IJCRR - 13(11), June, 2021
Pages: 87-91
Date of Publication: 04-Jun-2021
Print Article
Download XML Download PDF
Effectiveness of Muscle Energy Technique versus Positional Release Technique on Upper Trapezius Trigger Points in Subjects with Neck Pain \? Comparative Study
Author: Nipa Patel, Sonali Desai, Priyanshi Patel
Category: Healthcare
Abstract:Introduction: The neck is the most common site of nontraumatic musculoskeletal pain. Because the trapezius muscle works to move the neck in several directions, its degree of tightness or looseness affects neck flexibility. For people who work with more movements of the neck, or who spend many hours driving, the upper trapezius becomes very painful and sore. MET(Muscle Energy Technique) and PRT (Positional Release Technique) both are effective forms of treatment for upper trapezius trigger points. So this study compares these two techniques. Objective: This study compared the effect of Muscle Energy Technique (MET) and Positional Release Technique (PRT) on upper trapezius trigger points in subjects with neck pain Methods: This study involved 30 (13 males and 17 females) individuals with neck pain (Duration less than 1 month) and trapezius trigger point. They were divided into two groups: Group A- PRT + Conventional treatment and Group B- MET + Conventional treatment. Treatment was given for 1 week. Pre and Post measurements were taken (VAS was used to measure pain and NDI was used to assess neck disability). Data were analysed using unpaired t-test and paired t-test. Results: In within-group analysis, the p value was less than 0.05 (p< 0.05) for both groups so it suggests that both (PRT and MET) were effective to reduce pain and disability. No significant difference between the groups was noted. Conclusion: Both Positional Release Therapy and Muscle Energy Technique were significantly effective in reducing pain and neck disability in subjects with neck pain. But none technique is superior to the other.
Keywords: Muscle Energy Technique (MET), Positional Release Technique (PRT), Trigger points, Neck pain, Upper Trapezius, Neck Disabilit
Full Text:
Introduction
The neck is the most common site of nontraumatic musculoskeletal pain.1 The International Association for the Study of Pain defines neck pain as: “Pain perceived as arising from anywhere within the region bounded superiorly by superior nuchal line, inferior by an unoriginally transverse line through the tip of the first thoracic spinous process, and laterally by sagittal plane tangential to the lateral border of the neck”.2 Population-based surveys have shown lifetime prevalence of neck pain between 67% to 87% .3 Upper trapezius is designated as postural muscle.4 Any position which places trapezius in a shortened state for some time without rest may shorten the fibres and lead to dysfunction and restricted movements of the neck.5 A TrP is a hyperirritability spot in skeletal muscle or its fascia, located in palpable taut bands, which can be active or latent.6 Trigger points form in the muscle fibres, close to the motor endplate (neuromuscular junction). Excess acetylcholine (ACH) is released at the synapse, usually associated with overuse or strain, leading to the release of calcium. The resulting ischemia creates an O2 deficit and energy crisis. Symptoms of Active trigger points include resting pain, tenderness on palpation and can also have referred pain pattern. Also, Latent Trips can cause weakness and restrict movement -and pain is not spontaneous.7 MTrPs are considered a major source of pain in 30% of individuals with musculoskeletal dysfunction.8 Clinical signs of MTrPs include taut band, reproducing of pain, referred pain, restricted range of motion and muscle weakness.9 Muscle palpation adjacent to active myofascial trigger points feels tense.10 For deactivation of Trigger Points (TrPs) and decrease spasm Manual approaches like Muscle Energy Techniques (METs) and Positional Release Technique (PRT) is very effective.11 Muscle energy techniques (MET) were originally developed by two osteopathic physicians, Fred Mitchell, Sr. and Fred Mitchell, Jr.12 The approach involves the introduction of an isometric contraction to the affected muscle producing post isometric relaxation through the influence of the Golgi tendon organs (autogenic inhibition).11 MET may be used to decrease pain, stretch tight muscles and fascia, reduce muscle tonus, improve local circulation, strengthen weak musculature and mobilize joint restrictions.11 Positional Release Therapy [PRT] was developed by Lawrence H.13 PRT is a method in which muscles are placed in a position of greatest comfort, and this causes normalization of muscle hypertonicity and fascial tension. Also, it decreases joint hypomobility, increases circulation, followed by a reduction in swelling, decreased pain, and increase muscle strength.14 There are several studies available that compare these two techniques. After comparing MET and PRT for upper trapezius muscle spasm in computer workers and it is found that PRT is a more effective treatment.11 While other reported MET as a more effective form of treatment.7 Therefore this study will add to the growing body of knowledge whether these two techniques yield comparable outcomes or if one technique is superior to the other.
Materials and Methods
Patients were selected by convenient sampling based on inclusion (subjects having neck pain with unilateral upper trapezius trigger point, Age: 20-40 years, Duration of pain less than 1 month, VAS > 5, NDIQ > 15) and exclusion Criteria (Fracture of the cervical spine, neck pain with radiation into arms or upper extremity, Diagnosed cases of disc prolapsed, Any neurological impairment, Tumor in the cervical region, Any deformity e.g. spasmodic torticollis, Sprengel's deformity, scoliosis, History of surgery of the cervical spine during the previous 12 months, patients who are taking analgesics). The study was properly explained and informed consent was taken. They were divided into two groups:
Group A- PRT + Conventional treatment
Group B- MET + Conventional treatment
Pre-outcome measurements (VAS and NDI) were taken on 1st day before starting treatment. Conventional treatment (hot pack, Active neck movements, Shoulder bracing exercises, chin tuck exercises and trapezius stretching) was given in both groups along with specialized technique (MET or PRT)
Application of PRT
-
Then therapist applied Pressure by pinching the muscle between the thumb and fingers. Lateral flexion of subject’s head toward the side of a tender point, the therapist grasps the subject’s forearm and abducts shoulder to approximately 90° and adds slight flexion or extension to fine-tune.
-
The most comfortable position achieved was held for 90 seconds and after that passive return of the body part to an anatomically neutral position was maintained for 5minutes.15
Application of MET:
-
The patient lies supine, arm on the side to be treated lying alongside the trunk, head/neck side-bent away from the side being treated to just short of the restriction barrier, while the practitioner stabilizes the shoulder with one hand and cups the Ipsilateral ear/mastoid area, with the other.
-
With the flexed neck fully side-bent, and fully rotated towards the opposite side, the posterior fibres of the upper trapezius are involved in the contraction. This facilitates subsequent stretching of this aspect of the muscle.
-
With the flexed neck fully side-bent and half rotated, the middle fibres are involved in the contraction.
-
With the flexed neck fully side-bent and slightly rotated towards the side being treated, the anterior fibres of the upper trapezius are engaged.
-
The various contractions and subsequent stretches can be performed with the practitioner's arms crossed, hands stabilizing the mastoid area and shoulder.
-
The patient introduces a light resisted effort (20% of available strength) to take the stabilised shoulder towards the ear (a shrug movement) and the ear towards the shoulder.
-
The opposite effort towards movement is important in order to introduce a contraction of the muscle from both ends simultaneously.
-
The degree of effort should be mild and there should be no pain.
-
This contraction should be maintained for 7-10 seconds and, upon complete relaxation of effort, the practitioner gently eases the head/neck into an increased degree of side-bending and rotation, where it is stabilized, as the shoulder is stretched caudally.
-
As stretching is introduced, the patient can usefully assist in this phase of the treatment by initiating, on instruction, the stretch of the muscle ('as you breathe out please slide your hand towards your feet).
-
Patient participation in the stretch reduces the chances of a stretch reflex being initiated.
-
Once the muscle is in a stretched position, the patient relaxes and the stretch is held for up to 30 seconds.16
Treatment was given for 1 week. Post-treatment outcome measurements (VAS and NDI) were taken after the last session of treatment.
Results
The study comprised of total thirty patients (13 males and 17 females). The age of the subject ranged from 22 to 39 years (mean age – 36.16 years). Group 1 consists of 15 patients (mean age – 34.66 years) and group 2 consists of 15 patients (mean age – 37.66 years). Data were analysed using statistical software SPSS version 20. Before applying statistical tests, data were screened for normal distribution. The level of significance was kept at 95 %.
Within-group analysis
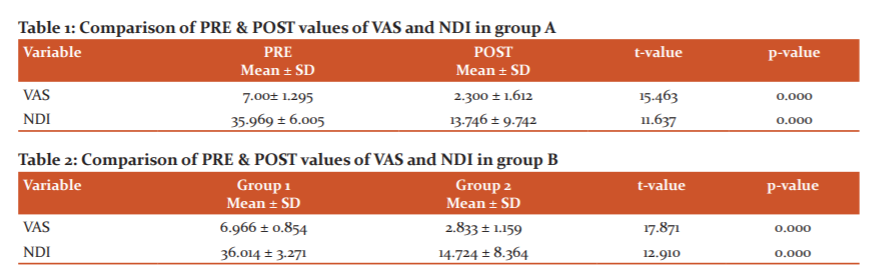
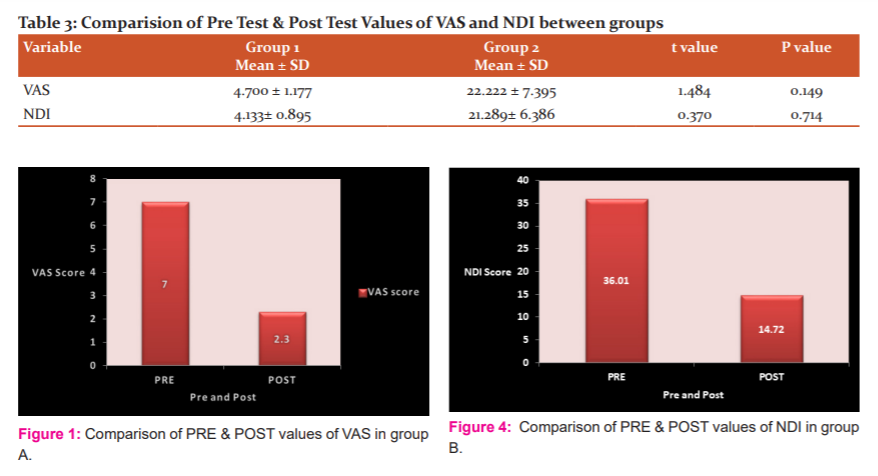
Group A: Paired t-test was used to compare the Pre and Post value of VAS and NDI in group A. And p-value is less than 0.05 (p<0.05) so it suggests the significant difference between the values. So MET is an effective treatment to reduce pain and neck disability in individuals with upper trapezius tender points (Table 1, Figures 1 and 3).
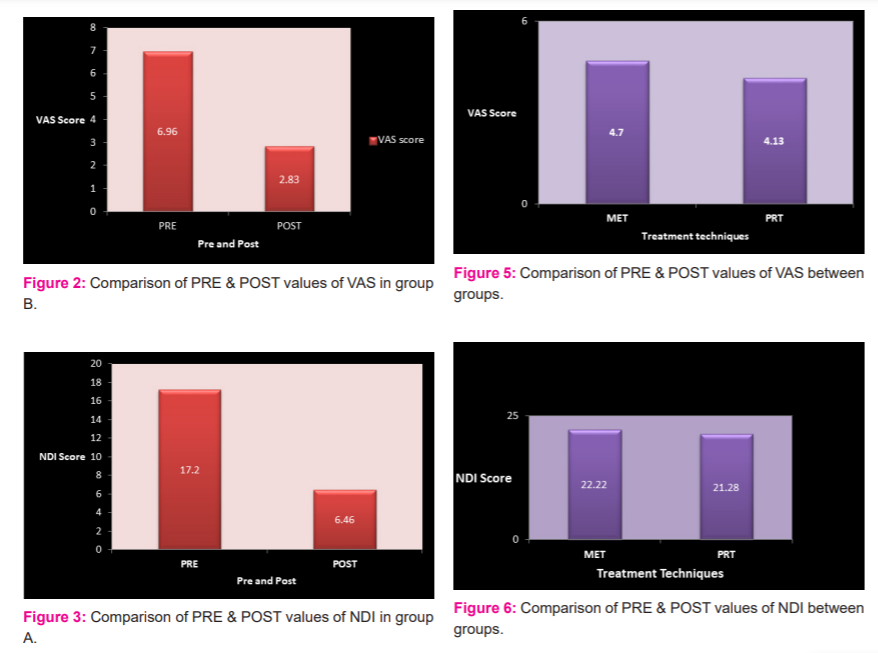
Group B: Paired t-test was used to compare the Pre and Post value of VAS and NDI in group B. And p-value is less than 0.05 (p< 0.05) so it suggests the significant difference between the values. So PRT is an effective treatment to reduce pain and neck disability in individuals with upper trapezius tender points (Table 2, Figures 2 and 4).
Between groups analysis
Un-paired t-test was used to compare the difference in VAS (Visual Analog Scale) and NDI (Neck Disability Index) between the groups. And P-value is more than 0.05 (P > 0.05) so it suggests no significant difference between the values. So there is no significant difference between the effect of MET and PRT to reduce pain and neck disability in individuals with upper trapezius tender points. (Table 3, Figure 5 and 6)
Discussion
Our study was aimed to compare the Muscle Energy Technique versus Positional Release Technique on pain and neck disability in individuals with neck pain. The within-group analysis had shown that there was a significant reduction in pain intensity (VAS) and neck disability (NDI) in both groups, which means that both the treatments (MET and PRT) were effective. Whereas Between groups analysis had shown that there was no significant difference between the effects of both treatments. Muscle energy technique has its effects over the stretch receptors called Golgi tendons and spindles which react to overstretch of muscle and inhibit further muscle contraction. When GTO is triggered, afferent nerve impulses enter the spinal cord dorsal root and reach the inhibitory motor neuron which stops impulses discharge from the efferent motor neuron. This prevents muscle contraction causing lengthening and relaxation of agonist. They also react to movements of the body and this may have a relaxing effect on the muscle. When a muscle gets shorten, the discharge through the spindle decreases and it relaxes the muscle. Pain relief could have occurred due to a decrease in the intrafusal and extrafusal fibre disparity and reset of the inappropriate proprioceptive activity. MET may influence pain mechanisms and promote hypoalgesia. The mechanisms are not known but may involve central and peripheral modulatory mechanisms, such as activation of muscle and joint mechanoreceptors may reduce pro-inflammatory cytokines and desensitize peripheral nociceptors. It may be effective due to the production of viscoelastic change and passive extensibility of muscle. Our finding is supported by a study done by Phadke et al.,2 in which they have compared MET with static stretching in a patient with mechanical neck pain and they found better improvement in the MET group as compared to the stretching group. Positional release therapy is an indirect myofascial technique focusing on the neurologic component of the neurovascular myofascial somatic dysfunction and is proposed to increase muscle flexibility. According to the Korr model, placing the muscle in a shortened position may decrease the muscle spindle activity and enables the central nervous system to decrease gamma discharge activity, therefore inhibiting the facilitated segment of the spinal cord. By shortening the extrafusal fibres or placing them in a position of ease, Korr hypothesises that the intrafusal and extrafusal fibre disparity decreases and the gamma discharge are turned down. This enables the muscle to return to its normal resting length as the hyperactive muscle spindles cease to fire. This passive approximation may be referred to as positional release.3 The effect of PRT is also based on local circulation, inflammatory reaction and neurophysiologic regulation of an activity that is influenced by the sympathetic nervous system. PRT removes restricted barriers of movement by decreasing muscle spasm, trigger point, pain and swelling and increasing circulation. Our finding is supported by a study done by Kumaresan et al.4 as they concluded that Positional Release Therapy can be useful in alleviating neck pain and improve functional ability. According to our results, both techniques were effective in reducing pain and functional disability in our patients. This finding is supported by a study done by Yeole,13 in which they have compared MET and PRT on neck pain in computer users and they found both techniques are effective in reducing pain and improving function in computer users with neck pain. Whereas study done by Thaker et al.7 concluded that the Muscle energy technique (MET) is an effective option in the treatment of chronic upper trapezius than the Positional Release Technique (PRT). Also, a study done by Rana et al.11 concluded that PRT was more statistically and clinically superior for decreasing VAS, NDI score and improving ROM and MMT. PRT showed earlier pain relief as compared to MET. Both groups received isometric neck exercises and upper trapezius stretching exercises with moist heat therapy and are known to have effects on pain and spasm and thus can attribute to pain relief and improved tissue extensibility in both groups.
Conclusion
This study concluded that both Muscle Energy Technique and Positional Release Therapy were significantly effective in reducing pain and neck disability in subjects with neck pain. After comparison, Cit showed that there was no difference between the effects of these two techniques. So we can use both techniques in clinical practice.
Acknowledgement: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Conflict of interest: Nil
Source of funding: Nil
References:
-
Mahajan R, Kataria C, Bansal K. Comparative effectiveness of muscle energy technique and static stretching for treatment of subacute mechanical neck pain. Int J Health Rehabil Sci 2012 Jul;1(1):16-21.
-
Phadke A, Bedekar N, Shyam A, Sancheti P. Effect of muscle energy technique and static stretching on pain and functional disability in patients with mechanical neck pain: A randomized controlled trial. Hong Kong Physiother J. 2016;35:5-11.
-
Alagesan J, Shah US. Effect of positional release therapy and taping on unilateral upper trapezius tender points. Int J Health Pharmac Sci. 2012;1(2):13-7.
-
Kumaresan A, Deepthi G, Anandh V, Prathap S. Effectiveness of positional release therapy in the treatment of trapezius. Int J Pharmac Sci Health Care. 2012;1(2):71-81.
-
Ravish VN, Helen S. To compare the effectiveness of myofascial release technique versus positional release technique with laser in patients with the unilateral trapezius. J Evol Med Dental Sci 2014;3(9):2161-7.
-
Saavedra FJ, Cordeiro MT, Alves JV, Fernandes HM, Reis VM, Mont'Alverne DG. The influence of positional release therapy on the myofascial tension of the upper trapezius muscle. Revista Brasileira de Cineantropometria & Desempenho Humano. 2014;16(2):191-9.
-
Thaker S, Dave Y, Patel S. A study to compare the effect of muscle energy techniques and positional release technique on pain and cervical ROM in patients with the chronic upper trapezius. Int J Sci Res. 2019; 8(6):13-17.
-
Basak T, Pal TK, Sasi M. A Comparative Study on the Efficacy of Ischaemic Compression and Dry Needling with Muscle Energy Technique in Patients with Upper Trapezius Myofascial Trigger Points. Int J Health Sci Res. 2018;8(4):74-81.
-
Shah N, Shah N. Comparison of two treatment techniques: Muscle energy technique and Ischemic compression on upper trapezius trigger point in subjects with non-specific neck pain. Int J Therap Rehabil Res. 2015;4(5):260-264 .
-
Rashad A, Asif M, Chughtai RB, Tanveer E, Uddin S, Amjad B, et al. Efficacy of Positional Release Therapy versus Integrated Neuromuscular Ischemic Technique in the Treatment of Upper Trapezius Trigger Point. J Phy Fit Treatment Sports. 2019;6(4): 555694 .
-
Rana P, Brahmbhatt B. Effect of muscle energy technique versus positional release technique in computer workers with upper trapezius muscle spasm: A comparative study. Int J Multidisc Res Dev. 2017;4(5):29-35 .
-
Thomas E, Cavallaro AR, Mani D, Bianco A, Palma A. The efficacy of muscle energy techniques in symptomatic and asymptomatic subjects: a systematic review. Chiroprac Man Ther. 2019;27(1):35.
-
Yeole UL, Diwakar NP, Pawar PP. Effect of Muscle Energy Technique And Positional Release Therapy on Neck Pain In Computer Users-A Randomized Control Trial. Int J Recent Sci Res. 2017;8(12):22490-22493.
-
Rishi P, Singh G. Effect of positional release technique versus ischemic compression on pressure pain threshold. Range of motion, and headache patients among college going , students. A randomized controlled trial. Int J Physiother. 2019;6(4):140-148 .
-
Chaitow L. Positional release techniques. 3rd Ed. Churchill Livingstone Elsevier; 2007
-
Chaitow L, Crenshaw K. Muscle energy techniques.3rd Ed. Elsevier Health Sciences; 2006.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





