IJCRR - 7(23), December, 2015
Pages: 30-33
Date of Publication: 10-Dec-2015
Print Article
Download XML Download PDF
LIPID PROFILE AND RISK OF OBESITY AMONG URBAN ADULTS
Author: Surinder Sharma, Bhuwan Sharma
Category: Healthcare
Abstract:Background: Dyslipidemia is a major risk factor for coronary heart disease and refers to lipid abnormalities such as high total cholesterol (TC), elevated low density lipoprotein cholesterol (LDL-C), hypertriglyceridemia, low high density lipoprotein cholesterol (HDL-C).Due to the scarcity of data, we performed a descriptive study so as to understand the pattern of lipid profile in an urban city in North India and the risk of obesity running in them. Methods: This cross-sectional study was performed by collecting data from three private hospitals in the city from January 1, 2014 till June 31, 2014. Patients who satisfied our inclusion criteria were included in the study. Participants of the study underwent standard hematological testing along with variables about their past medical history and anthropometric measurements were taken. Data was analyzed using SPSS version 21. Results: 636 patients were included in the study. 54% of the patients were males, 64% less than 65 years of age, 35% were overweight and 16% were obese. 33% were taking some form of lipid lowering drug. 67% had TC < 200 mg%, LDL-C < 130 mg% and HDL-C > 40 mg%. TC, LDL-C and triglycerides were found to be significantly associated with age and body mass index of the patient. Conclusion: This was the first study in the region to look at the baseline lipid profile of patients. Assessing dietary habits, nutritional status of patients, genetic make up and environmental factors and correlating that with their lipid profile variables would be the next step and would constitute areas of future research.
Keywords: Lipid, Population, Obesity, Dietary, Prevention, Urban
Full Text:
INTRODUCTION
Diseases like stroke, coronary heart disease, and diabetes are the most important cause of mortality today.1 Many times these diseases are preventable by simple measures. Cardiovascular disease remains as one of the most important public health problems in developed countries, while it is gaining foothold in developing countries like India as well. Previously conducted epidemiological studies of populations who have been followed for a long time have identified certain characteristics and lifestyles that are strongly associated with an increased risk of cardiovascular diseases. Smoking, lack of physical activity, poor dietary choice, hypertension are some of the risk factors which we know from previous studies are rick factors strongly related to increased morbidity.2 , 3 Dyslipidemia is a major risk factor for coronary heart disease and refers to lipid abnormalities such as high total cholesterol (TC), elevated low density lipoprotein cholesterol (LDL-C), hypertriglyceridemia, low high density lipoprotein cholesterol (HDL-C). 4 million deaths annually and about 50% of cases of ischemic heart disease worldwide have been estimated to be associated with dyslipidemia by the World Health Organization.4 Dyslipidemia has direct consequences on the risk of various disabling cardio- and cerebrovascular events. Due to the scarcity of data, we performed a descriptive study so as to understand the pattern of lipid profile in an urban city in North India and the risk of obesity running in them. This would be helpful because many studies have shown that modification of the plasma lipid concentrations is a useful approach in decreasing cardiovascular mortality
METHODOLOGY
Setting This cross-sectional study was conducted in the urban city of Jalandhar, Punjab, where we included patients who presented to private hospitals with in house laboratory services. We divided the city in four regions and in each region we identified four private hospitals in the city, of which three agreed to share their data with us. Institutional ethics review was obtained individually from each hospital. These three hospitals were located at approximately 7-8 kilometers away from each other, thereby covering majority of the urban population of Jalandhar. With a population of 21,93,590, 52% of which are males, Jalandhar is the fourth populous city of Punjab. The three hospitals were visited by 200-250 patients each daily in the outpatient department. Patients, who were admitted to these hospitals, mainly belonging to middle, upper-middle socioeconomic class, were usually from urban Jalandhar.
Study design We collected patient information from January 1, 2014 till June 30, 2014, from hospital records. We included all patients, aged 18 years or above, who were admitted in any inpatient ward in the included hospitals. Patients who only visited the outpatient department were not included in the study because of the lack of follow-up in these patients. After obtaining an informed consent, we collected demographic information like age, gender, body weight, any comorbid condition (present for more than a year and for which active treatment is being taken by the participant) or whether they are taking any lipid lowering drug or not. Lipid profile measurements were done using enzymatic method (Diasys diagnostic systems, Gmbh, Germany), which provides automated results. All laboratories followed standardization procedures as recommended by the World Health Organization, including the use of external control sera. All blood samples were taken early morning, after overnight fasting.
Definitions High total cholesterol (TC), high triglyceride (TG), high low-density lipoprotein cholesterol (LDL-C), and low highdensity lipoprotein cholesterol (HDL-C) were defined as TC ≥ 200mg/dL, TG ≥150mg/dL, LDL-C ≥130mg/dL, and HDL-C <40mg/dL according to the criteria prescribed by the Third Report of The National Cholesterol Education Program (NCEP) expert panel.5 Based on these definitions participants with dyslipidemia were identified.
Data collection and analysis Data obtained from hospitals was codified and entered into Microsoft excel sheets. Data were then analyzed using the Statistical Package for Social Sciences (SPSS) version 21. From their weight and height, Body Mass Index (BMI) was calculated. Participants were later grouped based on their lipid profile variables, using the criteria prescribed by the NCEP expert panel. Correlation between lipid profile values and age, and BMI of participants was determined using Pearson’s correlation analysis, p < 0.05 were considered to be significant.
RESULTS
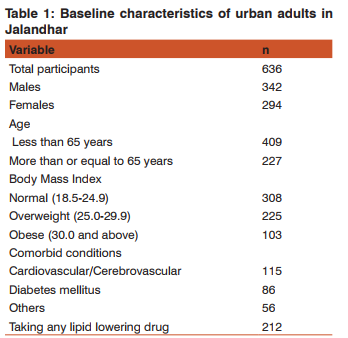
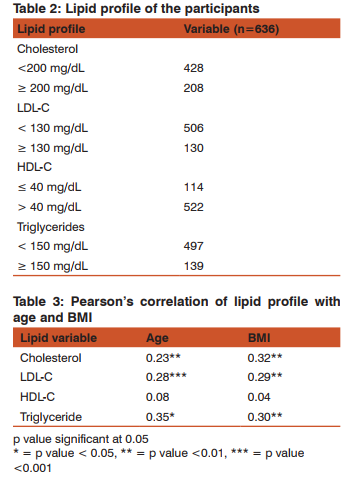
636 patients fulfilled our inclusion and exclusion criteria, 54% of which were males. 64% of the study population was aged 65 years or less. Using BMI values as shown in Table 1, 35% of the patients were overweight and 16% was obese. Of all the patients 40% had some comorbid condition, from which they were suffering for more than a year and were taking active treatment for it. 33% of the total study population was taking a lipid-lowering drug. Using cut off values for various lipid profile variables, 67% had normal total cholesterol levels, 79% had normal low density lipid cholesterol levels, 82% had higher than prescribed high density lipid levels and 78% had normal triglyceride levels. On further analysis, total cholesterol, LDL-C and TG showed statistically significant positive association with age and BMI. However, HDL-C showed no statistically significant associations with age or BMI. Refer to Table 3 for details.
DISCUSSION
India is witnessing double burden of communicable and non-communicable diseases. Earlier much stress was laid on communicable diseases and still the national health programs focus more towards communicable diseases. Recently launched National Programme For Prevention and Control of Cancer, Diabetes, Cardiovascular Disease and Stroke is a step towards increasing awareness of the general population towards lifestyle diseases. Therefore the purpose of this study was to study the lipid profile of adults living in an urban city of Jalandhar, Punjab which has never been studied before. 35% of our study population was overweight and 16% were obese. This should be kept in context of the view that 64% of the population was below 65 years f age. Deranged lipid profile is an interplay of various factors, genetic and environmental in particular. We have seen similar prevalence of dyslipidemia in other Asian populations, including Bangladeshi and Pakistani populations.6 Sometimes, even with low cholesterol and LDL levels risk of coronary heart disease remains high, like in Turkish populations.7 This has been attributed to genetic variations leading to low HDL levels in them.Dyslipidemia could be familial or secondary to several medical conditions, which include type 2 diabetes mellitus, excessive alcohol consumption, smoking, hypothyroidism, cholestatic liver disease, and obesity. In type 2 diabetes mellitus, the lipid abnormalities include elevated TGs, LDL-C and low HDL-C in a setting of insulin resistance.8 Excessive alcohol consumption can cause hypertriglyceridemia, and it was found in a study among hypertensive men who consume alcohol found that the risk of high TGs increased with increasing alcohol consumption.9 Screening for lipid abnormalities is widely recommended and practiced in industrialized nations. While some may suggest that evaluation for dyslipidemia is primarily aimed at identifying those who are candidates for lipid-lowering therapy, however a broader perspective is that lipid testing provides one component of the assessment of overall cardiovascular risk. It also helps to identify those who are likely to benefit from any of several different interventions, such as aspirin and antihypertensive therapy, that lower cardiovascular risk. One key component of a comprehensive plan to improve cardiovascular outcomes in patients with dyslipidemia is lipid-lowering therapy with statins. Results of our study will help health policy makers adopt a national strategy to prevent the extension of cardiovascular risk factors in the population and could serve as a baseline for assessment of future trends in the risk factors studied. With better health facilities, India as a nation is trying to overcome barriers to control communicable diseases. Now we need to shift our focus towards preventing non-communicable diseases. Our study has a few limitations. This study was conducted in a single city of India. Dietary habits of Indians vary state to state. Therefore the results of this study might not be generalizable to other parts of India or communities. Apart from BMI, waist circumference and waist-hop ratio have been prescribed by WHO to be used for assessment of obesity. These two variables are missing from our study
CONCLUSIONS
Our study tried to describe the lipid profile of adults in an urban city in India. This provides us with baseline information on the current scenario is and what needs to be done to improve that. Assessing dietary habits, nutritional status of patients, genetic make up and environmental factors and correlating that with their lipid profile variables would be the next step and would constitute areas of future research.
ACKNOWLEDGEMENT
Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors / editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. WHO mortality database. Website http://www.who.int/healthinfo/mortality_data/en/ Accessed Oct 15, 2015.
2. Bao W, Srinivasan SR, Wattigney WA and Berenson GS (1995): The relation of parental cardiovascular disease to risk factors in children and young adults. The Bogalusa Heart Study.Circulation 91, 365–371.
3. Shaw LW (1981): Effects of a prescribed supervised exercise program on mortality and cardiovascular morbidity in patients after myocardial infarction. The National Exercise and Heart Disease Project. Am. J. Cardiol. 48, 39–46.
4. World Health Organization. Quantifying selected major risks to health. In: The World Health Report 2002 - Reducing Risks, Promoting Healthy Life. Ch. 4. Geneva: World Health Organization; 2002. p. 47-97.
5. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001; 285: 2486-97.
6. Bhopal, R., N. Unwin, M. White, J. Yallop, L. Walker, K. G. M. M. Alberti, J. Harland, S. Patel, N. Ahmad, C. Turner, B. Watson, D. Kaur, A. Kulkarni, M. Laker, and A. Tavridou. 1999. Heterogeneity of coronary heart disease risk factors in Indian, Pakistani, Ban- gladeshi, and European origin populations: cross sectional study. BMJ. 319: 215 – 220.
7. Mahley, R. W., K. Erhan-Palaoglu, Z. Atak, J. Dawson-Pepin, A. M. Langlois, V. Cheung, H. Onat, P. Fulks, L. Mahley, F. Vakar, S. O?zbayrakci, O. Go?kdemir, and W. Winkler. 1995. Turkish heart study: lipids, lipoproteins and apolipoproteins. J. Lipid Res. 36: 839 – 859.
8. Zavaroni I, Dall’Aglio E, Alpi O, Bruschi F, Bonora E, Pezzarossa A, et al. Evidence for an independent relationship between plasma insulin and concentration of high density lipoprotein cholesterol and triglyceride. Atherosclerosis 1985;55:259-66.
9. Park H, Kim K. Association of alcohol consumption with lipid profile in hypertensive men. Alcohol Alcohol 2012;47:282-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





