IJCRR - 13(12), June, 2021
Pages: 179-182
Date of Publication: 22-Jun-2021
Print Article
Download XML Download PDF
Endocrown: An Approach Towards Management of Endodontically Treated Teeth -A Case Report
Author: Shanvi Agrawal, Seema Sathe Kambala, Dipak Manohar Shinde, Surekha Godbole Dubey
Category: Healthcare
Abstract:Introduction: Endocrowns are considered a viable option for the restoration of posterior endodontically treated and badly destructed teeth. When compared with conventional post & core crowns, the procedure involving the endocrown fabrication is considered more practical, less complex & easy to perform. Aims: To manage extensively damaged posterior teeth with a PFM based endocrown type of restoration. Methodology: This case report describes the management of extensively damaged endodontically treated posterior teeth, with endocrown-type restorations fabricated with metal ceramic-based prostheses with a 6-month follow-up period. Result: The porcelain-fused-to-metal prosthesis [PFM] based endocrown luted with GIC under proper isolation adheres perfectly with the bio integration concept and also had a success rate. Conclusions: Endocrowns has been considered as a promising treatment alternative for posterior endodontically treated teeth having excessive loss of coronal tooth structure associated with limited interocclusal space based on the patient's affordability and esthetic demands. The endocrown adheres perfectly with the bio integration concept & it should be used in restorative dentistry & should be more widely known.
Keywords: Endocrown, Porcelain-fused-to-metal prosthesis (PFM), Post-endodontic restoration, Esthetics
Full Text:
INTRODUCTION-
It remains a challenge to restore an endodontically treated tooth that has been extensively damaged. Their biomechanical deterioration impacts the tooth’s long-term prognosis.
The most commonly used restoration for these teeth still involves a post-retained foundation restoration and a crown. Increasing the retention of the core structure is the only advantage of post-insertion. Conversely, there is an increased risk of root fracture due to the weakening of the tooth structure because of intracanal retention. This type of restoration, as being invasive, makes the tooth prone to fracture (irreversible) & eliminates the chances for future interventions.1, 2
With progress in the advances of adhesive techniques, the emergence of minimally invasive dentistry without a post or crown is challenging the post-and crown concept.1 The monoblock technique, the antecedent of the endocrown was first described by Pissis in 1995.2 In 1993, Bindl and Mormann used the term-endocrown for the first.3 They discovered an adhesive restoration made up of monolithic ceramic secured to the pulp chamber, exploiting micromechanical retention properties of the walls of the pulp chamber.
CASE REPORT-
A female patient, 32 years old, reported to the Department of Prosthodontics and Crown & Bridge from the conservative & endodontics department with restoration in the upper left back tooth region. The patient gave a history of Root Canal Treatment done on the same tooth 5 days back and her medical history was non-contributory.
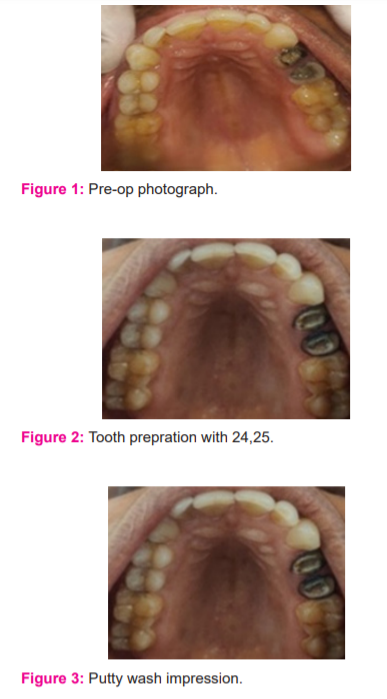
On a complete clinical examination, severe coronal loss of tooth structure was seen (Figure 1) Intra-oral periapical radiograph of 24, 25 shown an acceptable root canal filling without any indication of the periapical lesion and the patient was also asymptomatic.
Due to extensive destruction of coronal tooth structure, presence of thin walls, patient’s severe economic constraint, conservative post-endodontic management with a metal ceramic-based endocrown (Porcelain Fused to Metal ) was suggested as it has been considered as a practical, conservative,4 less complex & easily performed when compared with that of conventional crowns with post and core & after explaining the treatment options to the patient, informed consent was obtained and treatment is planned for endocrown.
Clinical procedure for metal-ceramic endocrown with 24,25
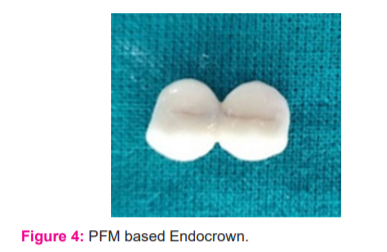
The tooth preparation was done according to the Bindl and Mörmann technique. At first, the reduction of the occlusal surface of the tooth (1.5-2mm) was carried out using a diamond wheel orienting it parallel to the occlusal surface. Using a flat end diamond bur at high speed, the cervical margins were levelled in shoulder shape maintaining a 1.5 mm thickness uniformly with the remaining coronal tooth structure under a constant cooling system throughout the procedure. (Figure 2)
The orientation of the bur was along the long axis of the tooth & a 7 to 10° of occlusal convergence was tried to maintain ensuring a constant flow of the prepared coronal pulp chamber & access cavity of depth approximately 3mm.
Opening of the root canal was carried out, and removal of GP (gutta-percha) 2 mm below each orifice level was completed, followed by complete sealing of the coronal orifices and the pulp chamber (2 mm thick) with glass ionomer restorative cement-Type II. The shouldered walls and margins were then smoothed with a finishing bur TR21EF (Dia-Burs, Mani).
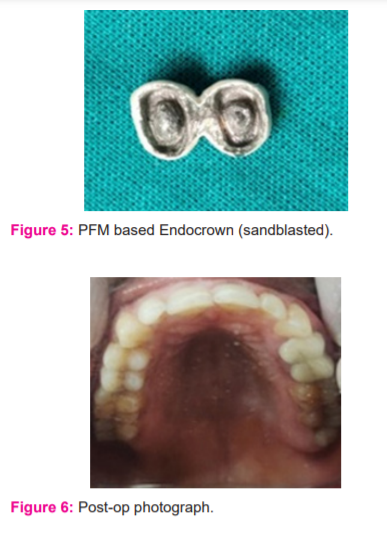
Gingival retraction cord 00 (Ultracord, Dent One Inc, USA) was applied along the gingival crevice and a polyvinyl siloxane impression was made (Aquasil LV, Dentsply DeTrey, Germany) using a single step putty wash impression technique (Figure 3) and for further processing, it was sent to the laboratory. Using tooth moulding temporary self-cure resin material, Temporization was done to maintain the dimensions of the prepared tooth in the inter-appointment period.
Also, sandblasting of the fabricated Porcelain Fused to Metal [PFM] endocrown was done to enhance the retention of this conservative single piece restoration (Figure 4 and 5) followed by luting of the final finished PFM based endocrown with GIC under proper isolation (Figure 6 and 7). The patient was then recalled after 6 months.
DISCUSSION-
In today’s era of adhesive dentistry, endocrown may be considered as a viable, feasible & conservative alternative to conventional crowns with post and core restorations. “The endocrown is secured to a pulpless posterior tooth, attached with the interior portion of the pulp chamber & cavity margins, obtaining micro-mechanical retention provided by the pulpal walls & micro-retention provided by the adhesive cementation”. In addition, it is an easier technique, has better acceptance, and require less clinical time making it a superior alternative amongst the various treatment options.
In another 2-year clinical study, according to Bernhart et al5 endocrowns presents a very promising treatment alternative for posterior endodontically treated teeth as well as it is proved to be very simple, feasible and having a success rate.
The endocrown adheres perfectly with the bio integration concept & can be a preferred choice for restoration of extensively damaged posterior endodontically treated teeth. Indications of endocrowns are especially in molars with roots that are small dilacerated, fragile, obliterated and severely mutilated tooth and also in situations, with extensive coronal tooth structure loss (i.e., ≥1/2 residual tooth structure) associated with inadequate interocclusal space, covering of ceramic of sufficient thickness on the metal/ceramic substructures is not possible to attain.
In this case, a PFM-based endocrown was planned according to the patient’s needs. As micro-retention can be affected in this case, the retention of the restoration was increased by incorporating secondary retentive grooves in the axial walls as stated in various studies6 in addition to the sandblasting of the metal surface before cementation thereby reducing the radius of rotation. Grooves limits the path of insertion & provides near parallel-sided walls to the preparation enhancing the retention.
Also, the resistance feature is enhanced by the anti-rotational design of the preparation. 7 According to Blair et al, anti-rotational design is chiefly used in metal-ceramic & all metal restorations but is generally unpractical for the all-ceramic crown. 8 Various other secondary retentive factors, such as pins, boxes, slots, can also be considered in such cases in a clinical scenario.
In addition, sandblasting was also done in PFM endocrown to enhance the bonding. Additionally, to provide enhanced retention & better bond quality, the cervical margins were levelled in a shoulder shape maintaining a uniform thickness thoroughly. Also, .the interior pulp chamber preparation might have enhanced the mechanical retention & stability of endocrown.
The removal of gutta-percha up to 2 mm in the pulp canal was carried out, to obtain the benefit of saddle-like anatomy of the floor of the cavity, & according to a biomimetic concept, placement of GIC in the pulp chamber creates a sufficient preparation geometry by filling of the internal undercuts, thereby contributing to an enhanced marginal seal in these cases. 9
However, contraindications of endocrowns are (1) pulp chamber depth - lesser than 3 mm or cervical margin width - lesser than 2 mm, (2) when there is only negligible remaining tooth structure present (3) when adhesion cannot be guaranteed. In addition, the differences in the MOE (modulus of elasticity) amongst the dentin and ceramic might lead to risks of root fracture and debonding. Hence, case selection is very critical & important for the continual success of endocrown-type of restoration.
Several factors such as the skill of the operator, correct tooth preparation techniques, suitable ceramic selection & bonding material influences the longevity & success of endocrown. In some circumstances, because of patients’ economical constraint & the lack of adhesive bonding, endocrown as a treatment option has been rejected. In such cases, PFM based endocrowns with adequate incorporation of retention and resistance features in the tooth preparation can be considered as a promising alternative.
In this case study, temporization was done with Luxatemp Automix Plus resin. The metal-ceramic crown, which will reproduce the natural tooth form, to respect the dental anatomy requires an adequate thickness, causing millions of dentinal tubules exposure which may act as a pathway for bacterial diffusion and colonization. Therefore, for the lasting success of the therapy, the prepared tooth surface must be adequately protected during prosthesis fabrication. Provisional restoration fixed with provisional cement offers acceptable retention, restoring form and function, acceptable esthetics as well as prevents tooth fracture and microleakage, to a certain degree maintaining the dimensions of the prepared tooth.
From a clinical perspective, if an obturating material in the root canal gets exposed to the saliva for 30 days or more, retreatment might be indicated. 10, In this case, report, the patient came within 15 days after the endodontic treatment for a definitive prosthesis.11
CONCLUSION-
Endocrowns has been considered as a promising treatment alternative for posterior endodontically treated teeth having excessive coronal loss of tooth structure associated along with the limited interocclusal space based on the esthetic demands & affordability of the patient. Though, PFM endocrowns might also be considered as a valuable treatment alternative, particularly in patients in whom economical constraint is a limiting factor. All the aforestated clinically significant factors should be analyzed before considering PFM-based endocrown in practical situations, to achieve favourable results. The endocrown adheres perfectly with the bio integration concept & it should be used in restorative dentistry & should be more widely known.
ACKNOWLEDGMENT:
The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
FUNDING: This research received no external funding.
CONFLICT OF INTEREST: The authors declare that they have no conflict of interest.

References:
1. Mukherjee P, Patel A, Chandak M, Kashikar R. Minimally Invasive Endodontics a Promising Future Concept: A Review Article. Int J Sci Stud. 2017;5(1):245-251.
2. Vinola SMJ, Balasubramanian S, Mahalaxmi S. “ENDOCROWN”—An Effective Viable Esthetic Option for Expurgated Endodontically treated Teeth: Two Case Reports. J Oper Dent Endod. 2017;2(2):97-102
3. Bindl A, Mörmann WH. Clinical evaluation of adhesively placed Cerec endocrowns after 2 years–preliminary results. J Adhes Dent. 1999;1:255-65.
4. Oswal N, Chandak M, Oswal R, Saoji M. Management of endodontically treated teeth with endocrown. J Datta Meghe Inst Med Sci Univ. 2018;13:60-2.
5. Bernhart J, Bräuning A, Altenburger MJ, Wrbas KT. Cerec3D endocrowns–two-year clinical examination of CAD/CAM crowns for restoring endodontically treated molars. Int J Comput Dent. 2009 Dec;13(2):141-154.
6. Casucci A, Osorio E, Osorio R, Monticelli F, Toledano M, Mazzitelli C, Ferrari M. Influence of different surface treatments on surface zirconia frameworks. J Dent. 2009 Nov;37(11): 891-897.
7. Raigrodski AJ. Contemporary materials and technologies for all-ceramic fixed partial dentures: a review of the literature. J Prosthet Dent. 2004 Dec;92(6):557-562.
8. Blair FM, Wassell RW, Steele JG. Crowns and other extracorporeal restorations: preparations for full veneer crowns. Br Dent J. 2002 May;192(10):561-571.
9. Amal S, Nair MG, Sreeja J, Babu A, Ajas A. Endocrown – an overlooked alternative. Arch Dent Med Res. 2016;2(1): 34-38.
10. Siqueira JF Jr. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J. 2001 Jan;34(1):1-10.
11. Ashok: Evaluation of postoperative complaints in fixed partial denture wearers and those with crowns: A questionnaire-based study.Int J Cur Res Rev. 2016;8(16).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





