IJCRR - 13(11), June, 2021
Pages: 35-37
Date of Publication: 04-Jun-2021
Print Article
Download XML Download PDF
A Pathological Surprise in a Non-Functioning Kidney
Author: Kundhavai Chandrasekaran, Lawrence D' Cruze, Sandhya Sundaram, K. Natarajan
Category: Healthcare
Abstract:Introduction: Upper urinary tract urothelial carcinoma is rare and accounts for about 5-10% of urothelial carcinomas. Grossly it may arise anywhere between the renal calyces to the distal ureter. Case Report: We report a very rare case of a 65-year-old male whose clinical and radiological diagnosis was pyelonephritis and non-functioning kidney but it turned out to be an unusual presentation of the tumour involving the entire kidney mimicking renal cell carcinoma. The final diagnosis of a high grade invasive urothelial carcinoma with squamous differentiation was rendered on histopathology highlighting the very rare presentation. Conclusion: We report a rare case of high-grade urothelial carcinoma in a non-functioning kidney.
Keywords: Kidney involvement, Pyelonephritis, Non-functioning kidney, Squamous differentiation, Upper urinary tract tumour, Urothelial carcinoma
Full Text:
INTRODUCTION
Upper urinary tract urothelial carcinoma is relatively rare and accounts for about only 5-10% of urothelial carcinomas.1Grossly it may arise anywhere between the renal calyces to the distal ureter.1,2 The tumour is usually advanced at the time of diagnosis. we report a rare case of urothelial carcinoma of the upper urinary tract.
CASE REPORT
We report a case of a 65-year-old male who presented with right-sided loin pain, decreased urine output and low-grade fever for a week. On examination, right renal angle tenderness was present. So with a clinical diagnosis of right pyelonephritis routine investigations were done. Urine examination showed 5-6 pus cells and urine culture showed E.coli growth. The patient had anaemia and hypoproteinemia.
CT - KUB showed a perinephric fluid collection with the possibility of infective aetiology.CT guided urogram revealed a nonfunctioning kidney with renal abscess extending into perinephric fat. Right ureteritis and cystitis were also seen.DTPA Renogram could not visualise right kidney indicating loss of function of the right kidney and subnormal function of left kidney. So with the clinical and radiological diagnosis of pyelonephritis and non-functioning kidney, open right nephroureterectomy was performed and the specimen was sent for histopathological examination.
PATHOLOGICAL FINDINGS
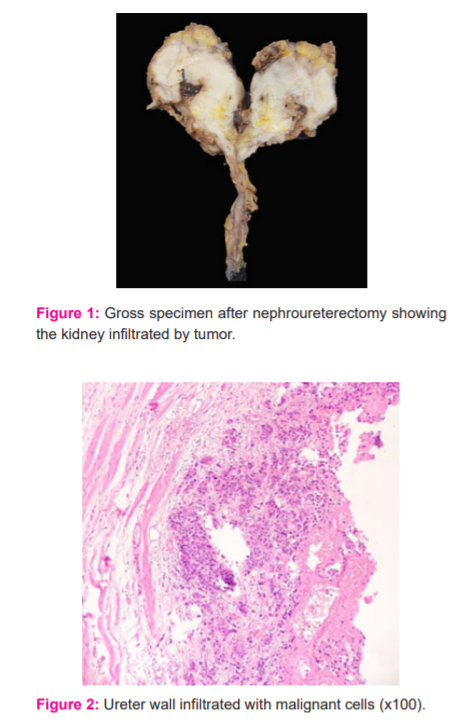
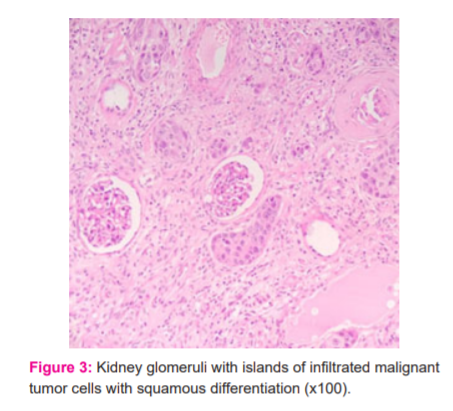
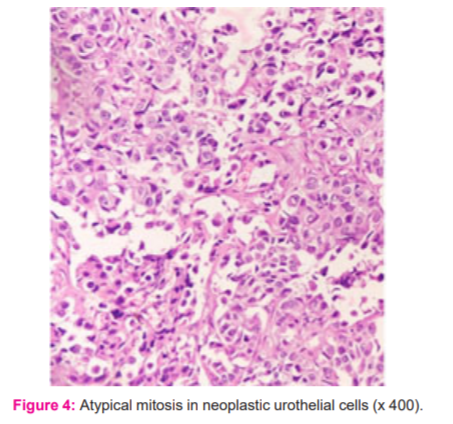
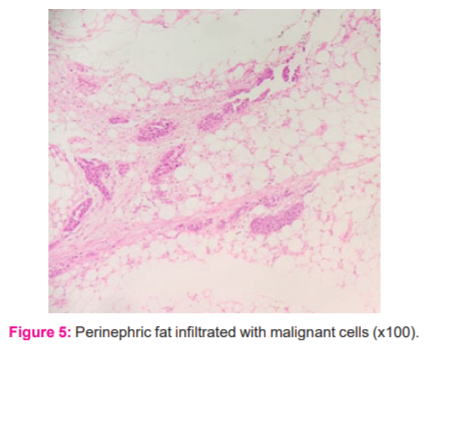
The right kidney specimen measured 8.7 x 5.4 x 4.5 cm. Grossly, on the cut section, there was a grey white lesion involving the entire kidney and extending into the ureter and perinephric fat mimicking renal cell carcinoma. The lesion was grey-white, soft to firm in consistency with no areas of haemorrhage or necrosis. The corticomedullary junction could not be made out. On microscopy, the lesion was arising from ureter and infiltrating into renal pelvis and renal parenchyma and the perinephric fat with dysplastic changes in the ureter. The lesion was composed of tumour cells arranged in sheets and clusters with individual cells having moderate to abundant eosinophilic cytoplasm and pleomorphic nuclei. Atypical mitosis was also seen. Few areas showed a squamoid pattern with intercellular bridges. Resected ureter margins showed carcinoma in situ. The final diagnosis was pT4 pNx Grade 2 Moderately differentiated High-grade urothelial carcinoma with squamous differentiation.
Repeat surgery - Right segmental ureterectomy with bladder cuff resection was done. Grossly it was a 3cm tumour beyond muscularis into periureteral fat. The diagnosis was pT3 pNx High grade invasive urothelial carcinoma.
DISCUSSION
Upper urinary tract urothelial carcinoma is rare. The most common presentation is hematuria(70-80%),3 and loin pain. The elderly age group is most affected and has a male preponderance.4 CT urogram is the preferred investigation and cystoscopy and ureteroscopy is preferred for taking biopsies.1
Intratubular spread has a very important impact on staging.4 types of intratubular spreads are pagetoid, typical, florid, secondary invasion from the intratubular spread.2 High-grade tumours have extensive intratubular spread.2 Urothelial carcinoma histologically has tumour cells arranged in sheets, cords with individual cells having moderate to abundant eosinophilic cytoplasm, pleomorphic nuclei. According to the literature, squamous differentiation is more commonly seen than glandular differentiation in urothelial carcinoma.5 Squamous differentiation was associated with chronic inflammatory conditions like chronic pyelonephritis. Few studies have shown squamous differentiation associated with poor prognosis.6
Sometimes the low-risk patients are treated by kidney sparing surgery.7 However, the gold standard treatment for upper urinary tract urothelial carcinoma is radical nephroureterectomy with bladder cuff resection.8 Majority of the patients with upper tract urothelial carcinoma present in higher grade and stage of the tumour. So the upper tract urothelial carcinoma has poor prognosis than the bladder tumour.9 Recurrences can occur in the bladder.
CONCLUSION
We report a case of upper urinary tract urothelial carcinoma where the clinical diagnosis was pyelonephritis and non-functioning kidney but it turned out to be an unusual presentation of the tumour involving the entire kidney mimicking renal cell carcinoma but the final diagnosis was high grade invasive urothelial carcinoma with squamous differentiation.
ACKNOWLEDGEMENT: The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript.
Conflict of interest: Nil
Source of funding: Nil
References:
1. Soria F, Shariat SF, Lerner SP, Fritsche HM, Rink M, Kassouf W, et al. Epidemiology, diagnosis, preoperative evaluation and prognostic assessment of upper-tract urothelial carcinoma (UTUC). World J Urol 2017;35(3):379?87.
2. Sarungbam J, Kurtis B, Phillips J, Cai D, Zhang D, Humayun I, et al. Upper urinary tract urothelial carcinoma with intratubular spread. Am J Clin Exp Urol 2014;2(2):102?10.
3. Qi N, Zhang J, Chen Y, Wen R, Li H. Microscopic hematuria predicts lower stage in patients with upper tract urothelial carcinoma. Cancer Manag Res 2018;10:4929?33.
4. Wang LJ, Chou WC, Pang ST, Yang CW, Chuang CK, Chang YH, et al. Risk Stratification of Upper Urinary Tract Urothelial Carcinoma Patients for Survival Prediction: A Simple Summation Scoring Method. J Cancer 2018;9(13):2284?94.
5. Mazzucchelli R, Scarpelli M, Galosi AB, Primio RD, Beltran AL, Cheng L, et al. Pathology of upper tract urothelial carcinoma with emphasis on staging. Int J Immunopathol Pharmacol 2014;27(4):509?16.
6.Makise N, Morikawa T, Kawai T, Nakagawa T, Kume H, Homma Y, et al. Squamous differentiation and prognosis in upper urinary tract urothelial carcinoma. Int J Clin Exp Pathol 2015;8(6):7203?9.
7. Leow JJ, Liu Z, Tan TW, Lee YM, Yeo EK, Chong YL. Optimal Management of Upper Tract Urothelial Carcinoma: Current Perspectives. Onco Targets Ther 2020;13:1?15.
8. Hutchinson R, Haddad A, Sagalowsky A, Margulis V. Upper tract urothelial carcinoma: special considerations. Clin Adv Hematol Oncol 2016;14(2):101?9.
9. Qin C, Liang EL, Du ZY, Qiu XY, Tang G, Chen FR, et al. Prognostic significance of urothelial carcinoma with divergent differentiation in upper urinary tract after radical nephroureterectomy without metastatic diseases: A retrospective cohort study. Medicine (Baltimore) 2017;96(21):e6945.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





