IJCRR - 13(13), July, 2021
Pages: 200-204
Date of Publication: 05-Jul-2021
Print Article
Download XML Download PDF
Rheumatic Manifestations in Human Immunodeficiency Virus/ Autoimmune Deficiency Syndrome Patients in Jammu Region
Author: Vinod Kumar, Ritu Bhagat, Ahmar Javid
Category: Healthcare
Abstract:Introduction: AS there is sparse data on rheumatic manifestations in HIV/AIDS in India and no prospective study on Rheumatic manifestations in HIV/AIDS patients has been conducted earlier in the J&K state, which also has a high population of HIV+ pa�tients, hence it was decided to undertake a prospective clinical study. The present study shall highlight the rheumatic manifesta�tions in HIV/AIDS patients in Jammu and this, in turn, will help physicians to target therapy accordingly to minimize the morbidity and mortality attributed to rheumatic disorders in HIV. Aim: To study the Rheumatic manifestations in HIV/AIDS patients in the Jammu region. Method and Materials: The present study was carried out on 413 patients during their visits to Voluntary Training and Counsel�ling Centre in Government Medical College, Jammu for a period of two years from 2017 to 2019. Results: There were 283 males (68.5%) and 130 females (31.4%) of the 413 HIV/AIDS patients. There were 83 (20%) subjects in WHO stage II, thirty-one (7.5%) in stage III, whereas 299(72.3%) in stage IV. Conclusion: Rheumatic disorders affect a significant proportion of HIV/AIDS patients. In the present study, the prevalence was 62.2%. Males were affected more than females. Arthralgia was the most common complaint in our study (35.7%).
Keywords: Autoimmune deficiency syndrome, Human immunodeficiency virus, Fibromyalgia
Full Text:
Introduction:
Infection by Human Immunodeficiency Virus (HIV) is characterized by a wide array of clinical manifestations, including flu-like illness in the initial stages to a multitude of clinical complications involving almost every major organ system in the body1. HIV-associated rheumatic manifestations may occur at any time of the clinical spectrum but tend to be more prevalent in later stages including AIDS1. The first reports of HIV-associated rheumatic diseases emerged in the mid-1980s, with the description of polymyositis, vasculitis, reactive arthritis and HIV-associated Sjogren’s syndrome i.e. diffuse infiltrative lymphocytosis syndrome (DILS)2,3,4,5. By 1988, it was recognized that a wide spectrum of rheumatic diseases complicated HIV infection6,7,8,9. HIV-associated rheumatic manifestations are 10
-arthralgia
-painful articular syndrome
-seronegative spondyloarthropathy
-HIV-associated arthritis
-connective tissue like disorders
-miscellaneous.
Material and Method: The present cross-sectional study was conducted in the Postgraduate Department of Medicine, GMC Jammu which involves finding Rheumatological manifestations in HIV/AIDS patients in the Jammu region during a period of two years from October 2017 to September 2019. 413 subjects included in the study were patients already diagnosed with HIV/AIDS according to WHO criteria.
Inclusion criteria:
The patients were selected for study from the following:
-
Voluntary Counselling and Training Centre, GMC Jammu
-
Patients detected to be HIV+ while being treated in GMC and its associated hospitals, Jammu (outdoor).
-
Patients referred to HIV/AIDS/ART centre GMC, Jammu from various peripheral health institutions.
Exclusion criteria:
-
HIV/AIDS + patients with co-morbid conditions like cirrhosis, diabetes mellitus, underlying malignancies.
All individuals were administered a questionnaire based on the World Health Organisation-International League against Rheumatism (WHO-ILAR), Community Oriented Programme for the control of rheumatic disorders (COPCORD) and Core Questionnaire (CQC). The purpose of the questionnaire was to screen persons with rheumatic complaints. Positive respondents were subjected to clinical examination within one week of administrating the questionnaire. In most cases, it was conducted on the same day. The points in the questionnaire were further clarified by taking the pertinent history. Physical examination was conducted with particular stress on the musculoskeletal system. No ethical clearance was required for this study and written consent was obtained from each subject for their participation in the study.
Plan of Analysis: The data obtained were analyzed with the help of computer software SPSS 12.ver. for windows and presented as mean and standard deviations. The statistically significant difference among the groups was assessed by the use of the Chi-Square test and the ‘to test. A p-value of <0.05% was considered statistically significant unless specified otherwise.
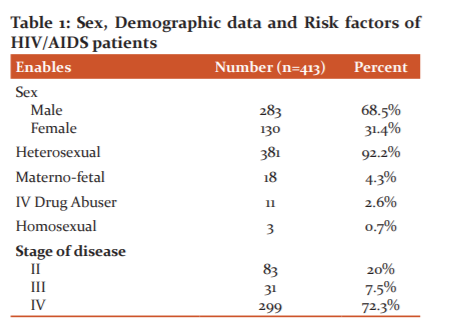
Result: Present study was undertaken to determine the point prevalence rates of major rheumatic disorders in HIV/AIDS patients in Jammu for two years from 2017 to 2019. The burden of HIV/AIDS in the community is large, not only in developed countries but also in developing countries. Since rheumatological complaints are very common in HIV/AIDS patients, so the physician is encountering an increased number of rheumatological diseases in HIV/AIDS patients in their practice. The following observations were made and shown in Table 1. There were 283 males (68.5%) and 130 (31.4%) females. Out of these 3 were homosexual and 11 were IV drug abusers, 381 were heterosexual. 83 were in clinical stage II, 31 were in stage III and 299 were in stage IV.
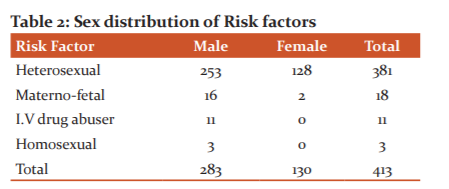
In materno-fetal transmission, there were 16 males and 2 females. In IV drug abuser 11 males only. In heterosexual here were 253 males and 128 Females. In homosexual, there were 3 males only ( Table 2).
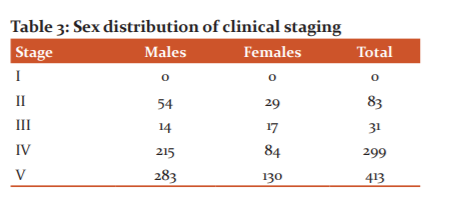
In clinical stage II, there were 54 males and 29 females. In clinical stage II, There were 14 males and 17 females. In clinical stage IV, there were 215 males and 84 females ( Table 3).
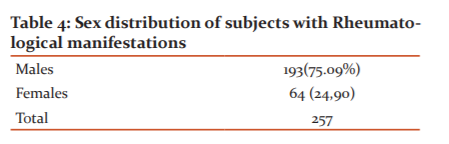
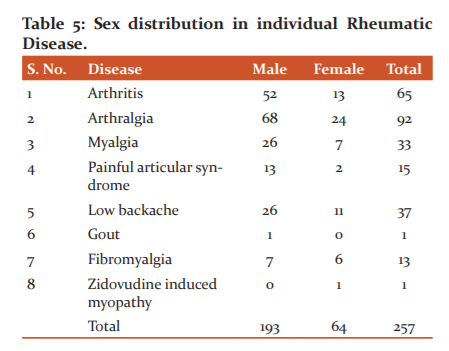
There were a total of 257 subjects with rheumatological manifestations. Out of these, there were 193 males and 64 females.
In arthritis, there were 52 males and 13 female wherein in arthralgia there were 68 males and 24 females. In myalgia, there were 26 males and 7 females. In painful articular syndrome, there were 13 males and 2 females. In low backache, there were 26 male and 11 females. In gout, there was 1 male. In fibromyalgia, there were 7 males and 6 females. In Zidovudine induced myopathy there was 1 female.
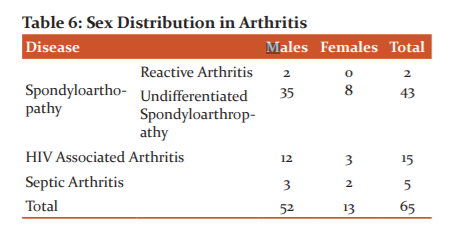
Out of 65 subjects (25.2%) spondyloarthropathy were found in 45 (69.2%) subjects, HIV associated arthritis in 15 (23.0%) subjects and septic arthritis in 5(7.6%) subjects. Out of 45, there were 37 males (82.2%) and 8 (17.7%) females. Two of the reactive arthritis patients were male children in the age group of 5 & 9. Out of 43 undifferentiated spondyloarthropathies, 35 (81.3%) males and 8 (18.6) were females. Out of 15 HIV -associated arthritis there were 12 (80%) males and 3 (20%) females.
Discussion:
A total of 257 rheumatic complaints were reported in this study and that is a prevalence of 62.2%. As reported by Xuan Zhang et al.11 rheumatic manifestations were found in 54.08%. Simms et al.12 reported rheumatic manifestations in 71.2% of the subject. Buskila et al.9 reported rheumatic manifestations in 66.1% of patients. Rogeaux et al.13 reported rheumatic manifestations in 79.1% of patients. Medina et al.14 reported rheumatological manifestations in 63% of cases. Munoz et al.8 reported rheumatological manifestations in 11% of patients. Narayanan et al.15 reported rheumatological disorders in 2% of cases. Achuthan et al.16, reported rheumatic disorders in 7.8% of cases. Vaidya et al.17 reported rheumatological complaints in 4% of cases.
Arthritis was found in 65 subjects 25.2%. There were 52 males (80%) and 13 (20%) females. Berman et al.18 reported arthritis in 24% of cases. Buskila et al.9 reported arthritis in 19% of cases. Medina et al.14 reported arthritis in 18% of patient. Krishnan et al.19 reported arthritis in 62% of cases. Marquez et al.20 reported arthritis in 13.3% of cases. Buskila et al.9 reported spondyloarthropathy in 15.2% of cases. Rogeaux et al.13 reported spondyloarthropathy in 20% of patients. Krishan et al.19 found spondyloarthropathy up to 28.1%. Blanche et al.21 reported spondyloarthropathy in 78.9% of HIV infected patients. Blanche et al.22 in Rwanda found spondyloarthropathy in 38.4% of patients.
In our study HIV – associated arthritis was found in 15 (23.0%) of subjects. Krishnan et al.19 found HIV – associated arthritis in 17.2%) of cases. Blackout et al.23 reported in 35% of cases. Blanche et al.22 reported HIV –associated arthritis in 15.3% of cases. Njobvu et al.24 reported HIV –associated arthritis in 22.7% of cases. Blackout et al.25 reported HIV –associated arthritis in 82% of the subject. Virtanen et al.26 reported HIV –associated arthritis in 46.6% of cases.
Septic arthritis was found in 5 (7.6%) of cases In our study, whereas Bileckot et al.25 reported septic arthritis in 5.1% of cases. Krishnan et al.19 reported septic arthritis in 3.4% of cases. Rogeaux et al.13 reported no case of septic arthritis. Cuellar et al.10 reported a prevalence of 1-4 % of septic arthritis. Blanche et al.22 reported septic arthritis in 34.6% of cases. Monteagudo et al.27 reported septic arthritis in 0.9% of cases.
Berman et al.6 reported Reiter's syndrome in 9.9%> of cases. Rogeaux et al.13 reported Reiter's syndrome in 1.6% of cases. Munoz et al.8 reported in 0.5%> of cases. Medina et al.14 reported in 8% of cases. Andrew28 reported a prevalence of 0 to 10%. Krishnan et al.19 reported Reiter’s syndrome in 7.1% of cases. Blackout et al.25 reported no case of Reiter's syndrome. Njobvu et al.24 reported Reiter's syndrome in 2% of cases. Virtanen et al.26 reported a prevalence of 20%. Massabki et al.29 reported in 2% of cases. Stein et al.30 in 37.5% of cases, In the present study no case of Reiter’s syndrome was found.
Arthralgia was found in 92 cases (35.7%). Out of these 68 (73.9%) were males and 24 (26.0%) were females. Berman et al.6 reported arthralgia in 34.6% of cases. Buskila et al.9 reported arthralgia in 15.2% of cases. Rogeaux et al.13 in 12.4% of cases. Munoz et al.8 reported arthralgia in 4.5% of cases. Medina et al.14 reported in 45% of cases. Krishnan et al.19 reported arthralgia in 21% of cases. Kanokwan et al.31 reported arthralgia in 26% of cases. Monteagudo et al.27 reported arthralgia in 12.2% of cases. Virtanen et al.26 reported arthralgia in 20% of cases.
The painful articular syndrome was diagnosed in 15 (5.8%>) patients of whom 13 (86.6%) were males and 2 (13.3%) were females. Berman et al.6 reported Painful articular syndrome in 9.9%> of cases. A painful articular syndrome is not reported by Krishnan et al.19 as well as Achuthan et al.16. Celular et al.10 reported painful articular syndrome in 10%> of cases. Rogeaux et al.13 reported painful articular syndrome in 4.1 % of cases.
myalgia was found in 33 (12.8%) cases. Monteagudo et al.27 reported myalgia in 12.2% of cases. Krishnan et al.19 reported myalgia in 14% of cases. Buskila et al.9 found myalgia in 35% of cases. Virtanen et al.26 in 6.6% of cases. Massabki et al.29 reported it in 28% of cases. Low backache was found in 37 subjects (14.3%). Berman et al.6 reported low backache in (14.2%) of cases. Rogeaux et al.13 reported low backache in 36.6%) of cases. Krishnan et al.19 reported no case of low backache. Virtanen et al.26 reported no case of low backache. Kanokwan et al.31 reported no case of low backache.
Fibromyalgia was found in 13 subjects (5%) in our study. Out of the 7 (53.8%) were males and 6 (46.1%) were females. Simms et al.12 reported a prevalence of 11% for fibromyalgia in HIV positive patients and 41% of HIV patients with musculoskeletal symptoms. Krishnan et al.19 reported no case of fibromyalgia. Virtanen et al.26 reported no case of fibromyalgia. Kanokwan et al.31 reported no case of fibromyalgia.
Zidovudine induced myopathy was reported in one (0.3%) patient in the present study and no case of polymyositis or dermatomyositis was found. Xuan et al.11 reported Zidovudine induced myopathy in 35% of cases. Krishnan et al.19 reported polymyositis in 3.4% of cases. Johnson et al.32 reported biopsy-proven myositis in 20%. Xuan et al.11 reported myositis in 8.16% of cases. Massabki et al.29 reported polymyositis in 1.1 % of cases. Johnson et al.32 reported myositis in 0.22%> of cases. Narayanan et al.15 reported no case of polymyositis.
No case of Sjogren’s syndrome/ diffuse infiltrative lymphocytosis syndrome has been reported in our study. Buskila et al.9 reported Sjogren's syndrome in 1.9%> of subjects. Rogeaux et al.13 reported no case of Sjogren syndrome / DILS in their study of 121 subjects. Munoz et al.8 reported no case of DILS/Sjogren's syndrome in 556 HIV +ve patients. Williams et al.33 found diffuse infiltrative lymphocytosis syndrome in 3%o of subjects. Krishnan et al.19 reported no case of DILS/ Sjogren syndrome in 29 HIV+ve subjects. Johnson et al.32 found concomitant diffuse infiltrative lymphocytosis syndrome in 9.3% of patients who were having myositis. Xuan et al.11 reported 11.2% of cases with Sjogren like syndrome/Diffuse infiltrative lymphocytosis syndrome.
No case of vasculitis was found in our study. Berman et al.6 found a prevalence of 0.9%. Simpson et al.34 reported no case of vasculitis Buskila et al.9 reported in 1.9% cases. Rogeaux et al.13 reported vasculitis in 0.8% of cases. Munoz et al.8 reported vasculitis in 0.4%o of cases. Krishnan et al.19 reported no case of vasculitis. Marquez et al.20 reported no case of vasculitis in their 75 patients. Xuan et al.11 reported vasculitis in 20.41% of cases including Bechet like disease, Henoch-Schonlein purpura and digital gangrene. Stein et al.30 reported no case of vasculitis. Otero et al.35 reported vasculitis in 8 patients. Kanokwan et al.31 reported vasculitis in 18%o of subjects. Manteagudo et al.27 reported vasculitis in 0.9% of cases. Massabki et al.29 reported vasculitis in 1% of cases. Narayanan et al.15 reported no case of vasculitis in their 469 HIV positive patients.
No case of SLE like disease was found in our study. Berman et al.6 reported no case of SLE like a disease. Buskila et al.9 reported no case of SLE. Elizabeth et al.36 reported that the prevalence of lupus In HIV is very low and from 1988-2002 only 30 cases were reported. Munoz et al.8 reported no case of lupus in 556 HIV positive patients. Krishnan et al.19 reported no case of lupus. Marquez et al.20 reported no case of lupus in their study. Xuan et al.11 reported a lupus-like disease in 10.2% of subjects.
A case of gout is found in our study (0.3%). No case of gout was reported by Buskila et al.9. Berman et al.6 reported no case of gout. Krishnan et al.19 reported no case of Gout. Basu et al.37 retrospectively did chart review and reported no case of gout during 1997, 3% of cases during 1998, 2% of cases during 1999, 2% of cases during 2000, 4% of cases during 2001, 3% of cases during 2002, 2% of cases during 2003, 2% of cases during 2004 and 2% of cases during 2005.
Conclusion: As rheumatic manifestations are very common in HIV/AIDS patients. The present study is to define the occurrence of various Rheumatic manifestations in HIV/AIDS patients. The present study was conducted on 413 subjects during their visit to Voluntary Training and Counseling Centre in Government Medical College Jammu, J&K. There were 283 males (68.5%) and 130 females (31.4%) of the 413 HIV/AIDS patients. There were 83 (20%) subjects in WHO Stage II, thirty-one (7.5%) in Stage III, whereas 299 (72.3%) in Stage IV. In the present study, the prevalence was 62.2%. Males were affected more than females. Arthralgia was the most common complaint in our study (35.7%). A rare case of gout (0.03%) is found in our study.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of funding: nil
References:
-
Cuellar ML. HIV: Infection–associated inflammatory musculoskeletal disorders. Rheum Dis Clin North Am. 1998; 24: 403-21.
-
Dalakas MC, Pezeshkpour GS, Gravell M. Polymyositis associated with AIDS retrovirus. J Am Med Ass. 1986; 256: 2381-83.
-
Yanker BA, Skolnik PR, Shoukimas GM, Gabuzda DH, Sobel RA and Ho DD. Cerebral granulomatous angiitis associated with the isolation of human T- lymphotropic virus type - III from the central nervous system. Ann Neur. 1986; 20: 362- 64.
-
Winchester R, Bernstein DH, Fischer HD, Roger Enlow and Gary Solomon. The co-occurrence of Reiter's syndrome and acquired immunodeficiency. Ann Internal Med. 1987; 106: 19-26.
-
Ulirsch RC and Jaffe ES. Sjogren's syndrome-like illness associated with the acquired immunodeficiency syndrome related complex. Human path. 1987; 18: 1063- 68.
-
Berman A, Espinoza LR, Diaz JD, et al. Rheumatic manifestations of human immunodeficiency virus infection. Am J Med. 1988; 85: 59-64.
-
Calabrese LH. Autoimmune manifestations of human immunodeficiency virus (HIV) infection. Clin Lab Med. 1988; 8: 269-279.
-
Fernandez S Munoz, Cardenal A, Balsa A, et al. Rheumatic manifestations in 556 patients with human immunodeficiency virus infection. Sem Arthr Rheum. 1991; 21: 30-39.
-
Buskila D, Gladman DD, Langevitz P, Bookman AA, Fanning M and Salit IE. Rheumatologic manifestations of infection with the human immunodeficiency virus (HIV). Clin Expt Rheum. 1990; 8: 567-73.
-
Cuellar ML and Espinoza LR. Rheumatic manifestation of HIV – AIDS. Baillieres Clin Rheum. 2000; 14 (3): 579-93.
-
Xuan Zhang, Hongbin Li, Taisheng Li, Fengchun Zhang and Yang Han. Distinctive rheumatic manifestation in 98 patients with Human Immunodeficiency Virus infection in China. J Rheum. 2007; 34: 1760-64.
-
Simms RW, Zerbini CAF, Ferrante N, Anthony J, Felson DT and Craven DE. Boston City Hospital Clinical AIDS Team: Fibromyalgia syndrome in patients infected with human immunodeficiency virus. Am J Med. 1992; 92: 368- 74.
-
Rogeaux O, Fassin D and Gentilini M. Prevalence of Rheumatic manifestations in immunodeficiency virus infection.ANN Med Interne(Paris). 1993;144(7):443-8.
-
Medina- Rodriguez F, Guzman C, Jara LJ, Hemida C, Alboukrek D and Cervera H. Rheumatic manifestation in Human Immunodeficiency Virus positive and negative individuals. A study of two populations with similar risk factors. J Rheum. 1993; 20:1880-84.
-
K Narayanan, Batra RB and Anand KP. Rheumatic manifestations of HIV infection. Ind J Rheum. 2008; 3(1): 4-7.
-
Achuthan K and Uppal SS. Rheumatological manifestations in 102 cases of HIV infection. J Int Rheu Arth 1996; 3: 43-47.
-
Vaidya S, Samant RS, Nadkar MY, Kopikkar GV, Kulkarni MG and Wadhva SL. HIV Infec Rheum dis. J Rheum Arth. 1996; 4: 83-87.
-
Berman A, Reboredo G, Spindler A, Lasala ME, Lopez H and Espinoza LR. Rheumatic manifestations in populations at risk for HIV infection: the added effect of HIV. J Rheum . 1991; 18(10): 1564-67.
-
Krishnan KK, Panchapakesa CR, Porkodi R, Madhavan R, Ledge SG and Mahesh A. Rheumatological manifestations in HIV-positive patients referred to a tertiary care centre. J Indian Rheum Assoc. 2003; 11: 104- 08.
-
Marquez J, Restrepo CS, Candia L, Berman A and Espinoza LR. Human immunodeficiency virus-associated rheumatic disorders in the HAART era. J Rheum. 2004;31 (4): 741-46.
-
Blanche P, Sicard D, Saraux A and Taelman H. Arthritis and HIV infection in Kigali, Rwanda and Paris, France. J Rheum. 1997; 24: 1149-1150.
-
Blanche P, Taelman H, Saraux A, Sicard D and Menkes JC. Acute arthritis and Human Immunodeficiency Virus infection in Rwanda. J Rheum. 1993; 20: 2123-27.
-
Bileckot R, Koubemba G and NKoua JL. Etiology of oligoarthritis in equatorial Africa. A retrospective study of 80 patients in Brazzaville, Congo. Rev Med Interne. 1999: 20: 408-417.
-
Njobvu P and McGill P. Psoriatic arthritis & human immunodeficiency virus infection in Zambia. J Rheum. 2000; 27: 1699-02.
-
Bileckot R, Mouraya A and Makuwa M. Prevalence and clinical presentation of arthritis in HIV Positive patients seen at the Rheumatology department in Congo Brazzaville. Rev Rhum Engl Ed. 1998 Oct;65(10):549-54.
-
Vertmen JF, Lite NH and Goldfarb MJ. AIDS & Rheumatic manifestations study of 15 cases. International Conference on AIDS 1994; 10: 199.
-
I Monteagudo, J Rivera, J Lopez-Longo, J Cosin, A Garcia-Monforte and L Carreno. AIDS & Rheumatic manifestations in a patient addicted to drug and analysis of 106 cases. J Rheum. 1991; 18: 1038-41.
-
Andrew Keat. HIV and overlap with Reiter's Syndrome. Baillieres Clin Rheum. 1994; 8:363-77.
-
Massabki Parlo S, Accetturi C, Nishie IA, da Silva NP, Sato EI and Andrade LE. Clinical implications of autoantibodies in HIV infection.AIDS. 1997; 11 (15): 1845-50.
-
Stein CM and Davis P. Arthritis associated with HIV infection In Zimbabwe. Journal of Rheumatology. 1996; 23: 506-11.
-
Kanokwan Kuthaner MD. Autoimmune and Rheumatic manifestation and antinuclear antibody study in HIV infected Thai patients. Int J Derm. 2002; 41 (7): 417-22.
-
Johnson RW, Williams FM, Kazi S, Dimachkie MM and Reveille JD. Human Immunodeficiency virus-associated polymyositis: a longitudinal study of outcome. Semi Arth Rheum. 2003; 49 (2): 172-78.
-
Williams FM, Cohen PR, Jumshyd J and Reveille JD. Prevalence of the diffuse infiltrative lymphocytosis syndrome among human immunodeficiency virus type-1 positive outpatients. Semi Arth Rheum. 1998; 41 (5): 863-68.
-
Simpson DM, Bender AN. Human immunodeficiency virus-associated myopathy; Analysis of 11 patients. Ann Neur. 1988; 24: 79-84.
-
Otedo AEO, Oyoo GO, Obondi JO, Otieno CF. Vasculitis in HIV report of eight cares. East Afri Med J. 2005; 82: 656-59.
-
Elizabeth CC, Fariba Rezaee and Joel Mendelson. Pediatric patient with Systemic Lupus erythematosus & congenital acquired immunodeficiency syndrome. An unusual case & review of the Literature. Pediat Rheumat. 2008; 6:7.
-
Basu D, Williams FM, Ahn CW and Reveille JD. Changing spectrum of the diffuse infiltrative lymphocytosis syndrome. Semin Arthr Rheum. 2006; 55(3) : 466-72.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





