IJCRR - 13(13), July, 2021
Pages: 91-96
Date of Publication: 05-Jul-2021
Print Article
Download XML Download PDF
Application of Dialectical Behavior Therapy (DBT) for Opioid Dependence: Case Study
Author: Komal S, Nandha KP
Category: Healthcare
Abstract:Background: Opioid dependency is among serious clinical and public health concerns in India. India has had an established pattern of use of an opioid group of drugs. Indeed, a sizable number of people in India use opioid drugs, suffer from opioid dependence and seek treatment for the same. The most common treatment strategy for opioid dependence is opioid substitution therapy (OST). Another regimen used for substance dependents is Dialectical behaviour therapy (DBT). It is said to incorporate concepts and modalities which are designed to promote abstinence and thereafter reduce the length of consumption and also the adverse impact of relapses. Case Presentation: This case study is about AB, a 23-years old male who sought care for opium dependence. His chief complaints were inability to cut down the use of the substance (opium paste), experiencing withdrawal symptoms, low mood, low self-confidence and increased craving for the substance. Psychological Assessment that was done comprised of Severity of dependence scale (SDS), Brief-Cope Questionnaire, Emotional Regulation Questionnaire (ERQ) and Interpersonal Competence Questionnaire-15 (ICQ-15). Subsequently, TAU along with DBT techniques was applied over two months (13 sessions) and showed significant improvement in the patient. The outcome of the intervention showed a decline in independence levels, increased distress tolerance, better emotional regulation and interpersonal relationships. The patient eventually demonstrated decreased drug usage and improved skilful behaviour. Conclusion: Thus, it can be concluded that DBT is effective along with pharmacology therapy to promote and enhance the holistic well-being of the patient with opioid dependence. This gives an example of how trainee treatment can be used not only to decrease opioid dependency level but also to increase distress tolerance, better emotional regulation and interpersonal effectiveness in relationships.
Keywords: Clinical Psychiatry, Emotional regulation, Inter-personal competence, Opioid dependence.
Full Text:
INTRODUCTION
The use of psychoactive substances has been part of human civilization for thousands of years. The pattern and dimensions of the use of such psychoactive substances, however, have taken on pathological proportions in modern times.1 in all parts of the world, narcotics have become a scourge, both in villages and towns. Heroin or other synthetic illicit drugs are widely prevalent like distilled opium.
If not quantifiable correctly, the complexity of the issue is undeniably vast and troubling. Being one of the largest legal producers of opium, India has had an established pattern of use of an opioid group of drugs. This has resulted in a sizable number of people who are using opioid drugs or are suffering from opioid dependence and seek treatment for the same.2 In the first and the only national survey to date on drug use in India, the prevalence of opioid use was found to be 0.7% of the general population among whom, around 22.3% were found to be opioid dependents.3
Opiate dependence is a chronic relapsing condition with sometimes catastrophic effects for individuals, families and communities. This has been seen as intensified in poor resource settings.4
In the last decade, the treatment and care structure of opioid addiction has changed considerably. Eventually, the focus has been put on implementing ambulatory methadone maintenance therapy (MMT) and buprenorphine maintenance (BMT)5. Maintenance therapies are given either through major specialist substitution centres (SSCs) or more recently through primary care doctors who either are entirely eligible to provide MMT / BMT treatment or those who have used it on few patients.5
Opioid substitution therapy (OST) is the most commonly used evidence-based treatment for opioid dependence in pharmacotherapy.6 although available in India for about three decades now, Indian research on this treatment modality has not been adequately reviewed so far. It is not a wholesome cure for drug dependence rather it is a therapy for the management of a chronic condition. Some clients may need therapy for years and some for their entire life.6-9
Another regimen used for substance abusers is Dialectical behaviour therapy (DBT). It is said to incorporate concepts and modalities which are designed to promote abstinence and thereafter reduce the length of consumption and also the adverse impact of relapses.10 it is a stem of psychotherapy that has been used as an adjunct to pharmacotherapy. It was developed by Marsha Linehan (Ph.D.) in 1980 which focuses on both cognitive and behavioural aspects of psychological treatments. Being an inclusive treatment program helps the patients with their efforts to build a life worth living.11 A successful DBT intervention helps the patient to learn to predict, communicate, pursue and maintain goals that are independent of their history of out-of-control behaviour, including substance abuse and are better able to cope with life’s day to day problems.11, 12
In the initial controlled trial of Linehan, while treating people with BPD, DBT proved to be efficacious to decrease their behaviour by themselves and their stationary psychiatric days.11 In another clinical study, DBT has demonstrated effective drug de-addiction, opioid use reduction, decrease elderly depression and adaptive coping ability, improved likelihood of completion of treatment and hospitalization among suicidal adolescents.12,13
CASE PRESENTATION
In the present case report, DBT was given to a male patient (AB) aged 23 to reduce his opioid dependence. AB was a student studying and living in Delhi. He recently presented for treatment at the psychology training clinic because his family was concerned that the use of opioid was interfering with his daily living and has destructed his life. In 2017, due to some family reasons, his family had to move to another city and he lived alone in Delhi to complete his post-graduation. AB’s family had 4 members including his parents and one elder sister. As reported by his family, he was never so involved in the family was very shy and hesitant as a child. Also would hardly share his feelings or thoughts with them. After his family left, AB reports that he felt lonely and there was no one around so he started making friends online.
He met a person through social media groups and started meeting him on regular basis soon he became his closest friend and AB offered him to live together in his apartment. His friend was a chain smoker and also consumed other substances. At one of the parties organized by both of them his friend insisted AB try “black paste” (opium paste). AB reports that he wasn’t thinking too much and went ahead trying it. He reported that it made him relaxed, feels good about himself, and was comfortable during conversations throughout the party. Also, He reported being drawn towards it and wanted to consume it again. Initially, for few months, he was doing it occasionally (0.3-0.5gms) with his friend (twice or thrice a month). Later he was very overwhelmed by it and escalated to consuming it on weekly basis. He became irregular to college and had low attendance during his 2nd semester. He reported about his increased smoking too (10-13 cigarettes in a day). He would constantly ask for money from his parents for other excuses and would buy opium paste. He then on daily basis started consuming opium paste 3 times (after waking up, afternoon and before going to bed) a day with soft drinks (0.5 grams at a time). He was consuming 1.5 grams a day. He reported no irritability or bodily discomfort due to the consumption of opium paste. This continued for more than a year. His family was completely unaware and due to the work restrictions couldn’t visit Delhi often. AB reported that the opium paste would cost him a lot and that he started feeling extremely guilty about his dependence and how dysfunctional he becomes if he tried to cut down the dose. He did repeat attempts to cut down or quit but would fail every time due to horrifying withdrawal symptoms (tremors in the hand, hot and cold flushes, increased heart rate, restlessness, decreased appetite, increased craving, and inability to sleep, irritability and eventually would feel low). In the meantime, he asked his friend to move out so that he could finally be by himself and study for his end semester exams. He scored very low and failed in 3 subjects. It was then that his college communicated with his parents and asked them to meet. His parents immediately came to Delhi and seeing AB in the worst of his health and living conditions asked him what was wrong. He then confronted them about using opium paste for about 2 years and that he was unable to quit and how he felt emotionally and mentally withered. His parents were completely shocked and scared. They immediately approached AB’s treatment in Delhi itself.
The present case came to a psychiatric centre in West Delhi (September 2019). His chief complaints included inability to cut down the use of the substance (opium paste), increased craving for the substance, experiencing withdrawal symptoms and low mood. He did not feel self-confident because of his academic failure and repeating a year The client reported first consumption of opioid at the age of 21 years. He repeatedly missed college because of withdrawal symptoms (sweating, trouble sleeping, agitation, anxiety). AB stated that his last intake of opioid was 4 days before the day of the appointment
Mental Status Examination
The patient was kept and tidy, maintained eye contact and was in touch with the surroundings. The attitude was cooperative, attention was aroused and sustained. The speech was relevant, coherent and goal-directed with normal reaction time. Affect was congruent and appropriate. Cognitive functions were intact (memory, attention, orientation, intelligence). No thought or perceptual abnormalities were found. Personal and Social Judgment were partially intact, was at the preparation stage of motivation with insight grade level 4 (awareness of being sick, due to dysfunctional unknown self traits).
Behavioural Observation
The patient had a positive attitude towards the examiner and the assessment procedure. He was cooperative and showed interest during the assessment. He faced no problem in understanding and responding to the test items. He was comfortable and was curious to know the results.
Assessment
A preliminary clinical interview by a senior psychiatrist was conducted to confirm the diagnosis of opioid dependence disorder as per ICD-10 (DCR)14 and to evaluate the presence of other psychiatric disorders to support the reliability of assessment procedures and intervention. The present case study was approved by the Institutional Ethical Committee of Shree Guru Gobind Singh Tricentenary University (SGTU/FBSC/ECA/2020/08). Before starting the therapeutic intervention, the baseline assessment was done using valid and reliable tools- the severity of dependence scale (SDS),15 Brief-Cope Questionnaire,16 Emotional Regulation Questionnaire (ERQ)17 and Interpersonal Competence Questionnaire-15 (ICQ-15).18The assessment was done pre and post-intervention to check for effectiveness of DBT for opioid dependence. Mental status examination and behavioural assessment were done by the therapist.
RATIONALE OF THERAPY:
AB was treated using DBT- According to which the patient required a revised atmosphere in which emotions are controlled, interpersonal disputes are treated, discomfort tolerated and equilibrium is sought.
Goals of the therapy:
-
To create awareness and understanding about the illness.
-
Reducing the severity of dependence on opioid consumption.
-
Enhancing coping skills, emotion regulation and interpersonal competence/skills.
Detailed Therapy:
DBT was planned in the sequence of sessions19 as mentioned in Table 1. The duration of each session held was for 1hr 15mins. The sessions were conducted twice a week by the therapist.
-
Oral opioid substitution therapy consisted of the following medicine list- Tramadol, Tapentadol, Buprenorphine, Benzodiazepine, Clonidine.
-
Intravenous drip (IV) consists of DNS (dextrose and sodium chloride) for electrolyte correction and prevents dehydration caused due to absence of opioids
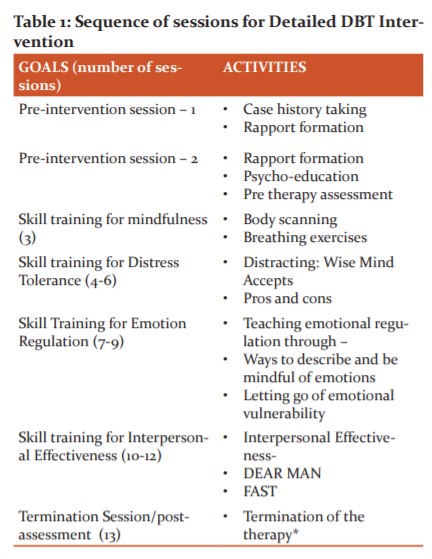
*Termination phase included- the summarization about the previous sessions, reviewing the progress, post-assessment and feedback from the patient.
Once the plan for structuring DBT within a training set was determined, the therapist and AB discussed his most prominent concerns to agree for DBT intervention, which included thoughts of substance use and explored how DBT could potentially address these problems. Consistent with DBT, AB was asked to commit to 10 weeks of therapy, as this would allow for sufficient time to work on the complex behaviours and skills deficits often seen with these types of clients. AB also was expected to attend 60- to 90-min individual sessions which were supervised by a clinical psychologist with extensive training and experience in DBT. The sessions were conducted twice in a week (13 individual sessions). AB could contact the therapist in between sessions and informed therapists would respond back as quickly as possible. Other measures were used to assess his general physical health, which he reported was fair and denied any chronic health conditions. The whole package, activities and procedures were chosen from skill repertories of the DBT skill training manual.19 Best efforts were retained to keep AB involved and attain the best of his capabilities. Following the hierarchy of treatment targets consistent with DBT, life-interfering behaviours were targeted first (e.g. reducing episodes of heavy substance use), followed by therapy-interfering behaviours (e.g. not doing homework, missing sessions), and then followed by quality of life-related behaviours (e.g. further reducing emotional impulsivity, initiating new relationships)
The mindfulness module was introduced first and the content was reviewed each time AB completed other modules or when he had taken an extended break from therapy. Additionally, he began each session with a brief mindfulness exercise (e.g. spending 10 min observing the sensations of their footsteps during a walk around the clinic or practising a body scan) to calm down, focus on the session and strengthen those skills.
The second was the distress tolerance module to provide AB with a set of coping skills via distraction techniques (WISE MIND ACCEPTS) to help him deal with physical and emotional pain caused by the urges to consume the substance. To increase his use of skills, AB frequently relied on skills such as pros and cons lists of using substances versus skills, focusing on the senses and distraction to manage physiological cravings or acutely distressing situations.
The third module emotional regulation was introduced to help AB develop effective skills to identify emotions and be mindful of them in different settings. He was asked to practice labelling his emotions in terms of thoughts and physiological responses. The intent was to train him to modify his responses and let go of his emotional vulnerabilities towards unhealthy behavioural patterns.
AB was most enthused to learn about the fourth module interpersonal effectiveness because these skills were likely to help him achieve many quality of life-related goals, such as building new relationships and sustaining them. The module focused on the need for effective interpersonal relationships and how to develop the skillset to sustain them. Assertive communication skills (DEAR MAN) were introduced as he would find it extremely hard to say “NO” to situations or people that can be damaging. One of his chief complaints was that he did not feel self-confident because of his academic failure and repeating a year again. In order to help with specific goal DBT technique (FAST) was used and practised very thoroughly.
DISCUSSION-
Given the complexity of this case and the fact that the client was treated within a training clinic, there are implications from this case study. Supervision and support from the therapists was a critical component that contributed to the success of this case. The therapist acknowledged feelings of anger and frustration as fluctuations in the clients’ functioning and substance use. Also was dedicated to being available for consultation during evenings and weekends. The sessions were meticulously planned before achieving the set goals with appropriate techniques.9,10 The different skills were delivered by the therapist using different methods like charts, diagrams, and role play. AB was highly interested in the mindfulness module as it would calm his impulses and frustration; make him more focused inside and out of sessions. At the start of the intervention, AB was smoking 7-9 cigarettes per day; however, toward later in therapy he consciously cut down it to 3-4 in a day. It was difficult for him to learn and be handy with distress tolerance skills but with constant practice, he managed to use them in divergent stress-provoking situations. These skills set improved his tolerance, enhanced his coping (scores improved from 76 to 80 on the brief cope questionnaire) also helped him effectively deal with situations rather than consuming opium and avoiding them. AB showed a significant reduction in opium intake on SDS (severity of dependence scale) from 13 to 10. Similar results have been seen in a Randomized clinical trial.10 Emotion regulation module took a great deal of time for him to understand the dialectics of emotions in everyday life. At times, AB expressed frustration with learning the skills for this module as he felt dumb for not already knowing these skills and these thoughts were complex and questioning to him shown to increase the likelihood that he would use substances rather than skills. In response to this challenge, it was helpful to discuss the dialectic of acceptance versus change. Specifically, it was helpful to explore both acceptance of why and how he did not already have the knowledge and the changes that he was making through treatment (When you’ve been able to use skills rather than substances, you tend to feel better in the long term). The viewpoint that substance abusers have difficulties regulating their emotions, and that negative emotional states precipitate substance use, is supported by a large body of empirical evidence.10 As per AB’s score on ERQ (emotion regulation questionnaire) the cognitive reappraisal subscale showed improvement of 3 points as AB was now better able to understand and interpret the intense emotion-provoking situation and act accordingly. There was a reduction in the Emotional suppression subscale which shows that AB got more comfortable in expressing and acknowledging his emotions. He realized the importance of maintaining a healthy daily routine for better emotional health. Similar results were shown in study 20 wherein “emotion regulation training (DBT) proved more effective than cognitive therapy, increasing distress tolerance and emotional regulation enhancement”
Relationships can become strained under the weight of addiction. Families, relationships and work often suffer as the person finds taking drugs as a priority above everything else. Interpersonal competence skill training was one of the key reasons for him to seek intervention. Initiating communication had always been a tough aspect of his entire childhood as well as his teenage life due to which he would either be left isolated or drawn towards unhealthy patterns. He learned that respecting oneself is equally important for him to form and sustain healthy relationships with others. He showed significant improvement on all 5 subscales of the interpersonal competence questionnaire (initiation, negative assertion, providing emotional support, disclosure about self and managing conflict). Ongoing assessment and self-monitoring were critical for this case. Throughout therapy, AB completed weekly assessments of overall functioning along with random urine tests. Throughout therapy, he was able to use skills more frequently and in increasingly difficult contexts, also maintained. The process prevented burnout, helped normalize common reactions and facilitated growth in case conceptualization and development of clinical skills for the training therapist as well.
This case study depicts the result of an individual patient, thereby restricting the generalization of findings. Further studies are recommended that will include a larger sample size, controlled socio-economic and demographic conditions while assessing different points of follow up. The application of DBT skill training can be also be extended towards the other major factors that significantly affect the frequent relapses in opioid dependence disorder.
CONCLUSION
In the present case report, there was a significant reduction in opioid dependence level, increasing coping skills, better emotional regulation and interpersonal relationships with the help of DBT. It was evident from the improvement in his pre and post-therapy scores. Thus it can be concluded that DBT offers the structure, strength, and compassion needed to enhance overall functioning and quality of life. It seems that DBT skill training given along with pharmacotherapy increase the effectiveness of treatment concerning substance dependence problem.
AUTHOR’S CONTRIBUTION
Komal Sancheti: Main author of research including planning, intervention and analysis. Dr. Nandha Kumara Pujam: Guidance in design, objectives, analysis and discussion as well as the final presentation. Dr. Nandha Kumara Pujam: is the guarantor for this paper.
COMPLIANCE WITH ETHICAL STANDARDS
Conflict of Interest- Nil
Financial support – nil
ACKNOWLEDGEMENT: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
-
Crocq MA. Historical and cultural aspects of man's relationship with addictive drugs. Dialogues Clin Neurosci. 2007;9(4):355-361.
-
United Nations Office on Drugs and Crime. South Asia Regional Profile. India: United Nations Office on Drugs and Crime. 2005. Available from: https://www.unodc.org/pdf/india/publications/south_Asia_Regional_Profile_Sept_2005/10_india.pdf. [Accessed on September 13, 2020].
-
Ray R. Ministry of Social Justice and Empowerment, Government of India and United Nations Office on Drugs and Crime. The extent, pattern and trends of drug abuse in India-National survey. 2004. Available from: www.unodc.org/India/Indianationalsurvey 2004.html. [Accessed on September 13, 2020].
-
Kermode M, Crofts N, Kumar MS, Dorabjee J. Opioid substitution therapy in resource-poor settings. Bull World Hea Org. 2011;89:243-243
-
Wittchen HU, Apelt SM, Soyka M, Gastpar M, Backlund M, Gölz J et al. Feasibility and outcome of substitution treatment of heroin-dependent patients in specialized substitution centres and primary care facilities in Germany: a naturalistic study in 2694 patients. Drug Alc Depend. 2008; 95(3):245-257.
-
Ambekar A, Goyal S. Clinical practice guidelines (CPG) for the management of opioid use disorders. In: Basu D, Dalal PK, editors. Clinical Practice Guidelines for the Assessment and Management of Substance use Disorders. Indian Psychiatric Society. 1st ed. Gurugram: Ind Psych Soc. 2014:157–262
-
Ambekar A, Rao R, Agrawal A, Kathiresan P. Research on opioid substitution therapy in India: A brief, narrative review. Ind J Psych. 2018;60(3):265-270.
-
Lawrinson P, Ali R, Buavirat A, Chiamwongpaet S, Dvoryak S, Habrat B et al. Key findings from the WHO collaborative study on substitution therapy for opioid dependence and HIV/AIDS. Addict. 2008; 103: 1484-92
-
Gowing L, Farrell M, Bornemann R, Sullivan LE, Ali R. Substitution treatment of injecting opioid users for prevention of HIV infection. Cochrane Database Syst Rev. 2008;2: CD004145
-
Dimeff LA, Linehan MM. Dialectical behaviour therapy for substance abusers. Addict Sci Clin Pract. 2008;4(2):39-47.
-
Linehan MM, Dimeff LA, Reynolds SK, Comtois KA, Welch SS, Heagerty P et al. Dialectical behaviour therapy versus comprehensive validation plus 12-step for the treatment of opioid-dependent women meeting criteria for borderline personality disorder. Drug Alcohol Depend. 2002; 67:13-26.
-
May JM, Richardi TM, Barth KS. Dialectical behaviour therapy as a treatment for borderline personality disorder. Ment Health Clin. 2016;6(2):62-67.
-
Lynch TR, Morse JQ, Mendelson T, Robins CJ. Dialectical behaviour therapy for depressed older adults: A randomized pilot study. Am J Geriatr Psychiatry. 2003; 11:33-45.
-
World Health Organization. The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. Geneva: World Health Organization. 1992
-
Gossop M, Best D, Marsden J, Strang J. Test-retest reliability of the Severity of Dependence Scale. Addict. 1997;92(3):353.
-
Mahmoud JS, Staten R, Hall LA, Lennie TA. The relationship among young adult college students' depression, anxiety, stress, demographics, life satisfaction, and coping styles. Issues Ment Health Nurs. 2012;33(3):149-56.
-
Gouveia VV, Moura de HM, Oliveira de ICV, Ribeiro MGC, Rezende, AT, Brito de TR. Emotional Regulation Questionnaire (ERQ): Evidence of Construct Validity and Internal Consistency. Psico-USF. 2018; 23(3): 461-471.
-
Coroiu A, Meyer A, Gomez-Garibello CA, Brähler E, Hessel A, Körner A. Brief form of the Interpersonal Competence Questionnaire (ICQ-15): Development and preliminary validation with a German population sample. Eur J Psychol Assess. 2015; 31(4):272–279.
-
Linehan MM. Diagnosis and treatment of mental disorders. Skills training manual for treating borderline personality disorder. New York. Guilford Press. 1993
-
Azizi A, Borjali A, Golzari M. The effectiveness of emotion regulation training and cognitive therapy on the emotional and addiction problems of substance abusers. Iran J Psych. 2010;5(2):60-5.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





