IJCRR - 13(10), May, 2021
Pages: 161-164
Date of Publication: 19-May-2021
Print Article
Download XML Download PDF
A Case Report of a Left-Sided Cerebrovascular Accident with Systemic Hypertension in Elderly Women
Author: Swapna G. Morey, Seema Singh, Ranjana Sharma, Ruchira Ankar
Category: Healthcare
Abstract:Introduction: Most of the time clinicians overlook the diagnosis of cerebrovascular accidents in elderly people. cerebrovascular accident is the most common health problem in India. Three main vessels supply blood to the brain. These vessels are the an�terior cerebral artery, middle cerebral artery and posterior cerebral artery Background: Worldwide, 13.7 million people will experience a hemorrhagic stroke each year. In India, 1.8 million people suffer�ing from a stroke. The incidence of stroke in the general population varies from 154 per 100,000 in India. Case Presentation: A case of 66-year-old women admitted to the medical intensive care unit on date 3 January 2020 with complaints about the inability to talk and weakness over the right half of the body since 2 days after examining the right-side hemiplegia and blood pressure is high 160/100mmof Hg. She had these complaints about about 2 days. Interventions: The patient was treated patient was started on intravenous and orally mannitol,ecosprin and analgesia. She is also under the care of the neurologists as his sodium valproate medication had been adjusted. Treatment consisted of hypertension, therapeutic exercise, and neuromuscular re-education. Conclusion: In this study, we mainly focus on medical management and outstanding nursing care to help prevent further complication. Overall the patient response was good and improvement time after a cerebrovascular accident is different for all people it can take weeks, months, or even years. But few people recover fully, but others have long-term. She takes a long period to recover.
Keywords: Cerebrovascular accident, Elderly women, Hemiplegia, Hypertension, neuromuscular, Therapeutic exercise
Full Text:
??????INTRODUCTION
Worldwide, 13.7 million people will experience a hemorrhagic stroke each year. In India, 1.8 million people suffering from a stroke. The incidence of stroke in the general population varies from 154 per 100,000 in India.1,2 Stroke is the fifth leading cause of death, behind cancer and cardiac disease.3 Approximately, twelve % of all strokes occur below the age of forty-year and slightly more common in males. It is a major cause of mortality and morbidity in the elderly.4 Three main vessels supply blood to the brain. These vessels are the anterior cerebral artery, middle cerebral artery and posterior cerebral artery. In this common long time disabilities add in paralysis, inability to talk, inability to walk and depression.5
Alcohol intake reduction, avoidance of cigarette smoking and exercise of these basic strategies and improvements in lifestyle have a higher potential for prevention of stroke.6 In cases of acute stroke, the study of the cerebral vasculature is very important for vasculature management. To assess the utility of MRA, Vascular occlusion, flow and severity of collateral stenosis.7
CASE HISTORY
Patient information
A case of 66-year-old women admitted in the medical intensive care unit on date 3 January 2020 with complaints about the inability to talk and weakness over the right half of the body since 2 days after examining right-side hemiplegia and blood pressure is high 160/100mmof Hg. She had these complaints about 2 days.
Medical/Surgical History
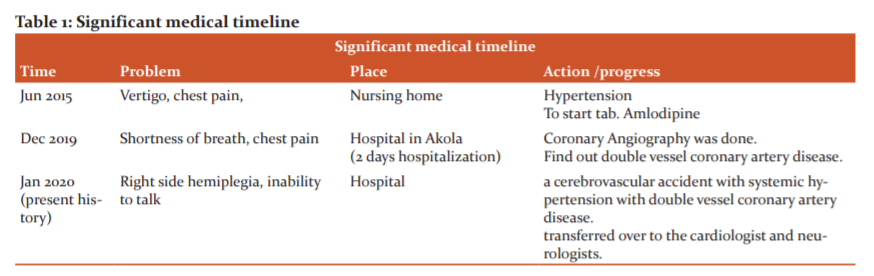
The patient has developed the problem of hypertension before 5 yr. After some investigation did the cerebrovascular accident (CVA) presented initially with the inability to talk, right side hemiplegia. She has a history of hypertension, obesity, anaemia, lower extremity oedema. But the patient underwent coronary angiography done before a few days. She has a double vessel coronary artery disease. No past and present surgical history of the patient. A significant medical problem in the timeline refers to in table 1.
Psychosocial history: She maintains good interpersonal relationships between family member, neighbours, friends and relatives.
Environmental history: Patient home surrounding environment is good. There is a facility of a closed drainage system and proper disposal of waste.
Physical examination
General parameter:
Height : 160 cm , weight : 92 kg , body mass index (BMI) : 35.93
Vital sign : temperature : 99.2 0F , pulse : 60 beat / min , respiration : 16 breath/min , blood pressure: 160/100mmof Hg
Mental status: She was semi-conscious and she had a Glasgow Coma Scale of 11.given the response after the stimulation.
Pulmonary/cardiovascular: Slow pulse rate and sound .respiration also abnormal and blood pressure is high. murmur sound is present.
Integumentary: no skin lesions .dry skin
Musculoskeletal system: She was obese and body mass index (BMI) of 35.93 .slow range of motion (ROM). Muscle weakness is present and a reduction in muscle strength. Periphery oedema in lower extremities.
Speech: inability to talk. sound is present
DIAGNOSIS ASSESSMENT
Blood investigation: In complete blood count (CBC):
Hemoglobin is 10.6 mg/dl(11-13mg/dl) , mean corpuscular hemoglobin concentration is 33.6 g/dl , Mean corpuscular volume (MCV) is 90 fl (78-98 fl ), total RBC count is 3.52 m/ul, WBC is 9200 (4500-11,500 k/ul) ,platelet count is 139,000/ml (150,000 to 450,000 ), Hematocrit (Hct) Levels is 31.7 % (37 %-47 %), monocytes is 03 %(00-15%) , Granulocytes is 74 % ()Lymphocytes is 20 %(20%-40%) , red cell distribution width (RDW) is 10.9 (11.6-14.8) , Eosinophils is 03 % (1-5 %) basophils is 00 % (0-1 % ).
In kidney fuction test (KFT): urea is 36 (9.81 – 20.1 mg/dl) , creatinine is 0.8 mg/dl (0.7-1.4 mg/dl ) ,sodium is 133meq/ l (135-145meq/l) , potassium 4.5(3.5-5.5 meq /l ).
In liver fuction test (LFT): alkaline phosphates is 86 (32-45g/l), Alanine transaminase (ALT) is 34 IU/L (0-50IU/L), aspartate aminotransferase,( AST) is 70 IU/L (10-40 IU/L) ,total protein ia 6.5 (23-38 g/dl) ,total bilirubin is 1.0 g/dl (1-1 g/dl ) ,conjugated bilirubin is 0.2 mg/dl (0-0.25 mg/dl ) ,unconjugated bilirubin is 0.8 mg/dl (0.2-0.7mg/dl) , globulin is 2.8.
In Lipid profile total cholesterol is 159 (200-239 mg/dl ) , triglycerides is 102 mg/dl(150-199 mg/dl) , low –density lipoprotein (LDL) Cholesterol is 94 mg/dl (130-159 mg/dl), high-density lipoprotein (HDL) cholesterol is 45 (35=45 mg/dl).
Calcium is 8.8 mg/dl (8.6-10.2 mg/dl )
Urine examination: Urine albumin is nil, urine sugar is nil, an epithelial cell is 1 cell /hpf.
In peripheral smear, red blood cell (RBC’s) - normocytic normochromic platelets are adequate on smear, seen in clumps no hemiparasite seen.
An electrocardiogram (ECG): An ECG may reveal abnormalities in heart rhythm seen in the ECG.
Brain magnetic resonance imaging (MRI) finding: MRI brain was done. MRI brain showed the suggestive of haemorrhage transformation of acute infarct in left corona radiate and parietal- temporal region corresponding to left middle cerebral artery (MCA).
Fundas examination: In fundus examination was done, which was suggestive of grade II hypertensive retinopathy in both eyes, no evidence of papilla oedema was noted
Therapeutic intervention
General measures: To check the vital sign (Temperature pulse respiration and BP. ) airway, fluid and electrolyte balance and prevention of complications like seizures, pulmonary aspiration, pressure source, thrombophlebitis are mandatory. Health management includes physiotherapy, healthy diet.
Pharmacological management
Antiplatelet agents: Tab aspirin 75mg/day is a non-steroidal anti-inflammatory drug (NSAID) with anti-platelet action, which is used to inhibit platelet aggregation and useful in stroke. To give a low dose in the long term help to irreversible blocks the formation of thromboxane A2 in platelets.
Osmotic diuretic: I nj. Mannitol 100 ml IV. Mannitol is an osmotic diuretic. To reduce of cerebral edema and increased intracranial pressure. To reduce vasogenic cerebral edema.
Antibacterial drug: Inj. Ceftriaxone – 1 gm IV. Ceftriaxone is the third-generation antibiotic from the family of the antibiotic.
Calcium channel blockers: Tab Amlodipin – 5 mg orally, Amlodipineis the calcium channel blocker.
Tab atorin 40mg orally. It is the works by blocking an enzyme (HMG-CoA-reductase) that is required in the body to make cholesterol. It helps for decreased the level of bad cholesterol and increases the level of good cholesterol.
Anticonvulsant drug: InjLevepril 500mg IV , levepril is the anticonvulsant drug. levepril is the help for modulation of the synaptic neurotransmitter release with the help of binding to the synaptic vesicle protein SV2A in the brain.
Proton pump inhibitors (PPIs): Inj. pantoprazole 40 mg IV. Pantoprazole is more effective than H2receptor blockers in reducing gastric acid secretion.
Antiemetic agent:- Inj emeset 4 mg IV . Decreases nausea and vomiting.
Oxygen therapy:- oxygen administration 4 litres/min through a nasal catheter.
Nursing management
First of all makes nursing assessment with the help of observation to check the consciousness, weakness, speech, vital sign, the reaction of a pupil, size of a pupil. To make the client lie comfortably in bed. After checking vital signs ensure patient airway and to given O2 therapy .elevate head end of the bed to 30o and railing bed is provided. To monitor BP.
Nursing diagnosis
1. Impaired physical mobility related to hemiparesis and loss of balance
Goal: to improve and maintain the increased strength and function of affected parts.
Intervention: - to given the proper position and the prone one or twice a day.
2. Impaired airway clearance related to disturbed breathing pattern.
Goal: To improve the breathing pattern
Intervention: assess the respiratory function and implement measures to maintain a patent airway and to improve breathing pattern. To give the prop up position.
3. Impaired nutrition due to less intake.
Therapeutic diet plan
Required the low sodium diet provides 2-3 gm sodium 1600- 1800 calories which give adequate nutrition given. carbohydrate 200gm, protein 60gm fat 40 gm.
Physiotherapy and rehabilitation
Physiotherapy and rehabilitation are useful in the first few months after stroke. exercise, re-education, the provided of walking aids, where appropriate, toe springs adaptation to home.
Communication
Assess the difficulty in using language to communicate or question answer. Encourage the patient's effort to communicate. Speak slowly in simple and also provided consult speech therapists.
DISCUSSION
So many studies indicated that the recovery period within six weeks. If the patient is normal recovery within thirteen weeks. In severe strokes may take twenty weeks. Both cognitive and physical function improved with to help of exercise.8 She has a diagnosis of cerebral vascular accident .systemic hypertension is the secondary diagnosis. the patient gives the respondent well to treatment but the patient relative takes discharge against medical advice (DAMA). As a report of the MRI showing the suggestive of haemorrhage transformation of acute infarct in left corona radiate and parietal- temporal region corresponding to left MCA, the patient had further investigations to find out the cause of hemorrhagic shock.
The patient reacted well to therapy, but more approaches may be used in the future to help in further changes. The rehabilitation and recovery of the patient will mostly depend on the phase of the disease condition. To make improvements and recovery expect the team also requires. In the stroke phase and rehabilitation is dependent on the stage, in stroke management to involves the interprofessional staff and team to manage the patient.
Prognosis
Cerebrovascular accident is a major cause of disability and death. The majority (66%) of stroke that requires hospitalization occur in adults over 65. If the patient has an elderly spousal caregiver who also has health concerns, home maintenance can be a particular challenge. Restricted family members may be living nearby to provide assistance.9,10
Improvement time after a cerebrovascular accident is different for all people it can take weeks, months, or even years. But few people recover fully, but others have long-term. she takes a long period to recover.
CONCLUSION
Hypertension related stroke is a common incident; It is a major cause of mortality and morbidity in the elderly. She fully depends on her family. So health talk taught them the importance of Physiotherapy and its implementation at home after discharge and its usefulness in rehabilitation. Being a health worker it’s an opportunity and responsibility to assist the patient and caregiver in the transition through acute hospitalization, long –term care, rehabilitation, and family requires continuous nursing evaluation and intervention adaptation in response to evolving needs to maximise.
Acknowledgement: The author thanks Dr.Seema Singh, Professor cum Principal, Smt.Radhikabai Meghe Memorial College of Nursing. Datta Meghe Institute of Medical Sciences, Sawangi (M) Wardha for her timely support and valuable suggestions.Mrs. Jaya Gawai, Asso. professor cum academic dean.Mrs.Vaishali Taksande, Professor Dept. of OBGY, The author also thanks Mrs. Archana Maurya, Professor, Dept. of Child Health Nursing. Smt.Radhikabai Meghe Memorial College of Nursing, Datta Meghe Institute of Medical Sciences, (Deemed to be University), Sawangi (M) Wardha, for their continuous support and valuable suggestions. The authors are also grateful to authors/editors/publishers of all those articles, journals and books, from where the literature for this article has been reviewed and discussed. The authors are grateful to the IJCRR editorial board members and the IJCRR team of reviewers who have helped to bring quality to this manuscript.
Ethical approval: Not applicable
Patient Inform consent: While preparing the case report and for publication patient’s informed consent has been taken.
Conflict of Interest: The author declares that there are no conflicts of interest.
Funding: Not applicable
References:
-
Kamalakannan S, Gudlavalleti AS, Gudlavalleti VS, Goenka S, Kuper H. Incidence & prevalence of stroke in India: A systematic review. Indian J Med Res 2017;146(2):175.
-
The stroke disease burden in India has increased nearly 100%?: Indian Stroke Association. 2019 Dec 20; https://health.economictimes.indiatimes.com/news/industry/the-stroke-disease-burden-in-india-has-increased-nearly-100-indian-stroke-association/72895241
-
Becheva M, Georgiev D. Functional Recovery of Patient Whit Ischemic Stroke: Case Report. Iranian J Public Health 2017;46(11):1579-7.
-
Kayla A. A Case Report: Cerebrovascular Accident. Phys Ther Scholarly Projects 2016;576.
-
Brenner I. Effects of Passive Exercise Training in Hemiplegic Stroke Patients: A Mini-Review. Sports Med Rehabil J 2018;3(3):1036.
-
Agrawal A, Joharapurkar SR, Gharde P. Ischemic stroke in a child mistaken as a functional disorder. Clin Neurol Neurosurg 2007;109(10):876-9.
-
Kumar RJ. Ischemic stroke: relevance of magnetic resonance angiography (mra) findings and correlating the changes with various conventional and nonconventional risk factors. Int J Curr Res Rev 2014;06(01):72–8.
-
Sunderland A, Tinson DJ, Bradley EL, Fletcher D, Hewer RL, Wade DT. Enhanced physical therapy improves recovery of arm function after stroke. A randomised controlled trial. J Neurol Neurosurg Psychiatry. 1992 Jul 1;55(7):530-5,
-
Lewis SM. Lewis's Medical-surgical Nursing: Assessment and Management of Clinical Problems. Elsevier Australia; 2009.
-
Black JM, Hawks JH, Keene AM. Medical-surgical nursing: Clinical management for positive outcomes. WB Saunders Co; 2001.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





