IJCRR - 13(13), July, 2021
Pages: 210-217
Date of Publication: 05-Jul-2021
Print Article
Download XML Download PDF
Effects of Early Ambulation in Post Operative Recovery Among Women with Abdominal Hysterectomy
Author: Amruta Taksande, Manjusha Mahakalkar, Vaishali Taksande
Category: Healthcare
Abstract:Background: Amazed all hysterectomy, most frequently performed surgical procedures in women is abdominal hysterectomy. If early ambulation is not done post operatively, there is chance of different complications such as eruption, deficient veins, lowers respiratory tract infection, minor bleeding and venous thrombo-embolism, blockage of pulmonary artery, paraplegic ileum and etcetera. Objectives: 1) To assess post operative recovery among the women who have undergone abdominal hysterectomy in control group.2) To assess the effectiveness of early ambulation in post operative among the women who have undergone abdominal hysterectomy in experimental group. 3) To compare post-operative recovery among the women who have undergone abdominal hysterectomy in control and experimental group. Methods and Materials: A quantitative research approach was used in this study with quasi-experimental group study research design and sample size was 100 were selected by a Non-Probability Purposive Sampling Technique. An observational checklist and post-operative related questionnaire was used to collect the data. Results: In experimental group, duration of post operative recovery among women who has undergone abdominal hysterectomy is less as compared to post-operative recovery among women who has undergone abdominal hysterectomy in control group. Also structured questionnaire related to post-operative recovery interpret that early ambulation is effective one in experimental group as compared to in control group. Conclusion: Early ambulation is effective and helps to recover soon.
Keywords: Early ambulation, Post operative recovery, Abdominal hysterectomy, Abdominal surgery, Gynecological operations
Full Text:
INTRODUCTION
Typically a gynecologist performs hysterectomy, which is a cut-out or surgical removal of the vagina. Hysterectomy may be complete body removal, known as total hysterectomy or fundus, and cervix uterine; sometimes referred to as partial removal of uterine body known as partial hysterectomy while keeping the cervix intact, known as supra cervical hysterectomy. It is the most frequently performed surgical procedure. More than 600,000 hysterectomies have been conducted in 2003.1,7 In favorable cases, more than 90 % of these procedures are conducted in the US alone. Such high rates in industrialized world have led major controversy that hysterectomies are performed largely for unwarranted and unnecessary reasons.2,3
As a last resort to cure such intractable uterine/reproductive system problems, hysterectomy is usually recommended. These disorders may include uterine fibroids, extreme intractable endometriosis, adenomyosis, chronic pelvic pain, frequent obstetric hemorrhage, and various forms of vaginal prolapse, and sometimes serious pre-placenta and placenta accrete.3,4,5
MATERIALS AND METHODS
The study was based on a quantitative research approach with a quasi-experimental group study research design. A Non-Probability purposive sampling technique was used and 100 samples of women from selected hospitals. Inclusion criteria were women between ages of 20 and 50 years and older and women who want to take part in this study. Exclusion criteria were women who are not available at the time of study and women who are having post abdominal hysterectomy complications. Tools were an observational checklist and post-operative related questionnaire. The data gathering process began from 12th Aug to 31st Aug 2019. The investigator visited the area in advance and obtained the necessary permission from the concerned authorities. The institutional Ethics Committee in its meeting held on 12/12/2018 has approved the study and the Referral number is 7758. Based on the objectives and the hypothesis the data were analyzed by using various statistical tests. In control group, early ambulation is not suggested while in experimental group, early ambulation is suggested and checklist is assessed after 5-6 days of early ambulation.
RESULTS
Section 1
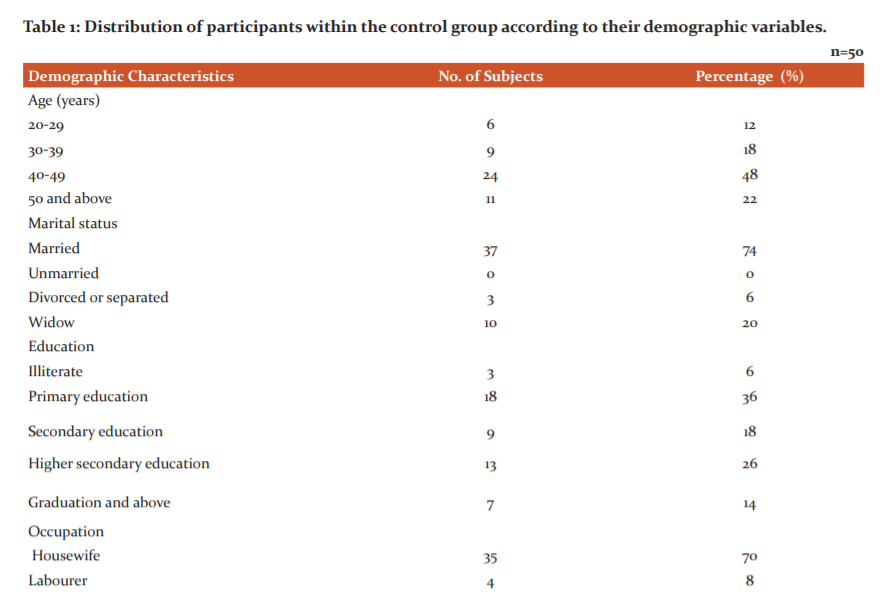
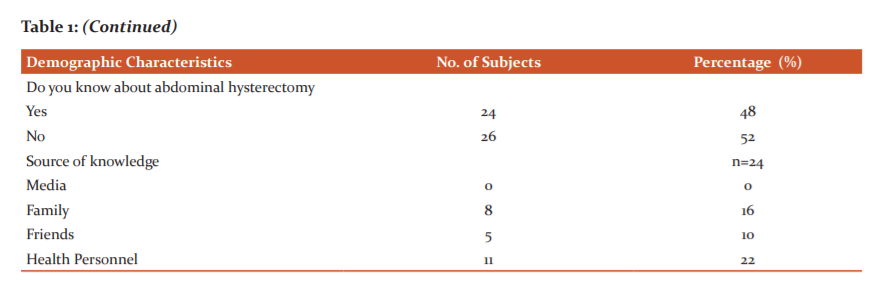
Part I – Distribution of participants within the control group according to their demographic variables.
Table no 1 Shows that, 6(12%) of 20-29yrs age, 9(18%) 30-39years old, 24(48%) 40-49yrs, 11(22%)50 yrs & above. 37(74%) married, no subjects unmarried, 3(6%) divorced or separated, 10(20%) widow. 3(6%) illiterate, 18(36%) had primary education, 9(18%) had secondary education, 13(26%)higher secondary & 7(14%) graduated & above. 35(70%) housewife, 4(8%) laborer, 6(12%) business women, 1(2%) on government job, 4(8%) on private job.24(48%) knew & 26(52%) didn’t know about abdominal hysterectomy, in 8(16%) source of knowledge was family, in 5(10%) it was friends, in 11(22%) source of knowledge was health personnel.
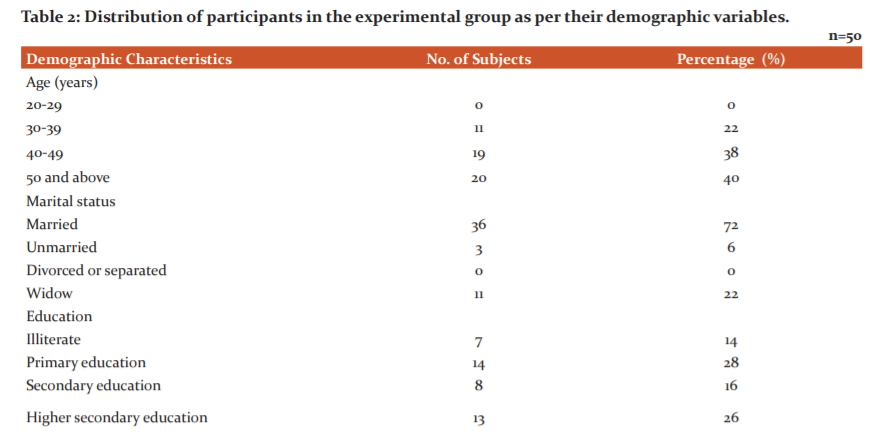
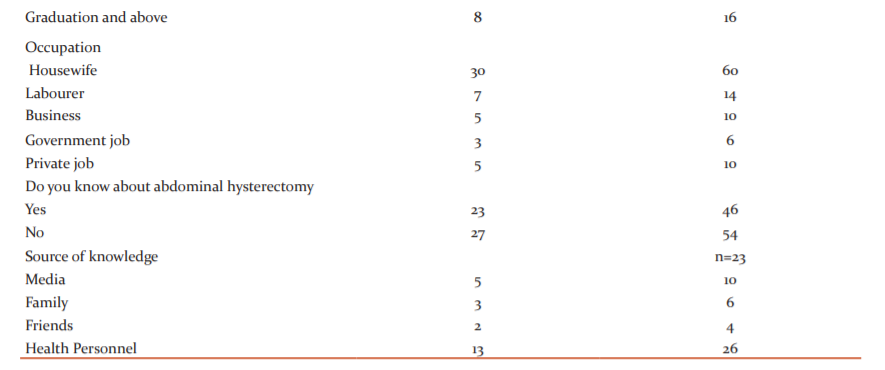
Part II – Distribution of participants in the experimental group as per their demographic variables.
Table no 2: No subjects were of 20-29 year age group, 11(22 %) were of 30-39 yrs, 19(38 %) 40-49 yrs age, 20(40%) were 50 yr-old & above. 36(72%) married, 3(6%) single, none divorced or separated, 11(22%) were widow. 7(14%) were illiterate,14(28%) primary education, 8(16%) secondary education, 13(26%) higher secondary, 8(16%) is graduated & above. 30(60%) housewife, 7(14%) labourer, 5(10%) business women, 3(6%) on government job and 5(10%) on private job.23(46%) subjects knew whereas 27(54%) did not know about abdominal hysterectomy, in 5(10%) source of knowledge was media, in 3(6%) it was family, in 2(4%) it was friends, in 13(26%) source of knowledge was health personnel.
Section 2
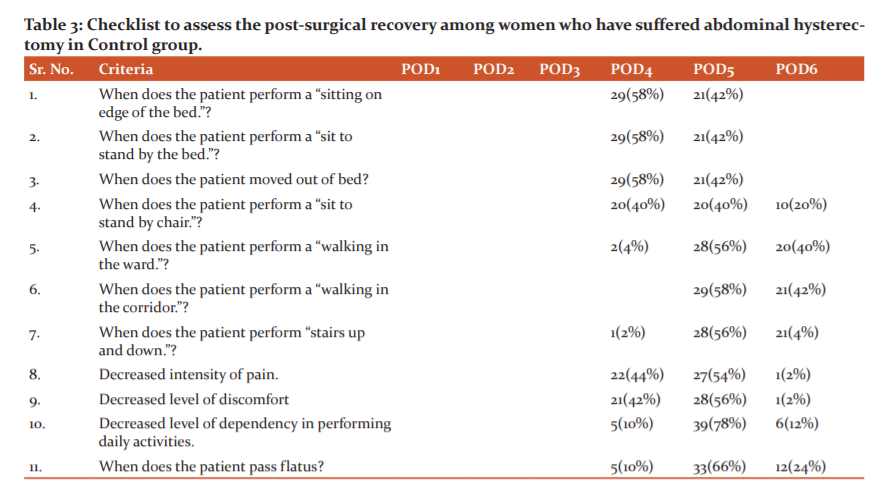
Part I – Checklist to assess the post-surgical recovery among women who have suffered abdominal hysterectomy in Control group.
Table no. 3 contain 29(58%) On day 4 & 21(42%) women on 5th day rest on bed's edge.
29(58%) on 4th day & 21(42%) were sitting on bed on POD5.
29(58%) on the 4th day & 21(42%) moved out of bed on POD5.
20(40%) on day 4 , 20(40%)on 5th & 10(20%) were sitting in chair on 6th day.
2(4%) on day 4, 28(56%) on POD5, 20(40%) walk in ward on day 6th day.
29(58%) on day 5, 21(42%) on POD6 perform walk in ward.
1(2%) on POD 4, 28(56%) on day 5 & 21(42%) on POD 6 perform stairs up & down.
22(44%) on day 4, 27(54%) on day 5 & 1(2%) felt decreased intensity of pain on POD6.
21(42%) on day 4, 28(56%) on POD 5 and 1(2%) on POD6 felt decreased level of discomfort.
5(10%) on day 4, 39(78%) on day 5 and 6(12%) on POD6 felt decreased level of dependency in performing daily activities.
5(10%) on day 4, 33(66%) on day 5, 12(24%)on POD6 passed flatus.
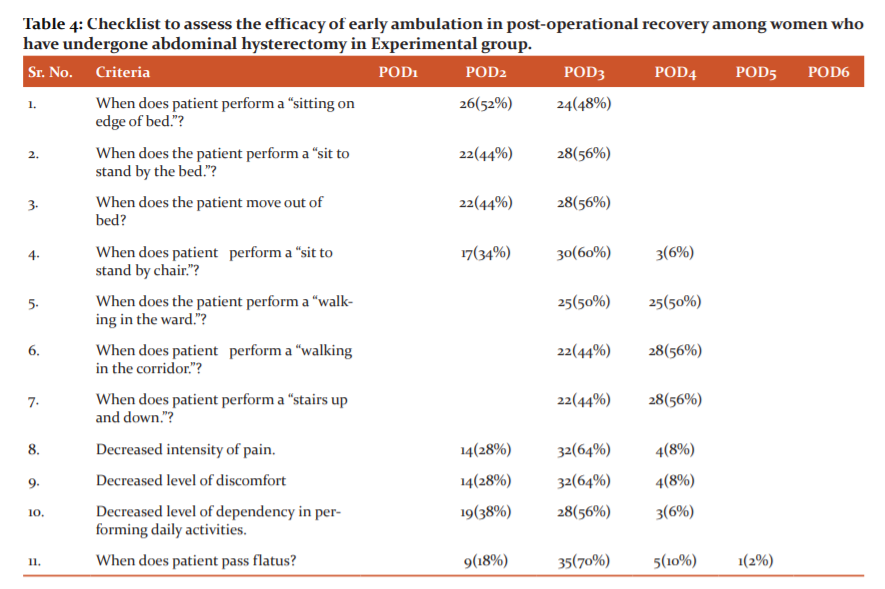
Part II – Checklist to assess the efficacy of early ambulation in post-operational recovery among women who have undergone abdominal hysterectomy in Experimental group.
Table no. 4 shows the following data
26(52%) on POD2 while 24(48%) sat on bed’s edge on POD3.
22(44%) on POD2, 28(56%) were sitting in bed on POD3.
22(44%) on POD2, while 28(56%) women shifted out of bed on day 3.
17(34%) on day 2, 30(60%) women on day 3, 3(6%) on day 4 were sitting at chair.
25(50%) on day 3, 25(50%) women walk in ward on POD 4.
22(44%) on POD 3, 28(56%) on POD4 perform walking in corridor.
22(44%) on POD 3, 28(56%) women on day 4 perform stairs up and down.
14(28%) on POD2, 32(64%) on POD 3, 4(8%) on day 4 felt decreased intensity of pain.
14(28%) on day 2, 32(64%) on day 3, 4(8%) on day 4 felt decreased level of discomfort.
19(38%) on day 2, 28(56%) on day 3 and 3(6%) on day 4 felt decreased level of dependency in performing daily activities.
9(18%) on day2, 35(70%) on day 3, 5(10%) on day 4 and 1(2%) women on day 5 passed flatus.
Section 3
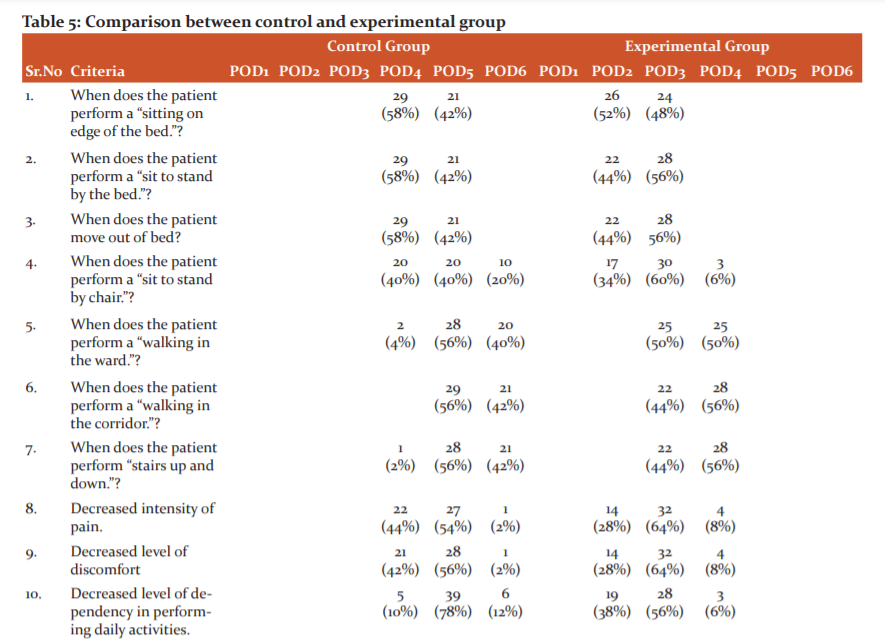
Table no. 5 shows a Comparison between the control and experimental group
In control group, 29(58%) on 4th day, 21(42%) on 5th day while in experimental group, 26(52%) on 2nd day & 24(48%) women on 3rd day perform a sitting on edge of bed.
In control group, 29(58%) on 4th day, 21(42%) on 5th day wherein among experimental group, 22(44%) on 2nd day, 28(56%) subjects on 3rd day perform a sit to stand by bed.
29(58%) on 4th day 21(42%) on 5th day, in control group, 22(44%) on 2nd day, 28(56%) women on 3rd day in experimental group moved out of bed.
In the control group, 20(40%) on the 4th day, 20(40%) on the 5th day, 10(20%) on the 6th day whereas in the experimental group, 17(34%) on the 2nd day, 30(60%) on the 3rd day 3(6%) subjects on 4th day sat to stand by the chair
2(4%) women on 4th day, 28(56%) on 5th day, 20(40%) on 6th day in the control group whereas 25(50%) on 3rd day, 25(50%) women on 4th day in the experimental group performed walking in the ward.
In control group, 29(56%) subjects on 5th day, 21(42%) on 6th day while in experimental group, 22(44%) on 3rd day, 28(56%) on 4th day performed walking in corridor.
1(2%) on 4th day, 28(56%) on 5th day 21(42%) on 6th day in control group while 22(44%) on 3rd day, 28(56%) on 4th day in experimental group performed stairs up and down.
In the control group, 22(44%) on the 4th day, 27(54%) on the 5th day 1(2%) on the 6th day whereas in the experimental group, 14(28%) on the 2nd day, 32(64%) on 3rd day, 4(8%) women on 4th day had decreased intensity of pain.
21(42%) on 4th day, 28(56%) on 5th day 1(2%) on 6th day in control group and 14(28%) on 2nd day, 32(64%) on 3rd day, 4(8%) subjects on 4th day felt decreased level of discomfort.
In the control group, 5(10%) on the 4th day 39(78%) on the 5th day, 6(12%) on the 6th day wherein in the experimental group, 19(38%) on the 2nd day, 28(56%) on 3rd day, 3(6%) women on 4th day had decreased level of dependency in performing daily activities.
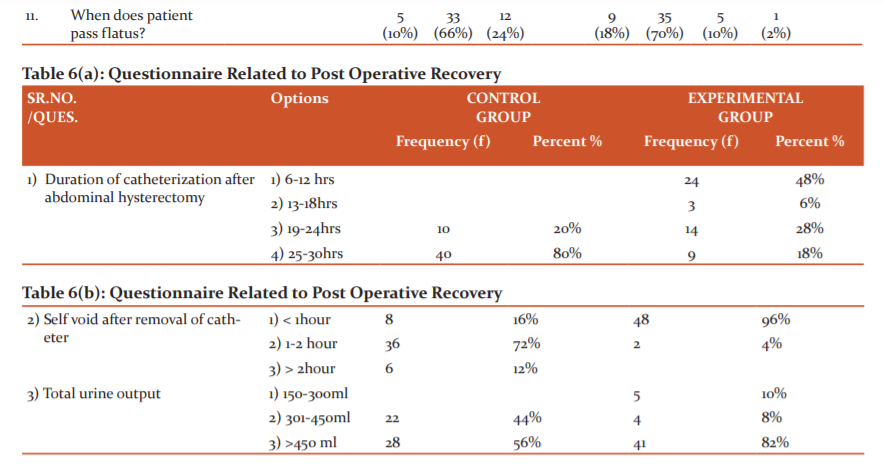
5(10%) on 3rd day, 33(66%) on 4th day, 12(24%) on 6th day in the control group whereas 9(18%) on 2nd day, 35(70%) on 3rd day, 5(10%) on 4th day 1(2%) subjects on 5th day in the experimental group passed flatus.
Section 4-
Structured questionnaire related post-operative recovery in the control and experimental group and comparison between them.
Table no. 6(a) having information about control group, duration of catheterization was 19-24hrs in 10 (20%) and 25-30 hrs in 40 (80%). In experimental group, it was 6-12hrs in 24(48%), 13-18hrs in 3(6%), 19-24hrs in 14(28%) and 25-30 hrs in 9(18%) women.
Table no.6(b) shows, control group, 8(16%) self void <1hr, 36(72%) between 1-2hr and 6(12%) self void>2hr however, in experimental group, 48(96%) women self void in <1hr, 2(4%)1-2 hr after removal of catheter.
In control group, 22(44%) women were having 301-450 ml & 28(56%) having >450 ml urine output. In experimental group, 5(10%) having 150-300 ml,4(8%) having 301- 450ml and 41(82%) having >450 ml urine output.
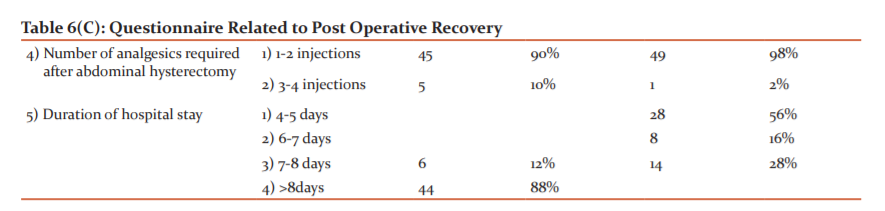
Table no. 6(c) having the information,In control group, 45(90%) 1-2 analgesic, 5(10%) required 3-4 analgesics & in experimental group, 49(98%) 1-2, 1(2%) required 3-4 analgesics after hysterectomy.
In the control group, 6(12%) for 7-8 days, 44(88%) for >8 days while in the experimental group, 28(56%) for 4-5 days, 8(16%) for 6-7 days and 14(28%) women for 7-8 days stays in the hospital.
DISCUSSION
Similar study was conducted which was eventual adherent study in which amide 50 patients who had undergone abdominal hysterectomy from June 1, 2003 to December 31, 2003. Study aimed to discover early activity's security and viability. The study concluded that in patients with hysterectomy, the early operation is possible and healthy. After 2 days of ambulation, most of the clients (78%) were able to ambulate 100feet.4,5,6
This study shows that, in experimental group, duration of post operative recovery among women is less as compared to post-operative recovery among women who has undergone abdominal hysterectomy in control group. Also structured questionnaire related to post-operative recovery interpret that early ambulation is effective one in experimental group as compared to in control group in which only post-operative recovery checked and early ambulation not suggested.7,8,9
CONCLUSION
Therefore, healthcare providers at all levels need to understand the importance of early ambulation after abdominal hysterectomy, become educated on the protocols and procedures of practice in order to make early ambulation on day zero new standard of care for all postoperative patients. Conflict of interest is nil and the source of funding was self. Early ambulation improved the state and aids in early discharge.
ACKNOWLEDGEMENT
We would like to thank all the participants and the authorities of the institutions for their cooperation throughout the data collection.
Conflict of Interest : None
Source of Funding: None

References:
1.Pinar G, Okdem S, Dogan N, Buyukgonenc L, et al. The Effects of hysterectomy on Body Image, self esteem and Martial adjustment in Turkish women with Gynaecologic cancer. Clin J Onc Nur. 2012; 16(3):99-104.
2. Elizabeth A Stewart, Wanda K Nicholson, et al. The burden of uterine fibroids for American-American women: results of a national survey. J Wom Hea.
2013:22(10); 807-816.
3. Daniel Morgan, Across the country, fewer women are getting hysterectomies and those who do are choosing less invasive methods with no hospital stays, saving millions in health care costs. Inst Health Pol Inn. 2018;23 (9): 142-145.
4. Earnest VV. Procedure Checklist to Accompany Caroline Bunker Rosdahl's Textbook of Basic Nursing. Lippincott; 1999; 142-145.
5. Priya SP, Roach EJ, Lobo DJ. Effectiveness of pre-operative instruction on knowledge, pain, and selected post-operative behaviours among women undergoing abdominal hysterectomy in selected hospital, Bangalore, Karnataka. Man J Nur Hea Sci. 2017; 3(1):3-9.
6. Katz A. Sexuality after hysterectomy. J Obst Gynec Neon Nur. 2002 May; 31(3):256-62.
7. Banos Calbo M. Enhanced Recovery Programme in Abdominal Surgery. J Obst Gynec NeonNur.2018:30(4): 875-879.
8. Behjati AZ. An Evaluation of the Historical Importance of Fertility and Its Reflection in Ancient Mythology. Avic Res Insti. 2016; 17(1): 2-9.
9. Chaudhari S. Psychiatric effects of Hysterectomy. J Adv Res. 1995; January; 51(1): 27–30.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





