. Den. Res. 2018;4(4): OG01-7.
-
Say L, Chou D, Gemmill A, Tunçalp Ö, Moller AB, Daniels J, Gülmezoglu AM, Temmerman M, Alkema L. Global causes of maternal death: a WHO systematic analysis. The Lancet Glob Heal. 2014;2(6):e323-33.
-
National health portal [Internet].Preeclampsia [ UPDATED 2016 June 01;cited 2016 june01]. Available at https://www.nhp.gov.in/disease/gynaecology-and-obstetrics/preeclampsia
-
Thakur B, Kulkarni V, Thakur . Platelet indices in PIH.J Cont Med A Dent. 2016;4(3):20-6.
-
Abdulla HAB. The Effects of Pregnancy Induced Hypertension on PT and APTT among Sudanese Pregnant Women Attending to Wad Madani Maternity Teaching Hospital - Gezira State Sch. J. App. Med. Sci. 2017;5(10D):4094-7
-
Agarwal S, Buradkar S. Coagulation studies in toxaemia of pregnancy. J Obstet Gynaecol Ind. 1978; 27:992-6.
-
Chavan SS, Patil SL.Study of role of thrombocytopenia in predicting severity of Preeclampsia. Medpulse-Int Med J. 2015;2(9):557-9
-
Nirmala T, Kumar PL, Vani BR, Murthy SV, Geetha RL. Study of coagulation profile in pregnancy-induced hypertension (PIH). Indian J Pathol and Oncol. 2015;2(1):1-6
-
Sultana F, Partibhan R, Shariff S. Thrombocytopenia in Pregnancy Induced Hypertension. J Med Sci Health. 2015;1(2):19-24.
-
Sharma UK, Kouli R, Sonowal R, Saikia P. Coagulation parameters in pre-eclamptic and eclamptic patients - A comparative study of 90 cases. Int J Contemp Med Res. 2016;3(8):2235-8
-
Chaware SA, Birare SD, Naigaonkar NV, Mahule SK. Comparative study of coagulation profile in Pre-Eclamptic and Eclamptic Patients with normotensive pregnant patients:2 Year Study. Int J Contemp Med Res. 2017;6(2):445-9
-
Vinodhini R, Kumari L. Evaluation of platelet count as a prognostic index in eclampsia and pre-eclampsia. Int J Mod Res Rev. 2014;2(10):447-52.
-
Sameer MA, Meshram DP, Deshpande SA, Sadhu D, Pandit S. Role of platelet count as important prognostic marker in pregnancy induced hypertension. IOSR J Dent Med Sci. 2014;13:39-43.
-
Mohapatra D, Priyadarsini N, Behera M, Panda P, Mishra T. Hematological parameters in the assessment of pregnancy induced hypertension. Int J Pharm Bio Sci. 2015;6:854-9.
-
Akhila NR, Jayalakshmi L, Devi K. Study of mean platelet volume in gestational hypertension and normal pregnancy. Int J Biomed Res. 2015;6(6):366-9.
-
Shah AR, Chaudhari SN, Shah MH. Role of platelet parameters in diagnosing various clinical conditions. Natl J Med Res. 2013;3:162-5.
-
Anjali NS, Garkal KD, Deshmukh PR. Physiological parameters in pregnancy induced hypertension. Int J Recent Trends Sci Techn. 2013;7:24-5.
-
Rupakala BM et al. Hypertensive disorders of pregnancy cases Int J Reprod Contracept Obstet Gynecol. 2018;7(3):848-54
-
Mishra DP, Choudhury S, Tudu B. Evaluation of coagulation indices in preeclampsia and eclampsia. J. Evid. Based Med. Healthc. 2019;6(17):1316-20
-
Annam V, Srinivasa K, Yatnatti SK, Suresh DR. Evaluation of platelet indices and platelet counts and their significance in preeclampsia and eclampsia. Int J Biol Med Res. 2011:2(1):425-28.
-
Shetty J, Rao S, Kulkarni MH. Hematological Changes in Pregnancy-induced Hypertension. Int J Sci Stud. 2016;4(5):216-21.
-
Sameer MA, Meshram DP, Deshpande SA, Sadhu D, Pandit S. Role of platelet count as an important prognostic marker in pregnancy-induced hypertension. IOSR J Dent Med Sci. 2014;13:39-43.
-
Mushtaque T. A comparative study of coagulation profile in term normal pregnancy, preeclampsia and eclampsia (doctoral dissertation).Available at http://localhost:8080/xmlui/handle/123456789/8903
-
Do?an K, Guraslan H, Senturk MB, Helvacioglu C, ?dil S, Ekin M. Canplatelet count and platelet indices predict the risk and the prognosis of preeclampsia. Hypertens Pregnancy. 2015;34(4):434–42.
-
Ceyhan T, Beyan C, Baser I, Kaptan K, Gungor S, Ifran A(2006). The effect of preeclampsia on complete blood count, platelet count and mean platelet volume. Ann Hematol. 2006;85:320–2.
-
Mishra DP, Choudhury S, Tudu B. Evaluation of coagulation indices in preeclampsia and eclampsia. J. Evid. Based Med. Healthc. 2019;6(17):1316-20.
-
Bhutani K, Vij C, Kaur M, Bedi GK. Pregnancy Induced Hypertension: A Study on Its Multisystem Involvement. Int J Cur Res Rev 2018;10(9):27.
-
National Ethical Guidelines by ICMR on biomedical research 2017, chapter 5, Informed consent process Box 5.2 (Conditions for granting a waiver of consent).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





