IJCRR - 13(13), July, 2021
Pages: 205-209
Date of Publication: 05-Jul-2021
Print Article
Download XML Download PDF
Endodontic Revascularization of Necrotic Permanent Anterior Tooth with Platelet Rich Fibrin, Platelet Rich Plasma, and Blood Clot - A Comparative Study
Author: Suvarna Sunder J, Seema Abid Hussain, Ullah Tareen Sabahat, Prabu Mahin Syed Ismail, Shetty Akhil, Patel Pawan
Category: Healthcare
Abstract:Introduction: Treatment of necrotic tooth requires extensive management due to chances of fracture. Revascularization is the procedure for the management of immature necrotic tooth. Aim: The study was done to assess endodontic revascularization of the necrotic permanent anterior tooth with Platelet Rich Fibrin (PRF), Platelet Rich Plasma(PRP), and blood clot. Materials & Methods: Thirty patients within the age range 15-25 years with the non-vital maxillary anterior tooth with or without periapical pathology and immature apex were selected and subjected to revascularization endodontics PRF, PRP and blood clot. Healing, root lengthening, apical closure and dentinal wall thickness was determined. Results: Group I used PRF, group II used PRP plus collagen and group III used blood clot. Group I had 6 males and 4 females, group II had 5 males and 5 females and group III had 4 males and 6 females. There was excellent healing seen in 80% in group I, 30% in group II and 10% in group III. Mann Whitney U test showed a significant difference (P 0.05) Conclusion: It was concluded from the present study that PRP had superior result in terms of apical closure, root lengthening and dentine wall thickness compared to the blood clot and PRF.
Keywords: Apical closure, Endodontics, Necrotic teeth, PRP, Revascularization
Full Text:
Introduction
Treatment of necrotic tooth requires extensive management since chances of fracture through small roots as well as thin dentinal walls is more.1 The most commonly employed procedure for the closure of immature root apex is apexification. Stem cells are totipotent cells that help in the proliferation and production of cells, capable of differentiating into specialized cells.2
Adult stem cells and embryonic stem cells are two types of stem cells that help in pulp revascularization. The common site of their occurrence is pulp, apical papilla and periodontal ligament.3 These clonogenic cells induce dentin-pulp regeneration after they get differentiated into appropriate cells. Development of a complete tooth from a stem cell will be possible in the future. Stem cells after differentiating odontoblasts induce hard tissue apposition.4
Revascularization is the procedure for the immature necrotic tooth. It helps in the completion of root formation of the immature necrotic tooth.5 Most commonly used material for it is mineral trioxide aggregate (MTA) and calcium hydroxide (Ca (OH)2). The results of the treatment lead to the fracturing of teeth in 30% of cases. Hence there is a shift in the management of immature necrotic teeth.6
The formation of a functional pulp-dentin complex is regarded as a substitute method to exchange the conventional apexification method to initiate root formation and dentinal walls thickening in the case of the immature non-vital tooth.7 Recent studies showed blood clot as a material in regenerative endodontics which acts as scaffold leading to enhance the concentration of growth micromolecules.8 Platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) both comprise of increased concentration of growth factors and increase the cell proliferation over time when compared to the blood clot.9 The present study aimed at assessing endodontic revascularization of necrotic permanent anterior with PRF, PRP and blood clot.
Methodology
Study design
Thirty patients within the age range 15-25 years of either gender were selected among those reporting to the Endodontic department. Inclusion criteria were non-vital maxillary anterior tooth due to either trauma or caries, a tooth with or without periapical pathology and immature apex. Exclusion criteria were patients beyond the age group, a tooth with mature apex.
The sample was decided based on significance level: 0.05, power: 80% and the number of immature teeth as 30. The study commenced with approval from higher authorities and written consent from selected patients.
Methods
In all patients’ teeth were carefully examined clinically by an Endodontist. All procedures such as pulp vitality test, palpation, percussion test, depth of clinical pocket and occurrence of sinus were performed. Radiographic analysis with digital intra-oral radiographs was performed such as the presence of radiographic bone loss, widening of periapical pathology etc.
All strict asepsis was procedures such as isolation of tooth, access cavity formation, working length determination, biomechanical preparation, irrigation with sodium hypochlorite (NaOCl) was performed. Canals were dried using sterile paper points followed by the use of triple antibiotic dressing paste to medicate the canals.
Over root canal medicament, the cotton pellet was inserted followed by insertion of temporary filling material, Cavit. Over it, glass ionomer cement (GIC) was placed and patients were recalled after 2 weeks. On recall visit, if the tooth found to be asymptomatic, Cavit was removed. Triple antibiotic dressing paste was removed with the irrigation of 2.5% sodium hypochlorite and saline. Following this, three groups were made based on the material used. In group I, PRF clot as the scaffold was used, in group II, PRP plus collagen as the scaffold was used which was pushed towards the apical area and in group III, a blood clot was used. Bleeding at the apical end was induced with a 20K- file. After seeing frank bleeding in the canal, a tight cotton pellet was introduced in the coronal portion of the canal and pulp chamber for about10 minutes to induce the clot formation in the apical two-thirds of the root canal. Patients were recalled at regular intervals on 6, 12 and 24 months to assess tooth clinically and radiographically. Signs of healing, apical closure, increase in root length and dentinal wall thickness was recorded.
Statistical analysis
Results of the study were expressed as percentages. Mann Whitney U test was applied for the assessment. The significance of the study was labelled at 0.05, highly significant at 0.01.
Results
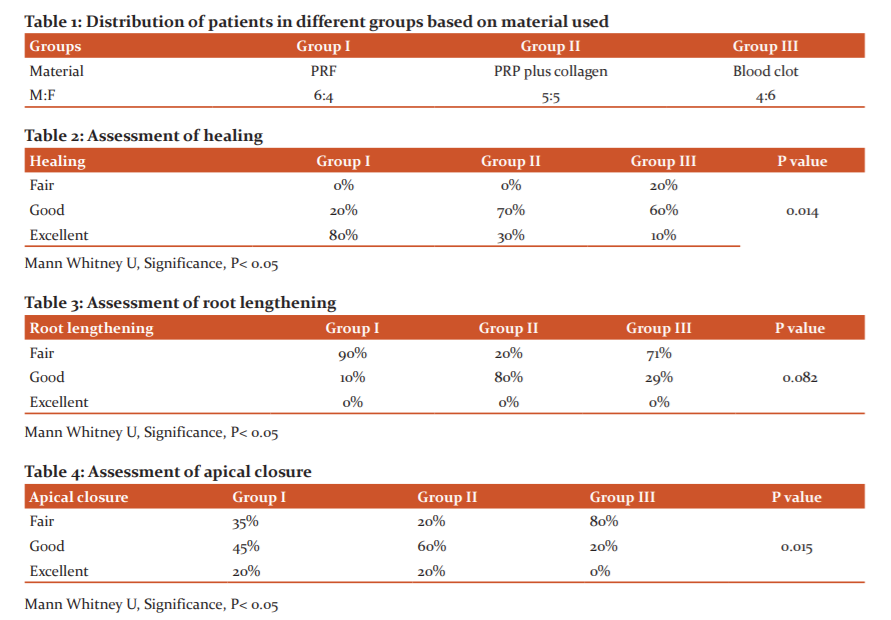
Table 1 shows that group I used PRF, group II used PRP plus collagen and group III used blood clot. Group I had 6 males and 4 females, group II had 5 males and 5 females and group III had 4 males and 6 females.
Table 2 indicates, assessment of healing after revascularization. Group II (PRP) had 70% good, 30% excellent healing, whereas Group III (blood clot) group had 60% good, 10% excellent healing. Group, I (PRF) had 80% excellent healing compared to other groups. Table-3 indicates the outcome of root lengthening. Group II had good (80%) root lengthening compared to Group III (29%) and Group I (10%).
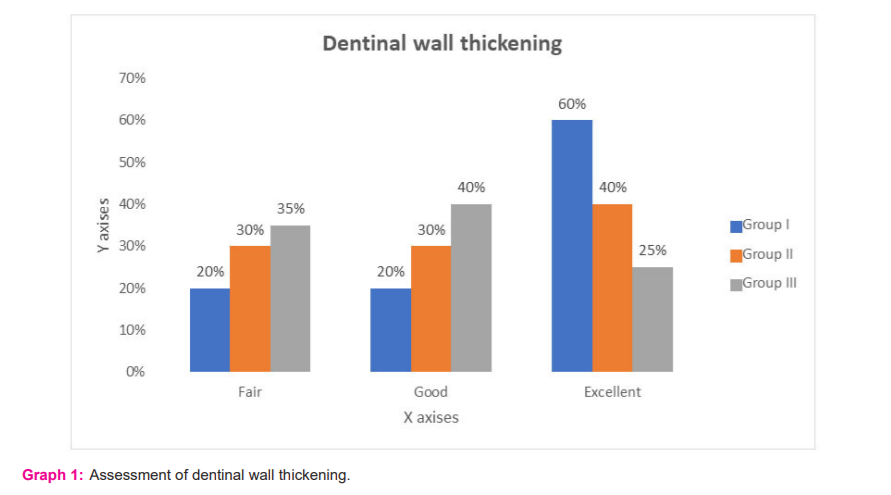
Apical closure found to be good in 45% and excellent in 20% in group I, good in 60% and excellent in 20% in group II and good in 20% and fair in 80% in group III. Mann Whitney U test showed a significant difference (P<0.05) (Table 4). Dentinal wall thickening was fair in 35%, good in 40% and excellent in 60% in group I, 40% in group II and 25% in group III. It was good in 20%, 30% and 40% in group I, II and III respectively with a non-significant difference (P> 0.05) (Graph 1).
Discussion
Regenerative Endodontics is a widely used treatment option nowadays. Dentinal wall thickening and root lengthening are extensively seen with it as compared to apexification.10 The occurrence of sufficient occlusal seal is possible with it, helping in inhibition of re- infection.11 Immature non-vital maxillary anterior tooth is not suitable for endodontic therapy due to its thin dentinal walls.12 PRF offers superior results in terms of apical closure and root lengthening. Revascularization of immature, necrotic maxillary anterior teeth proved to be beneficial for the regeneration of apical tissue to initiate apexogenesis.13 A study by Windley et al.,14 assessed the usefulness of antibiotic paste in the disinfection of immature dog teeth with apical periodontitis. It was ascertained that disinfection of canal, insertion of scaffold matrix for permitting tissue growth and effective coronal seal against micro-organism can be the deciding pints in endodontic revascularization of necrotic immature teeth. This is a novel procedure in endodontics.8 In the present study, we attempted to assess endodontic revascularization of necrotic permanent anterior with PRF, PRP and blood clot.
In this study, we enrolled 30 teeth which had 18 males and 12 females. age group 15-25 years comprised of 10 males and 7 females and 20-25 years had 8 males and 5 females. Group I used PRF, group II used PRP plus collagen and group III used blood clot. Group I had 6 males and 4 females, group II had 5 males and 5 females and group III had 4 males and 6 females. Rizk et al.,15 conducted a study on 30 patients for determining pulp revascularization process in maxillary necrotic permanent immature central incisors in which group I was treated with PRP and group II with PRF scaffolds. Results showed significant improvement in the increase in bone density and reduction in apical diameter. PRP found to be an alternative to PRF in the revascularization process.
We found that excellent healing was seen in 80% in group I, 30% in group II and 10% in group III. This can be explained by the fact that the PRF serves as a matrix onto which vital cells from the peri-apical is seeded to re-establish pulp vascularity.16
In this study it was observed that apical closure found to be good in 45% and excellent in 20% in group I, good in 60% and excellent in 20% in group II and good in 20% and fair in 80% in group III. The concept of revascularization has been explained by numerous researchers. It is hypothesized that at the apical end of the root canal, a small amount of vital pulp tissue containing dental pulp stem cells (DPSCs) remains which retain tissue regeneration potential and can multiply into the newly formed blood clot matrix. It tends to differentiate into odontoblasts and deposits tertiary or tubular dentin.17
We observed that dentinal wall thickening was fair in 35%, good in 40% and excellent in 60% in group I, 40% in group II and 25% in group III. It was good in 20%, 30% and 40% in group I, II and III. The revascularization procedure is possible due to the presence of stem cells in the apical papilla of incompletely developed teeth.18 The presence of collateral circulation at the apical papilla region promotes survival during the process of pulp necrosis. It also promotes the regeneration of pulpal tissues. In the presence of surviving epithelial cells from Hertwig’s roots sheath, it may differentiate into primary odontoblasts to induce root formation completion.19
Narang et al.20 compared regenerative procedure in 20 patients using MTA, blood clot, PRF and PRP in group I, II, III and IV respectively. It was found that 98% of cases in Group III showed excellently, 60% in Group II and 80% in Group IV showed good results in terms of periapical healing. 90% in Group III showed excellently, 40% in groups II and IV showed good results in terms of root lengthening with the non-significant difference between group (P> 0.05). Apical closure found to be good in 66.7%, 40% and 60% in group II, III and IV respectively. Revascularization accompanied with PRP contributed improved results than blood clot group.
The constraint of the present research is the smaller sample size. Only PRF and PRP material was included in this study. The inclusion of more materials could have shown better results.
Conclusion
A successful revascularization procedure in necrotic permanent anterior teeth was observed both clinically as well as radiographically. It was concluded from the present study that PRP had superior result in terms of apical closure, root lengthening and dentine wall thickness compared to the blood clot and PRF.
Conflict of interest: Nil
Source of funding: Self
Acknowledgement: Nil
Authors contribution
-
Dr. Suvarna Sunder J- review
-
Dr. Seema Abid- editing
-
Dr. Sabahat Ullah Tareen - manuscript writing
-
Dr. Prabhu Mahin S- evaluation
-
Dr. Akhil Shetty- assessment
-
Dr. Pawn Patel- data collection
References:
-
Zhang P C. Yelick AM. Vital pulp therapy-current progress of dental pulp regeneration and revascularization. Int J Dent. 2010, Article ID 856087, 9 pages.
-
Thomson S, Kahler B. Regenerative endodontics— biologically-based treatment for immature permanent teeth: a case report and review of the literature. Austr Den J. 2010; 55: 446–452.
-
Nosrat A. Seifi, and S. Asgary. Regenerative endodontic treatment (revascularization) for necrotic immature permanent molars: A review and report of two cases with a new biomaterial. J End 2011; 37: 562–567.
-
Shah A. Logani U. Bhaskar, and V. Aggarwal. Efficacy of revascularization to induce apexification/apexogenesis in infected, non-vital, immature teeth: A pilot clinical study. J Endod. 2008; 34: 919–92.
-
Garcia-Godoy F, Murray PE. Recommendations for using regenerative endodontic procedures in permanent immature traumatized teeth. Dent Traumatol 2012;28:33-41.
-
Langer and J. P. Vacanti. Tissue Engg Sci. 1993; 260: 920–926.
-
Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:638-46.
-
Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJ, Mouhyi J, et al. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:e37-44.
-
El Ashiry EA, Farsi NM, Abuzeid ST, El Ashiry MM, Bahammam HA. Dental pulp revascularization of necrotic permanent teeth with immature apices. J Clin Ped Dent. 2016;40(5):361-6.
-
Bonte E, Beslot A, Boukpessi T, Lasfargues JJ. MTA versus Ca (OH)2 in apexification of non-vital immature permanent teeth: A randomized clinical trial comparison. Clin Oral Investig. 2015; 19: 1381–1388.
-
Huang GT. A paradigm shift in endodontic management of immature teeth: conservation of stem cells for regeneration. J Dent. 2008; 36:379-386.
-
Yang M. Regenerative endodontics: a new treatment modality for pulp regeneration. JSM Dent. 2013; 1:1011.
-
Prescott RS, Alsanea R, Fayad MI, Johnson BR, Wenckus CS, Hao J, et al. In vivo generation of dental pulp?like tissue by using dental pulp stem cells, a collagen scaffold, and dentin matrix protein 1 after subcutaneous transplantation in mice. J Endod. 2008;34:421?6.
-
Windley W. Teixeira F, Levin L, Sigurdsson A, Trope M. Disinfection of immature teeth with a triple antibiotic paste. J Endod. 2005; 31:439- 443.
-
Rizk HM, Al-Deen MS, Emam AA. Comparative evaluation of Platelet Rich Plasma (PRP) versus Platelet Rich Fibrin (PRF) scaffolds in regenerative endodontic treatment of immature necrotic permanent maxillary central incisors: A double-blinded randomized controlled trial. Saud Dent J. 2020 Jul 1;32(5):224-31.
-
Ding RY, Cheung GS, Chen J, Yin XZ, Wang QQ, Zhang CF. Pulp revascularization of immature teeth with apical periodontitis: a clinical study. J Endod 2009; 35: 745-749.
-
Sunitha Raja V, Munirathnam Naidu E. Platelet-rich fibrin: Evolution of a second-generation platelet concentrate. Ind J Dent Res. 2008;19:42-6.
-
Marx RE. Platelet-rich plasma (PRP): What is PRP and what is not PRP? Impl Dent. 2001;10:225-8.
-
Lucarelli E, Beretta R, Dozza B, Tazzari PL, O'Connel SM, Ricci F, et al. A recently developed bifacial platelet-rich fibrin matrix. Eur Cell Mater. 2010;20:13-23.
-
Narang I, Mittal N, Mishra N. A comparative evaluation of the blood clot, platelet-rich plasma, and platelet-rich fibrin in the regeneration of necrotic immature permanent teeth: A clinical study. Contemp Clin Dent. 2015;6:63-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





