IJCRR - 13(12), June, 2021
Pages: 193-196
Date of Publication: 22-Jun-2021
Print Article
Download XML Download PDF
Effectiveness of Fluoroscopy-Guided Genicular Nerve Radiofrequency Ablation in the Management of Chronic Osteoarthritis of Knee: A Prospective Study
Author: Sahu SK, Pandey A, Dash A
Category: Healthcare
Abstract:Introduction: Chronic osteoarthritis of the knee is a frequently encountered painful condition in the elderly and requires an astute approach for its treatment. The etiologies of chronic osteoarthritis are multiple:-age, obesity, hereditary, female preponderance, the association of diseases such as thyroid disorder, rheumatoid arthritis increases the risk significantly. Objective: The effectiveness of nonsurgical options in providing pain relief and functional improvement is generally inadequate. Method: Inclusion criteria:- No response to conservative management for a minimum of 3 months. Tibia femoral osteoarthritis (Kellgren-Lawrence) grade 3-4 on radiological evaluation. Exclusion criteria: Acute knee pain, Prior knee surgery, Patients on anticoagulant medications, psychiatric illness, Steroid/ Hyaluronic injections taken in the past 3 months. Result: The pain intensity was much lower post block when compared to baseline pre-procedure values of both the indices throughout 6 months follow up. The patient's painless standing/mobility period also increased significantly after injection as it was before the procedure. Conclusion: Notable heterogeneity (p < 0.001) was noticed and concluded the Funnel Plot. In our result, it was observed that the age group 30-39 had a significantly higher mortality rate.
Keywords: Chronic osteoarthritis of knee, Genicular nerve, Radiofrequency ablation, Visual analogue score, Oxford knee score
Full Text:
INTRODUCTION
Chronic osteoarthritis of the knee is a chronic debilitating and troublesome condition in the elderly which results in a significant amount of pain in joints causing limitation of function and day to day activities.1 Many modalities of treatment are available, such as pharmacological and surgical. However, surgical management is the most definitive treatment for chronic osteoarthritis.2 The effectiveness of nonsurgical options in providing pain relief and functional improvement is generally inadequate. Genicular nerve radiofrequency ablation, which was introduced by Choi et al. has given a new dimension for the treatment of chronic osteoarthritis because it is a minimally invasive method being done as a daycare procedure and the patient can be discharged after a brief period of observation for possible post-procedural complications.3-7 The procedure targets chiefly the three nerves supplying the knee joint:-Superomedial genicular nerve(SMGN), Superolateral genicular nerve (SLGN) and Inferomedialgenicular nerve(IMGN). Good relief has been observed with this procedure with significant improvement in the functional well being of the patient for up to 12-15 weeks. If the recent literature is to be followed, studies suggest that GNB (Genicular Nerve Blocks) could be an apt treatment option for patients unwilling to undergo surgery or who are not fit for knee arthroplasty.VAS (visual analogue scale) and OKS (oxford knee score) are commonly used parameters to evaluate the degree of disability and estimate the quality of life of having chronic knee pain.
MATERIALS AND METHODS
This is a prospective study done at IMS and SUM Hospital, Bhubaneswar. We have included 30 patients having chronic osteoarthritis of the knee. The duration of this study was 2 years (2018-2020). The patients were of the age group 50-70 years who had pain around the knees, failing conservative management or were not suitable candidates for surgery or were unwilling to undergo knee arthroplasty. IMS-SH/SOA/16089.
Inclusion criteria:-
1. No response to conservative management for a minimum of 3 months.
2. Tibiofemoral osteoarthritis (Kellgren-Lawrence) grade 3-4 on radiological evaluation.
Exclusion criteria:-
1. Acute knee pain.
2. Prior knee surgery.
3. Patients on anticoagulant medications, psychiatric illness.
4. Steroid/Hyaluronic injections taken in the past 3 months.
All patients underwent complete workup with all routine investigations to rule out any co-morbidities, infection and coagulation abnormalities. Analgesics were withdrawn in the post-procedure period. For all patients, an anteroposterior view of the knee (in standing position) and lateral view (in 45 degrees of flexion) was done and the radiological classification done as per the radiographic findings ( Table 1).
Procedure:-
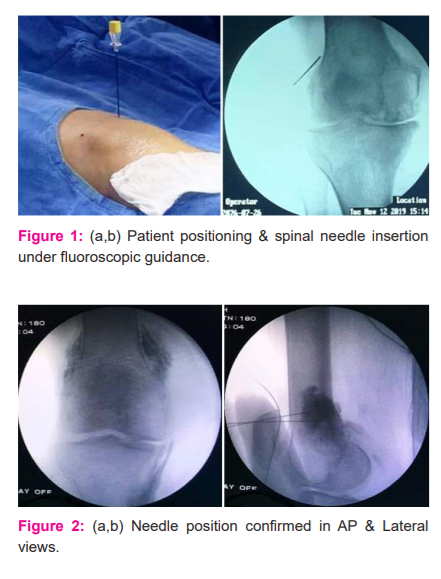
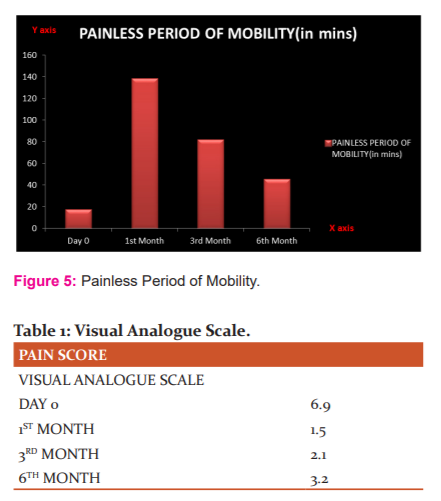
With the patient lying supine, the knee(s)were prepped and draped in the usual sterile fashion using a sterilized cloth drape[Fig1a]. The skin of the landmark areas was anaesthetized with Xylocard 2%, after confirming under fluoroscopy. A spinal needle (23G) was inserted over the junction of the femoral diaphysis and the medial femoral condyle, another needle was inserted to femoral diaphysis and the lateral femoral condyle junction [Fig1b], 3rd needle to the lateral tibial diaphysis and the medial tibial condyle. Placement of all needles was confirmed on lateral fluoroscopic view and the exact location for the point of injection was confirmed after injecting 0.5ml of Iopamidol(non-ionic contrast solution)in the lateral view to make sure, there is no intravascular extravasation [Fig2]. Asteroid mixture consisting of 2ml of 2% Xylocard, 2ml Triamcinolone acetonide(40 mg), 0.5ml (75 micrograms) of Clonidine hydrochloride and 5 ml of distilling water to make the mixture of 10 ml and was slowly injected at the three designated sites after a negative aspirate. Stryker system was used to ablate the genicular nerve at 50 degree Celsius for 60 seconds, following which the needle was withdrawn about 5mm and a second ablation was done. A sterile dressing was applied at the end of the procedure and the patient was observed for 2 hours post-procedure to make sure, that there were no post-procedure complications.
RESULTS
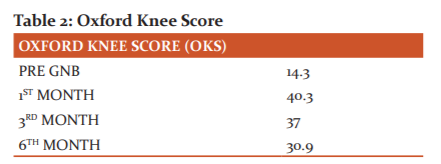
In our study, there were a total of 30 patients of which 18 were females and 12 were males with a mean age of individuals 66 years. Mean pain intensity as per visual analogue scale (VAS) in the pre-procedure phase was 6.9 and as per Oxford knee score (OKS), it was 14.3 (Figure 3, 4 and 5). The pain intensity was much lower post block when compared to baseline pre-procedure values of both the indices throughout 6 months follow up. The patient’s painless standing/mobility period also increased significantly after injection as it was before the procedure.
DISCUSSION
A review of the literature has shown that GNRFA may be an effective alternative for patients with knee osteoarthritis.14-17 The use of fluoroscopy device in performing nerve blocks can greatly increase the efficacy and precision, which in turn can significantly reduce the complications.8,9 Primarily, superolateral, superomedial and in feromedialgenicular nerves transverse along the areas connecting the shaft of the epicondyle, periosteally.10 Secondly, fluoroscopic imaging gives good visualization concerning tissue depth and needle gauge. Thirdly, as we are using contrast fluoroscopy, it can prevent unintentional intravascular injection.11 However, potential complications result after performing every diagnostic procedure. There are some common side effects such as leg muscle weakness, discomfort at the injection site. Other complications include vascular injuries, pseudoaneurysm, AVfistula, hemarthrosis, which are extremely rare but can carry potential morbidity.12 Many authors suggested that the effects of the block were indirect and acted via alterations in nociceptive processing and effect on the neuropathic brain pathway.13 Though genicular nerve radiofrequency ablation targets bony landmarks, it may be difficult to isolate the exact anatomic location of>1 of the genicular nerves18,19. The OKS and VAS scoring system gives us an assessment regarding the quality of life in chronic osteoarthritis patients which are seldom used in other studies. The success of this study is encouraging as evident by the improved pain scores on regular follow up. The patients, after the procedure, are encouraged to undergo physiotherapy sessions in the form of static quadriceps exercises to avoid any recurrences in pain. All the patients were also trained about the mobility process and the areas of work that they should avoid so that the effect of analgesia stays for a considerable amount of time (Table 2). Lifestyle modification is also a very important aspect in the management of chronic osteoarthritis which was judiciously promoted among the patients. However, this study had a limitation in that no control group was assigned for comparison.
CONCLUSION
This study demonstrates the long term effects of genicular nerve block under fluoroscopic guidance for patients with chronic osteoarthritis providing them with pain relief. The combination of the genicular nerve block with the addition of other rehabilitative measures extends the pain-free period significantly. In the light of the above study, a longer follows up time is required to assess the efficacy of a single time injection. In addition to the above fact, the frequency of repeat injections and their effectiveness in patients who do not have adequate pain relief demand more studies with larger sample size and a longer study period. For generating high-level evidence, larger studies with randomized control groups can be planned.
Acknowledgement: The authors are highly grateful to the Dean IMS & SUM Hospital for providing all the support during the study.
Conflict of interest: There is no conflict of interest among the authors.
Source of funding: Nil
Author’s Contribution: Santosh Kumar Sahu conceived, planned, designed and guided the study and drafted the manuscript. Abhishek Pandey collected the data. Aniruddh Dash processed the manuscript for final editing and drafting.

References:
1. Peat G, McCarney R, Croft P. Knee pain and osteoarthritis in older adults: A review of community burden and current use of primary health care. Ann Rheum Dis. 2001; 60:91-97.
2. Yu SP, Hunter DJ. Managing osteoarthritis. Aust Prescr. 2015; 38:115–119
3. Choi WJ, Hwang SJ, Song JG, Leem JG,Kang YU, Park PH, Shin JW. Radiofrequency treatment relieves chronic knee osteoarthritis pain: A double-blind randomized controlled trial. Pain. 2011;152: 481-487.
4. Kesikburun S, Yasar E, Uran A, Adiguzel E, Yilmaz B. Ultrasound-guided genicular nerve pulsed radiofrequency treatment for painful knee osteoarthritis: A preliminary report. Pain Physician. 2016;19:E751-E759.
5. McCormick ZL, Korn M, Reddy R, Marcolina A, Dayanim D, Mattie R, Cushman D, Bhave M, McCarthy RJ, Khan D, Nagpal G, Walega DR. Cooled radiofrequency ablation of the genicular nerves for chronic pain due to knee osteoarthritis: Six-month outcomes. Pain Med. 2017;18:1631-1641.
6. Protzman NM, Gyi J, Malhotra AD, Kooch JE. Examining the feasibility of radiofrequency treatment for chronic knee pain after total knee arthroplasty. Pain Med Res. 2014; 6:373-376.
7. Sari S, Aydin ON, Turan Y, Ozlulerden P, Efe U, Kurt Omurlu I. Which one is more effective for the clinical treatment of chronic pain in knee osteoarthritis: Radiofrequency neurotomy of the genicular nerves or intra-articular injection? Int J Rheum Dis. 2016;doi:10.1111/1756-185X.12925.
8. Roos EM, Nk A. Strategies for the prevention of knee osteoarthritis. Nat Rev Rheumatol. 2015;
9. Ucuncu F, Capkin E, Karkucak M, OzdenG, Cakirbay H, Tosun M, Guler MA. Comparison of the effectiveness of landmark guided injections and ultrasonography-guided injections for shoulder pain. Clin J Pain. 2009; 25:786-789.
10. Hoeber S, Aly AR, Ashworth N, RajasekaranS. Ultrasound-guided hip joint injections are more accurate than landmark-guided injections: A systematic review and meta-analysis. Br J Sports Med. 2016; 50:392-396.
11. Baker R, Dreyfuss P, Mercer S, BogdukN. Cervical transforaminal injection of corticosteroids into a radicular artery: A possible mechanism for spinal cord injury. Pain 2003; 103:211-215.
12. Kim SY, Le PU, Kosharskyy B, Kaye AD, Shaparin N, Downie SA. Is Genicular Nerve Radiofrequency Ablation Safe? A Literature Review and Anatomical Study. Pain Physician. 2016;
13. Afridi SK, Shields KG, Bhola R, GoadsbyPJ. Greater occipital nerve injection in primary headache syndromes—prolonged effects from a single injection. Pain.2006; 122:126-129.
14.Crawford DC, Miller LE, Block JE.Conservative management of symptomatic knee osteoarthritis: a flawed strategy? Orthop Rev(Pavia).2013.February 22:5(1):e2.
15.Kidd VD. Genicular nerve radiofrequency ablation: a novel approach to symptomatic knee osteoarthritis. JBJS JOPA.2018;6(1):e10.
16. Choi WJ,Hwang SJ,Song JG,Leem JG, Kang YU. Radiofrequency treatment relieves chronic knee osteoarthritis pain. Orthop Rev. 2011.March:152(3):481-7.
17. Iannaccone F, Dixon S, Kaufman A.A review of long term pain relief after genicular nerve radiofrequency ablation in chronic knee osteoarthritis. Pain Physician. 2017.March:20(3): E437-E444.
18. Iannaccone F, Le PU, Kim JH, Kim SY. Anatomical basis of genicular nerves: implication for RFA as a treatment for chronic knee pain. Presented as a poster exhibit at the 15th Annual Pain Medicine Meeting. Pain Physician. 2016; 11:17-19:
19. Orduna Valls JM, Vallejo R, Lopez Pais, Soto E, Torres Rodriguez D et al. Anatomic and USG evaluation of the knee sensory innervations: a cadaveric study to determine anatomic targets in the treatment of chronic pain. Reg Anesth Pain Med.2017;42(1):90-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





