IJCRR - 13(13), July, 2021
Pages: 114-117
Date of Publication: 05-Jul-2021
Print Article
Download XML Download PDF
Systolic Blood Pressure and Heart Rate Responses of Individuals with Neck Versus Abdominal Obesity in Response to - Incentive Spirometry Based 10 Sustained Maximal Inspirations (A Possible Clinical Tool)
Author: Mayank Shukla, Ankita Samuel
Category: Healthcare
Abstract:Introduction: Deposition of fat over the upper trunk and neck is called neck obesity. It is a topographical central fat distribution. In this cross-sectional study, it is demonstrated that individuals with neck obesity are having a hyperresponsive cardiovascular system, to the incentive spirometry breathing exercise as compared to abdominal obese individuals. Objective: To check sustained maximal inspirations using incentive spirometry (IS) as a tool for cardiovascular (CVS) responses of the neck and abdominal obese individuals. Methods: Sample size and population: N=30 individuals (15 with neck obesity and 15 with abdominal obesity volunteered and gave written informed consent to participate. The setting was the Research Lab of AIPT, Amity University, Noida, UP. India. Inclusion Criteria: Age group: 18-30 years; BMI ≥25kg/cm2 ; Circumference of abdomen ≥ 88 cm in females and ≥ 102 cm in males; [abdominal obesity group]; Circumference of neck ≥ 35 cm in females and ≥ 41 cm in males. [neck obesity group]. Ex�clusion Criteria: Any previous history of cardiovascular disease; Uncontrolled diabetes mellitus; Hb, < 10mg/dl; Known asthma; known COPD; Smoking history.Intervention: Sustained maximal inspirations 10 per minute were carefully administered. Outcome measures: heart rate, blood pressure responses. Results: Significant changes in systolic blood pressure (SBP) & heart rate (HR) are seen between the neck and abdominal obese population (p< 0.05) at 95% CI. Pre incentive spirometry Sustained Maximal Inspiration breaths, SBP of abdominal obese individuals (mean\?SD-115.47\?7.38) was higher than neck obese (mean\?SD-108.73\?8.54) at (p = 0.028*); whereas post-incentive spirometry SBP was more in neck obese ((mean\?SD-126.80\?7.84 ) than in abdominal obese ((mean\?SD-114.0\?11.0) at (p = 0.001*). HR also increased significantly post incentive spirometer in neck obese (mean\?SD-100.53\?11.37) than in abdominal obese (mean\?SD-92.80\?1.16) at (p = 0.046*). Conclusion: IS based CVS responses are significantly different in the neck obese. It may be checked further using IS based SMI as a tool for other populations.
Keywords: Hypertension, Tachycardia, Cardiovascular screening, Obesity, Sustained maximal inspirations
Full Text:
INTRODUCTION
Excessive deposition of fat topographically on specific body segments is known as regional obesity. It may cause cardiovascular presentations.1 Neck obesity is considered an index of upper body obesity. It may cause different responses of blood pressure from those seen for abdominal obesity.2 Incentive spirometry (IS) induces sustained maximal inspirations (SMI). They produce changes in the cardiovascular features. Cardiopulmonary is a single functional unit that gives rise to two different body systems of cardiovascular and pulmonary.3,4
OBJECTIVE
The objective was to compare responses of systolic and diastolic blood pressure, heart rate and peripheral arterial saturation of neck obese and abdominal obese individuals to 10 breaths in 1minute using IS.
PROPOSED RATIONALE AND IMPLICATIONS
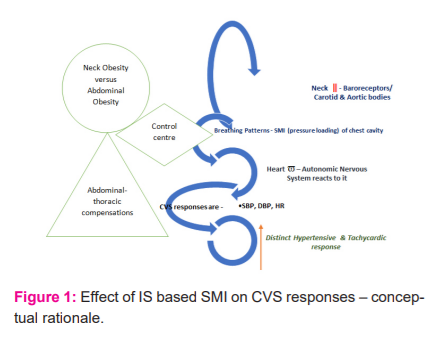
The rationale is seen in Fig. 1. Changes in the neck can lead to changes in CVS responses to IS based SMI. Interconnecting structures are carotid and aortic bodies via the autonomic nervous system. How fat deposition changes these features is to be found. Framingham heart study in their landmark findings have reported upon the localization of fat deposition and related health risk.17
RESULT AND DISCUSSION
Institutional Ethical clearance and informed consent: The study protocol was reviewed and cleared by the Institutional NTCC committee of Amity Institute of Physiotherapy, Amity University Uttar Pradesh. NTCC/AIPT/MPT AY 2014-15-A1102713009.Weekly review and internal and external presentations were done for the progress. Written informed consent was obtained from all participants.
N=30 Individual with obesity (15 necks obese and 15 abdominal obese) was taken as per the inclusion and exclusion criteria. Both males and females participated in the study as seen in Table -1.
Their resting blood pressure, heart rate, and peripheral oxygen saturation (SpO2) were recorded twice, and an average was taken, following which they were asked to breathe in and out of a flow-based incentive spirometer (IS) 10 breaths in a minute. During these patients were instructed to take inspirations and to raise the ball maximally, hold it for 5 seconds and repeat it after a brief pause. Incentive spirometry induces biofeedback & self-controlled sustained maximal inspirations (SMI). After IS the parameters were measured again immediately. 5, 6, 7

Written informed consent was taken from all participants. Ethical approval for this research was granted by the institutional NTCC committee of AIPT, AUUP.
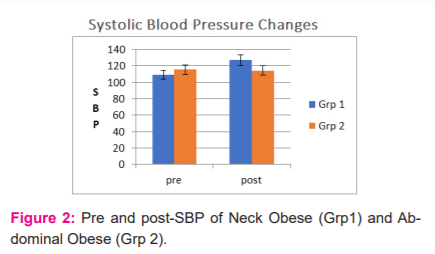
Systolic blood pressure is a marker of cardiac contractility, which usually is required to overcome the afterload. Significant changes in this are interpreted as increased contractility of the myocardium. Increased systolic blood pressure is responsible for various adverse effects. In Fig 2 it is seen that there are a significant increase in SBP for neck obese (Grp-1) individuals in response to IS based 10 SMIs in 1 minute. Neck circumference is reported to have higher odds of hypertension.18There are recent reports of cut-off points of NC for children for cardiometabolic risk.19A systematic review has also confirmed NC as a new measure for hypertension. We have shown hyperresponsive SBP to IS based SMIs, it may be taken up in future studies how this measure affects clinical outcomes in different population like individuals with metabolic syndrome or survivors of an acute cardiac event. 8,9 Also, routine use of hypertensive response to IS based 10 SMI instead of resting BP, or in addition to it is a new paradigm of this research report.
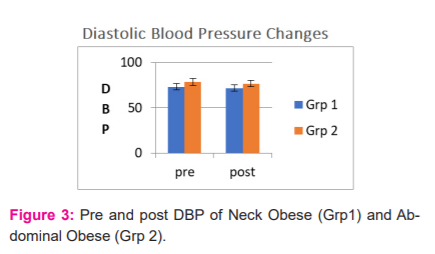
Diastolic blood pressure (DBP) usually does not change in response to respiratory interaction in asymptomatic individuals, therefore changes are not witnessed by us in DBP with SMI as seen in Fig-3. It is dependent upon the cardiac preload; it may vary in the clinical populations and may be checked by future studies carried out for the IS based SMI responses. 10,11

Heart rate is seen as changing significantly in the study as seen in Fig 4. This is important because increased heart rate is a response that may form the very basis of all adverse effects as well. It has obvious clinical implication for symptomatology during activities of daily living, occupational or leisure time for different populations with regional obesity.12
The neck is the connecting body segment between the cranium and trunk. It houses the cervical spine, brain stem, cervical plexus, carotid arteries, baroreceptors, carotid bodies, trachea, oesophagus and thyroid gland. The distribution of fat varies among individuals with obesity irrespective of gender where there may be more deposition on the trunk or the neck in certain individuals leading to specific physiological changes.2 Deposition of fat on the neck is an independent prognostic marker for cardiovascular diseases and may reflect in the general assessment of obese individuals.3,4 In clinical practices, the BMI is usually considered as an obesity marker and abdominal obesity is also considered. Neck obesity is not considered generally.5 It can be easily checked by checking neck circumference. 13,14,15
Incentive spirometry involves the use of sustained maximal inspirations. These bellowing movements of the lungs and sustained maximal inspiration/ Valsalva manoeuvre are known to stimulate the nervous system.6 Cardiopulmonary system is one unit and changes in each usually reflect in the other.7 Thus incentive spirometry was used. It is commonly used in hospitals and clinics.
The cardiovascular responses were exaggerated among the individuals with neck obesity and it may have a sympathetic wing activation response in the autonomic nervous system.1,8,9There are many reports which have demonstrated the different clinical implications of obesity and neck obesity has become a cause to fight for.,14,15.
It has been seen in the present study that cardiovascular responses are exaggerated to incentive spirometry induced sustained maximal inspirations significantly among neck obese. This forms an important simple clinical test that may be used for the global neck obese population’ CVS.17
During the screening of COVID-19 cases after they have recovered and for checking the cardiac status this test (IS based CVS screening) is making a case as well.18, 19,20
CONCLUSION
Neck Obesity is an independent cardiovascular clinical marker that needs to be checked for preventive and treatment effects. Testing CVS responses to 10 sustained maximal breaths in a minute using incentive spirometry, can be used in initial and follow-up screening of susceptible populations.
Conflict of interest: Authors declare no conflict of interest.
Financial support: Nil.
Acknowledgement: Authors would like to acknowledge all participants for their time and participation. The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals, and books from where the literature for this article has been reviewed and discussed. The authors also acknowledge the valuable comments of the reviewers and editors.
Authors’ Contribution: Ankita Samuel contributed to conceptualization, data collection, analysis, report writing for the research. Mayank Shukla contributed to conceptualization, data analysis, report writing and journal communication for the paper.
References:
1.Kotsis V, Stabouli S, Papakatsika S, Rizos Z, Parati G. Mechanisms of obesity-induced hypertension. Hypertens Res. 2010 May;33(5):386-93.
2.Zen V, Fuchs FD, Wainstein MV, Gonçalves SC, Biavatti K, Riedner CE, Fuchs FC, Wainstein RV, Rhoden EL, Ribeiro JP, Fuchs SC. Neck circumference and central obesity are independent predictors of coronary artery disease in patients undergoing coronary angiography. Am J Cardiovasc Dis. 2012;2(4):323-30.
3.Joshipura K, Muñoz-Torres F, Vergara J, Palacios C, Pérez CM. Neck Circumference May Be a Better Alternative to Standard Anthropometric Measures. J Diabetes Res. 2016; 2016:6058916.
4.Wang Y, Chen HJ, Shaikh S, Mathur P. Is obesity becoming a public health problem in India? Examine the shift from under- to overnutrition problems over time. Obes Rev. 2009 Jul;10(4):456-74.
5.Borel AL, Coumes S, Reche F, Ruckly S, Pépin JL, Tamisier R, Wion N, Arvieux C. Waist, neck circumferences, waist-to-hip ratio: Which is the best cardiometabolic risk marker in women with severe obesity? The SOON cohort. PLoS One. 2018 Nov 8;13(11): e0206617.
6.Yakinci C, Mungen B, Karabiber H, Tayfun M, Evereklioglu C. Autonomic nervous system functions in obese children. Brain Dev. 2000 May;22(3):151-3.
7.Tonhajzerova I, Javorka M, Trunkvalterova Z, Chroma O, Javorkova J, Lazarova Z, Ciljakova M, Javorka K. Cardio-respiratory interaction and autonomic dysfunction in obesity. J Physiol Pharmacol. 2008 Dec 1;59(Suppl 6):709-18.
8.Malden D, Lacey B, Emberson J, Karpe F, Allen N, Bennett D, Lewington S. Body Fat Distribution and Systolic Blood Pressure in 10,000 Adults with Whole-Body Imaging: UK Biobank and Oxford BioBank. Obesity (Silver Spring). 2019 Jul;27(7):1200-1206.
9.Balasubramanian P, Hall D, Subramanian M. Sympathetic nervous system as a target for aging and obesity-related cardiovascular diseases. Gerosci. 2019 Feb 15;41(1):13-24.
10.Sparrow D, Borkan GA, Gerzof SG, Wisniewski C, Silbert CK. Relationship of fat distribution to glucose tolerance: results of computed tomography in male participants of the Normative Aging Study. Diab. 1986 Apr 1;35(4):411-5.
11.Cornier MA, Despres JP, Davis N, Grossniklaus DA, Klein S, Lamarche B et al. Assessing adiposity: a scientific statement from the American Heart Association. Circul. 2011 Nov 1;124(18):1996-2019.
12.Bastien M, Poirier P, Lemieux I, Després JP. Overview of epidemiology and contribution of obesity to cardiovascular disease. Progress in cardiovascular diseases. 2014 Jan 1;56(4):369-81.
13.Ortega FB, Sui X, Lavie CJ, Blair SN. Body mass index, the most widely used but also widely criticized index: would a criterion standard measure of total body fat be a better predictor of cardiovascular disease mortality? In Mayo Clinic Proceed. 2016 Apr 91; (4):443-455.
14.Piché ME, Poirier P, Lemieux I, Després JP. Overview of epidemiology and contribution of obesity and body fat distribution to cardiovascular disease: an update. Progr Cardiov Dise. 2018 Jul 1;61(2):103-13.
15.Henriksson H, Henriksson P, Tynelius P, Ekstedt M, Berglind D, Labayen I, et al. Cardiorespiratory fitness, muscular strength, and obesity in adolescence and later chronic disability due to cardiovascular disease: a cohort study of 1 million men. Eur Heart J. 2020 Apr 14;41(15):1503-1510.
16. Clerkin KJ, Fried JA, Raikhelkar J, Sayer G, Griffin JM, Masoumi A, Jain SS, Burkhoff D, Kumaraiah D, Rabbani L, Schwartz A. COVID-19 and cardiovascular disease. Circul. 2020 May 19;141(20):1648-55.
17-Kannel WB, Cupples LA, Ramaswami R, Stokes III J, Kreger BE, Higgins M. Regional obesity and risk of cardiovascular disease; the Framingham Study. J Cli Epidem. 1991 Jan 1;44(2):183-90.
18- Nafiu OO, Zepeda A, Curcio C, Prasad Y. Association of neck circumference and obesity status with elevated blood pressure in children. J Hum Hypert. 2014 Apr;28(4):263-8.
19- de Santis Filgueiras M, de Albuquerque FM, Castro AP, Rocha NP, Milagres LC, de Novaes JF. Neck circumference cutoff points to identify excess android fat. J de pediatria. 2020 May 1;96(3):356-63.
20- Moradi S, Mohammadi H, Javaheri A, Ghavami A, Rouhani MH. Association between neck circumference and blood pressure: a systematic review and meta-analysis of observational studies. Horm Metab Res. 2019 Aug 1;51(8):495-502.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





