IJCRR - 13(13), July, 2021
Pages: 39-44
Date of Publication: 05-Jul-2021
Print Article
Download XML Download PDF
A Comparative Study of the Functional Outcome of Patellar Tendon Splitting and Medial Parapatellar Approaches in Intramedullary Interlocking Nailing of Tibia
Author: Sandesh V, Nagakumar JS, Sandesh Agarwal, B.S. Sheik Nazeer
Category: Healthcare
Abstract:Introduction: The \"fractures of the shaft\" of the tibia are the most common fractures among the long bone fracture. Various approaches to intramedullary nailing have been proposed. Pain in the anterior region of the knee is the very common complication of intramedullary nailing procedures. Although all techniques for nail insertion have been proven feasible, a correlation of Pain in the anterior region of the knee and functional outcome is lacking between the trans patellar and medial parapatellar techniques. Aim: To compare functional outcome in both the approaches of trans patellar and medial parapatellar techniques for the tibial fracture treatment. Materials and Methodology: After a detailed clinical examination & detailed history were taken among 60 subjects divided into two groups of splitting and sparring groups. Between two groups compared to age, sex, cause of the injury, \"open/ closed types of injury\", side of injury, time of union, anterior knee pain, range of motion. Results: No statistically significant values were observed among the two groups when the age, sex, mode of injury, sides, type of injury, time of union were compared. Statistically significant values were observed when the anterior knee pain, range of mo�tion were compared between the group. Conclusion: Medial parapatellar technique was efficient in treating the tibial fracture than the trans patellar splitting technique in the present study.
Keywords: Medial parapatellar, Trans patellar, Intramedullary interlocking, Tendon splitting, Nailing of the tibia
Full Text:
INTRODUCTION:
The tibia is exposed to frequent injury, thereby being the most commonly fractured long bone. Because one-third of the tibial surface is subcutaneous all through its “length” and it also has a precarious blood supply than other bones, which are enclosed by bulky muscles.1
Tibial shaft fractures are the most common fractures encountered among young aged people.2 Fractures of the tibia are amid the most popular “long bone fractures” because of their potential for nonunion, malunion and propensity for their open injury.2 For the treatment of diaphyseal tibial fractures, tibial nailing has become the standard care as intramedullary nail acts as an internal splint.1
The intramedullary nail is used to treat diaphyseal fractures of the tibia commonly. The infrapatellar approach is the most commonly used. Hyperflexion of the knee during the procedure may however increase the risk of valgus and procurator deformities in proximal third tibial shaft fractures. To address this problem, a semi- extended technique has been developed,3 of which also a subcutaneous variant exists.4 For the same reasons, the suprapatellar approach has been introduced.5,6 For this approach, an incision is made just proximal to the superior pole of the patella and the nail is inserted through the patellofemoral joint. Few clinical studies have suggested favourable outcomes associated with a suprapatellar approach.5,6,7
The potential damage to the cartilage of the patellofemoral joint remains a significant drawback, although rates of anterior knee pain following this procedure seem lower than seen after the infrapatellar approach.6,7 Infra patellar approaches have gained more importance due to the drawbacks of the suprapatellar approach. Even though all nail insertion techniques have been proven feasible, a contrast of the rates of pain in the anterior part of the knee and functional outcome is lacking. The present study aimed to analyze functional outcome in both the approaches and prevalence of fracture malalignment and study the incidence of anterior knee pain in both approaches, according to Waters and Bentley scoring.
MATERIAL AND METHODS:
This study was a prospective comparative study conducted in the department of orthopaedics at R.L.J. Hospital and research centre, attached to Sri Devaraj Urs Medical College, Tamaka, Kolar. The sample size was estimated based on the functional outcome between the medial parapatellar approach versus the patellar tendon splitting approach. A study by Sadeghpour et al.8 observed a difference of 30% in the functional outcome of excellent, expecting a 40% difference in excellent functional outcome between the methods in the present study with a 95% confidence interval with the power of 80%. The required sample size per group was 30. So, the final sample size was 60. The data collection for the study was done between September 2018 to June 2020. The study population included patients age more than 18 years, closed tibia shaft fracture, Open type I, II tibial diaphyseal fracture, Segmental tibial fractures. Exclusion criteria included Pathological fractures, Tibial shaft fractures with intraarticular extension, previous history of knee surgery, knee osteoarthritis. The study was approved by the institutional human ethics committee. Informed written consent was obtained from all the study participants, and only those participants willing to sign the informed consent were included in our study.
Methodology:
A sample of size 60 was selected using the purposive sampling technique based on inclusion and exclusion criteria. Patients were randomized into two groups with odd and even. Group A was undergoing a medial parapatellar approach (30 patients). Group B was undergoing a patellar tendon splitting approach (30 patients). All patients were evaluated by detailed history about the trauma, mode of injury and detailed clinical examination. Pre-Op Evaluation: The fractures were classified by the method of AO classification and GUSTILO ANDERSON classification for open fractures. Post Op Pain Evaluation: It is based on Waters and Bentley scoring.The clinical anterior knee pain rating system described by Waters and Bentley. The patient is called for periodic follow up on day 1, day 7, 1 month and 6months. Routine Investigations for Surgical Procedure were carried out. The radiological investigation included an X-ray of the leg with knee and ankle – AP and lateral view. Blood Investigations: CBC, BT, CT, Blood grouping, Renal function tests, Liver function tests (if required), RBS, FBS/PPBS, HbA1C (If required), HIV, HBsAg, serum electrolytes.
Statistical Methods:
Anterior knee pain and range of movements were assessed on 1st day, one week, one month, six months and was considered as primary outcome variables. Age, gender, mode of injury, etc., were considered as other study relevant variables. Study Group (Sparring v/s Splitting) was considered as an explanatory variable. Shapiro wilk test p-value of >0.05 was considered as a normal distribution. For normally distributed Quantitative parameters, the mean values were compared between study groups using an independent sample t-test (2 groups). Categorical outcomes were compared between study groups using the Chi-square test. Data was also represented using clustered bar charts and error bar chart. P-value < 0.05 was considered statistically significant. IBM SPSS version 22 was used for statistical analysis.9
Results:
A total of 60 participants were included in the final analysis with 30 participants in the sparring and splitting group.
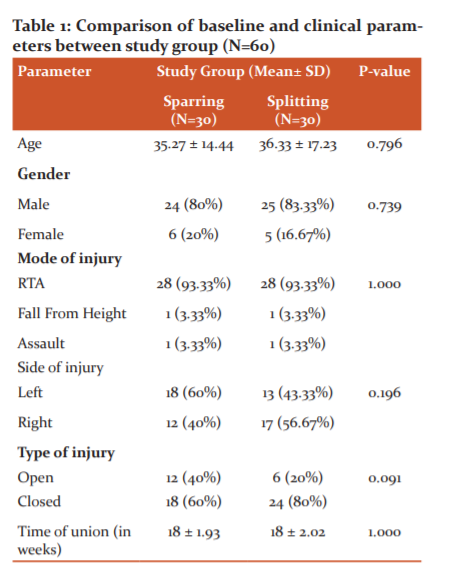
The difference in baseline parameters like age and gender and clinical parameters like mode of injury, side of injury, type of injury and time in the union between the study group was not statistically significant (P Value>0.05). (Table 1)
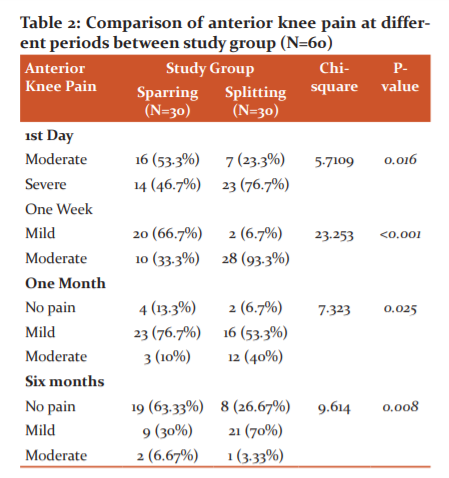
The difference in the proportion of anterior knee pain at 1st day, one week, one month and six months between the study group were statistically significant (P Value<0.05). (Table 2 and 3)
DISCUSSION:
Nailing of the tibia is the choice of treatment due to the reasons of sharing of physiologic loads, intramedullary position & allowing weight-bearing of affected extremity immediately after placement.10 However pain in the anterior part of the knee is the most commonly reported complication that has been associated with the tibial plateau width, fracture type, nail prominence, fracture union, socio-demographics, time after surgery, infrapatellar fat lesion, entry point location and intra articular structure injury, location and size of the scar.11Some associate the iatrogenic injuries to the infrapatellar branch of the saphenous nerve as the reason for the anterior knee pain.12 Nowadays, closed methods have superseded the old methods of open surgeries.13 Literature points to the medial parapatellar incision being safer as compared to the trans patellar approach for intramedullary interlocking nail insertion.8,14
In the study, Anterior knee pain at 1st day, 7 days, 30 days, six months and range of movements at 1st day, 7 days, 30 days, six months was considered as primary outcome variables. Age, gender, mode of delivery, etc., were considered as other study relevant variables. Study Group (Sparring v/s Splitting) was considered as an explanatory variable. The present study is comparable with the study of Bakhsh et al.15 (2016)Song et al.16( 2012)Sadeghpour et al.17 (2011).
A study reported incidence rates of metaphyseal ankle fractures that varied considerably by age and gender. Incidence ranged from a low of 3 per 10,000 per year among 30 to 34-year-old women to a high of 28 per 10,000 per year among 15 to 19-year-old boys.18
Clinical Variables:
Mode of injury and the side affected: Most commonly, the Tibial fractures are caused due to road traffic accidents, sports injuries; a gunshot injury, direct trauma, fall from height. The prognosis depends upon the soft tissue injury status. It is sufficient to say here that the higher the velocity of the trauma, the more association of the presence of major soft tissue damage. In the present study, a similar observation was made with “majority sustaining an RTA”, in both the groups, however they were not statistically significant. Similar values were obtained in the study of Song et al.16 Sadeghpour et al.17 However, the majority of subjects in the study of Baksh et al15, where they sustained a fall though not significant. The difference in the proportion of right and left side of injury between the study group was not statistically significant (P Value>0.05). This is following the study of Vijay Baba et al.19
Type of injury: The exposed anatomical location of the tibia makes it vulnerable to direct blow and high energy trauma as a result of motor vehicle accidents thus resulting in comminuted fractures, which are frequently open with significant loss of skin and soft tissues. In contrast to the rest of the” appendicular skeleton, tibia has precarious blood supply due to inadequate muscular envelope”. When the type of injury was compared between the study group in the sparring group, the majority had open than closed injury, while the reverse was true in the splitting group, though the difference in the proportion of the type of injury between groups was not statistically significant. This is in comparison with the study of Sadeghpour et al17, and Bakshet al.15 In these studies, the closed injuries superseded the open injuries, though not statistically significant. Attention must be paid to the soft tissue. Because the bone is subcutaneous, a closed fracture can easily become an open fracture, as the bone spikes through the skin. In addition, bleeding or swelling in the soft tissues can increase the interstitial pressure and block blood flow, leading to ischemic necrosis of muscle or nerve, i.e., compartment syndrome.
Anterior knee pain incidence: In the Tibial fracture treatments, anterior knee pain is the most commonly reported complication with an incidence of about 18%-86%. The cause of this pain is multifactorial like tibial plateau width, fracture type, nail prominence, fracture union, sociodemographic, time after surgery, infrapatellar fat lesion, entry point location and intra articular structure injury, location and size of the scar.11 Iatrogenic injuries to the infrapatellar branch of the saphenous nerve are also believed to be the cause of anterior knee pain.12 The nail designs may also have been implicated in injuring the proximal tibiofibular joint and cause knee pain.20On Comparison of anterior knee pain at different periods between study group the severity of the pain reduced with the time in both the groups. However, the sparring group showed less severity to the pain than the splitting group. This shows a better efficacy of the sparring procedure than the splitting method. The difference in the proportion of anterior knee pain at 1st day, 1st week, one month and six months between the study group was statistically significant (P Value<0.05). This is in comparison with the study of Sadeghpour et al.17 where they also observed a similar significant reduction of pain between the two groups at 3 and 6 months. In a prospective clinical study including 56 patients undergoing suprapatellar tibial nailing in the semi extended position, Sanders et al6, did not report any significant sequelae affecting the patellofemoral cartilage as per Magnetic Resonance Imaging and arthroscopic follow-up evaluations. Interestingly, none of the patients in the series complained of anterior knee pain at the 12 months follow-up. In a retrospective cohort study, Jones et al.5 recorded the outcomes of 38 patients undergoing suprapatellar nailing in the semi extended position versus 36 patients undergoing infrapatellar nailing. These authors reported no differences in anterior knee pain and no functional differences between the two patient groups at a minimum of 12 months follow-up.
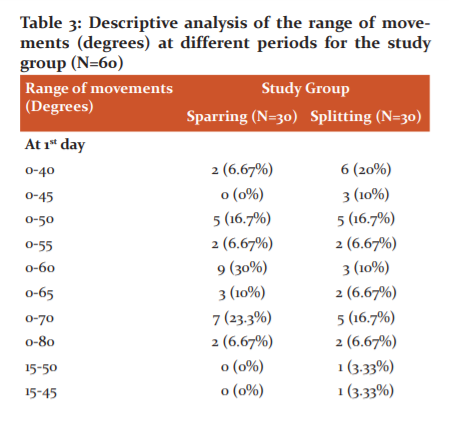
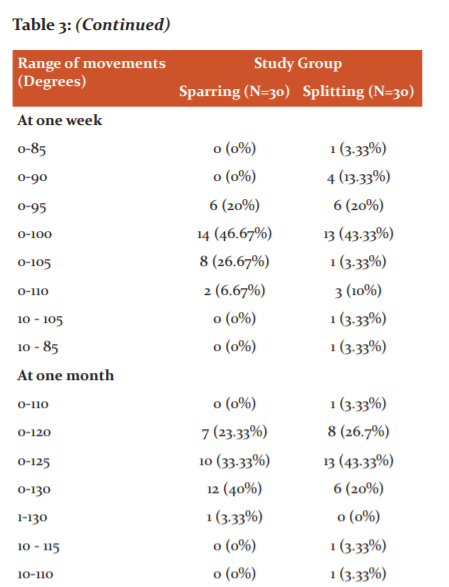
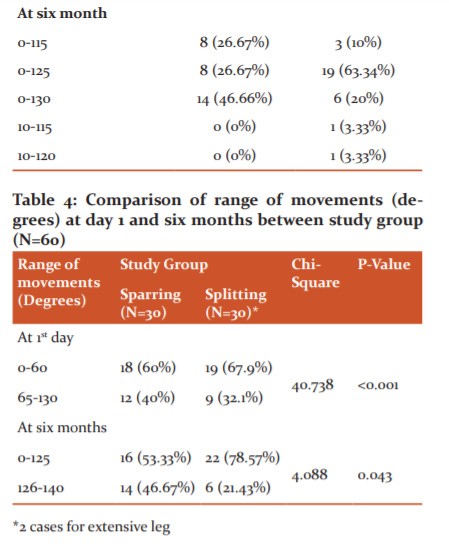
Range of Movements: One of the essential aspects of closed reduction and internal fixation with interlocking intramedullary nailing is the ability to mobilize the patient early. The descriptive analysis of a range of movements (degrees) at different periods for the study group showed that the medial parapatellar technique had a greater ROM than the splitting method. Comparing the range of movements (degrees) at day 1, day 7,1 month, 6 months between the study group was statistically significant. (P Value<0.05)
Time for union: Union occurring after 20 weeks was classified as a delayed union. Non-union was defined as a union not having taken place with radiological evidence that the fracture union process had ceased. Among the study population, the time of union was 18 ± 1.93 weeks in the sparring group and 18 ± 2.02 weeks in the splitting group. The difference in the meantime of union between the study group was not statistically significant (P Value>0.05). This is similar to the study of O'Dwyer et al.21, where the time of union was 15 weeks. Vijay Baba et al.19 in their prospective study observed that the time to union ranged from 12 to 32 weeks with an average of 20 weeks.
In our study, out of the 60 patients, 3 patients developed surgical site infection, which was treated with sensitive antibiotics after culture and sensitivity were obtained. One patient with open type fracture developed an infection which was treated by serial debridement and vacuum dressing, and two patients had an extensor lag of 15 degrees initially, and it was observed that at six months they had 10 degrees of extensor lag.
COMPLICATIONS:
In our study, out of the 60 patients, 3 patients developed surgical site infection, which was treated with sensitive antibiotics after culture and sensitivity were obtained. One patient with open type fracture developed an infection which was treated by serial debridement and vacuum dressing, and two patients had an extensor lag of 15 degrees initially, and it was observed that at six months they had 10 degrees of extensor lag.
CONCLUSIONS:
This prospective study with 60 subjects with a mean age of 36 years had the majority of male participants. The majority of our study participants in both groups had encountered tibial fracture due to road traffic accident. When compared between the 2 methods of approach for management of tibial fractures, we found a medial patellar approach to be better than trans- patellar. There was a significant reduction of pain along an improved range of movement in the medial patellar group was significant compared to the trans-patellar group. Hence our study results conclude, medial patellar approach to be better than trans patellar with a better outcome comparatively.
References:
1. Toivanen JAK, Väistö O, Kannus P, Latvala K, Honkonen SE, Järvinen MJ. Anterior knee pain after intramedullary nailing of fractures of the tibial shaft. A prospective, randomized study comparing two different nail-insertion techniques. J Bone Joint Surg Am. 2002 Apr;84(4):580–5.
2. Anubhav R, Rajan A. Comparision of transpatellar and medial parapatellar tendon approach in tibial intramedullary nailing for the treatment of fracture shaft of the tibia. Open J Orthop Rheumatol. 2020 Jan 28;5(1):001–5.
3. Kubiak EN, Widmer BJ, Horwitz DS. Extra-articular technique for semi extended tibial nailing. J Orthop Trauma. 2010 Nov;24(11):704–8.
4. Leliveld MS, Verhofstad MHJ, Bodegraven E Van, Haaren J Van, Lieshout EMM Van. Anterior knee pain and functional outcome following different surgical techniques for tibial nailing?: a systematic review. Eur J Trauma Emerg Surg. 2020;(0123456789).
5. Jones M, Parry M, Whitehouse M, Mitchell S. Radiologic outcome and patient-reported function after intramedullary nailing: a comparison of the retropatellar and infrapatellar approach. J Orthop Trauma. 2014 May;28(5):256–62.
6. Sanders RW, DiPasquale TG, Jordan CJ, Arrington JA, Sagi HC. Semiextended intramedullary nailing of the tibia using a suprapatellar approach: radiographic results and clinical outcomes at a minimum of 12 months follow-up. J Orthop Trauma. 2014 May;28(5):245–55.
7. Chan DS, Serrano-Riera R, Griffing R, Steverson B, Infante A, Watson D, et al. Suprapatellar Versus Infrapatellar Tibial Nail Insertion: A Prospective Randomized Control Pilot Study. J Orthop Trauma. 2016 Mar;30(3):130–4.
8. Sadeghpour A, Mansour R, Aghdam HA, Goldust M. Comparison of trans patellar approach and medial parapatellar tendon approach in tibial intramedullary nailing for the treatment of tibial fractures. J Pak Med Assoc. 2011 Jun;61(6):530–3.
9. IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.
10. Gaines RJ, Rockwood J, Garland J, Ellingson C, Demaio M. Comparison of insertional trauma between suprapatellar and infrapatellar portals for tibial nailing. Orthopaedics. 2013 Sep;36(9):e1155-8.
11. Jankovic A, Korac Z, Bozic N-B, Schedule I. Influence of knee flexion and atraumatic mobilisation of the infrapatellar fat pad on incidence and severity of anterior knee pain after tibial nailing. Injury. 2013 Sep;44 Suppl 3:S33-9.
12. Leliveld MS, Verhofstad MHJ. Injury to the infrapatellar branch of the saphenous nerve, a possible cause for anterior knee pain after tibial nailing? Injury. 2012 Jun;43(6):779–83.
13. Bong MR, Koval KJ, Egol KA. The history of intramedullary nailing. Bull NYU Hosp Jt Dis. 2006;64(3–4):94–7.
14. Ahmad S, Ahmed A, Khan L, Javed S, Ahmed N, Aziz A. Comparative Analysis Of Anterior Knee Pain In Transpatellar And Medial Parapatellar Tendon Approaches In Tibial Interlocking Nailing. J Ayub Med Coll Abbottabad. 2016;28(4):694–7.
15. Bakhsh WR, Cherney SM, McAndrew CM, Ricci WM, Gardner MJ. Surgical approaches to intramedullary nailing of the tibia: Comparative analysis of knee pain and functional outcomes. Injury. 2016;47(4):958–61.
16. Song SY, Chang HG, Byun JC, Kim TY. Anterior knee pain after tibial intramedullary nailing using a medial paratendinous approach. J Orthop Trauma. 2012;26(3):172–7.
17. Sadeghpour A, Mansour R, Aghdam HA, Goldust M. Comparison of trans patellar approach and medial parapatellar tendon approach in tibial intramedullary nailing for the treatment of tibial fractures. J Pak Med Assoc. 2011;61(6):530–3.
18. Shanmuganathan DK, Sounderrajan DD. Evaluation of clinical and functional outcome of internal fixation with intramedullary interlocking nailing with ‘Poller’ blocking screws in tibial metaphyseal fractures. Int J Orthop Sci. 2020;6(1):573–7.
19. N VB, Arumugam B. Interlocked Intramedullary Nailing in the Management of Closed Diaphyseal Fractures of Tibia- A Prospective Analysis. Int J Cont Med Res. 2016;3(7):1987–91.
20. Laidlaw MS, Ehmer N, Matityahu A. Proximal tibiofibular joint pain after insertion of a tibial intramedullary nail: two case reports with accompanying computed tomography and cadaveric studies. J Orthop Trauma. 2010 Jun;24(6):e58-64.
21. O’Dwyer A, Chakravarty RD ECI nailing technique and its effect on union rates of tibial shaft fracture. Injury. 1994 Sep;25(7):461-4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





