IJCRR - 13(10), May, 2021
Pages: 142-146
Date of Publication: 19-May-2021
Print Article
Download XML Download PDF
Effect of Motor Dual-Task Training Over Progressive Resisted Exercises on Balance and Mobility in Elderly People
Author: Sarulatha Haridass, M. Manikumar, Vasanthan Rajagopalan, R. Vijayaraghavan, Ramesh Kumar Jeyaraman
Category: Healthcare
Abstract:Background: The older adults' population is rapidly growing and projected to be 198 million in 2030, which means greater demand on the health care system to sustain and improve the quality of life. The international report of the World Health Organization declared that the elderly above 65 years have 28% to 35% of falls every year and this rate rises with growing age and associated risk factors. Falls cause reduced confidence, mobility, major injuries, decreased functional status and increased dependency in older adults. Hence the need to explore an effective exercise program for the elderly to improve their functional abilities. Objective: To analyse the effects of motor dual-task training over progressive strength training in older adults with impaired balance. Methods: This is Randomized pilot study. The elderly participants aged between 60 to 75 years from residential care facilities were randomly allocated to 2 groups, (12 in each). One group received motor dual-task exercise (MDT) and the other group received progressive resisted exercises (PRE), for a total of 24 sessions. The effects of MDT and PRE on balance and mobility were analysed using Performance-oriented mobility assessment (POMA) scale. Results: It was observed that the motor dual-task training group showed better improvement in balance and mobility measures. (p< 0.001) Conclusion: This pilot study gives insight into the benefits of motor dual-task training in improving mobility and feasibility of inclusion in geriatric rehabilitation. Further research to investigate effects of PRE and MDT exercises on other functional par
Keywords: Strength training, Falls, Gait, Older adults
Full Text:
INTRODUCTION
Ageing progressively declines movements and functions, thereby impacting muscle strength, endurance and power. By 2025, the geriatric population is expected to be 840 million in developing countries.1 The distribution of elderly aged 60 and above is projected to increase from 7.5% in 2010 to 11.1% in 2025. The elderly population in India is expected to reach 158.7 million in 2025 eventually increasing the burden on the resources of the country.2
Elderly people are vulnerable to functional impairments. Common activities like rising from the chair, reaching top shelves, activities requiring postural responses, functional activities like walking, climbing stairs becomes challenging and risky. The impaired mobility and muscle strength gradually lead to loss of balance, body instability and increases the risk of falls. The reductions in the important physical components due to ageing have to be identified at the earliest to prevent & control essential physical losses. The uses of various physical exercises in enhancing functional activity in older adults have been the focus of recent research. The exercise protocol requires the inclusion of the best possible combination of training parameters to improve musculoskeletal, neurological & cardiovascular adaptations which can help cope with the functional activity.
Strength training was found to be one of the important exercise components recommended in kinds of literature. But the use of strength training as the stand-alone protocol for elderly subjects is still debated and is an area of interest for many researchers. Moreover, the exercise protocol needs to address the root cause of functional limitation and the important factors like muscle strength, balance, postural control, cognition etc,.3 Falls in the older age group has a debilitating effect on mobility, confidence in performing activities of daily living (ADL), resulting in institutionalization and escalation of economic costs4 and hence it’s imperative to develop an effective exercise protocol for a better quality of life in the elderly.
Most of the functional activities and ADL require performance of a motor task, postural control & cognitive function simultaneously, probably with the role of recognition and concentration as a part of motor learning.5 It has been reported that older subjects have difficulty in performing the dual task at the same time like walking and balancing activities.6 Few studies highlighted the importance & benefits of dual-task balance training, in the prevention of falls in elderly people.7
Due to the dearth of studies within the context of literature searched, the contribution and the effectiveness of strength training and dual-task exercises in improving balance and mobility which are the cardinal element of functional activity in the elderly population eventually resulted in the scope of the present study. We aimed to study the feasibility to analyse the effect of motor dual-task exercises and progressive resisted exercises on balance & mobility improvements in the elderly.
MATERIALS AND METHODS
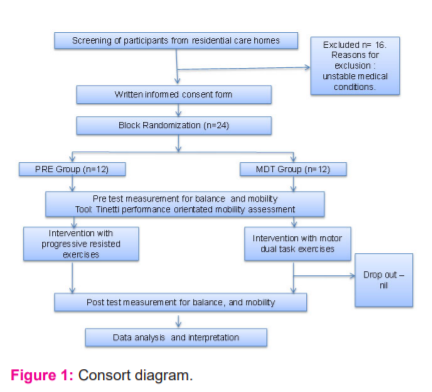
This was a randomized pilot study conducted in elderly from residential care homes. Ethical clearance was obtained from the institutional human research & ethical committee(001/03/2016//IEC/SU). The participants were recruited from residential elderly care centres, who volunteered and were willing to take part in the study. Written informed consent was obtained from all the participants. Nearly 12 participants were recruited in each group.
Inclusion criteria
Elderly aged between 60 to 75 years of both genders, who were able to ambulate at least 5m with/without aide and able to stand independently for 1 min without support, POMA score of 24 and less were included. The cognitive status was assessed to ensure that the subjects were mentally competent to perform the exercises safely, understand and respond appropriately to the tests and questionnaires used as outcome measures.
Exclusion criteria
Participants with unstable medical conditions and with significant visual or auditory impairments, vestibular disorders, severe pain on weight-bearing during activity with musculoskeletal disorders of the lower extremity, who underwent regular exercises for lower limb strength and/or balance training in the past 3 months and conditions like stroke, Parkinson’s disease, cancer were excluded.
The baseline data on age, sex, BMI, no of falls, presence of physical discomfort were recorded and preserved for data analysis before randomly allotting them into the groups. The pre-test data on balance and gait using POMA were collected before beginning the intervention and post-treatment (at the end of 8 weeks of intervention). The participants were allotted using block randomization, each containing 4 sealed envelopes (2 PRE, 2MDT). The allocation concealment was done using sealed opaque envelopes which were sequentially arranged. The sealed envelopes were opened by the investigator who was blinded to the intervention.
Participants in both groups underwent 8 weeks of supervised exercise training. Each exercise program consisted of 3 sessions per week and hence underwent a total of 24 sessions. Each session consisted of warm-up exercises for 10 mins (Stretching of major lower limb muscles), followed by main exercises (respective to their allotted groups) for 40 mins and cool-down exercises for 10min similar to warm-up exercises.
Motor dual-task exercises included challenging the balance tasks with upper limb manipulation, change in the base of support, activities on complaint surface and progressed from standing to walking. The participants started the exercises by normal standing, standing with a narrow base of support like standing with feet together side to side, semi tandem standing, tandem standing, weight shifts with active ankle rolling in normal stance and tandem stance, one leg standing with palm supported on the wall and later off the wall. The above exercises were performed in normal stance and tandem stance with arm movements to the lateral side (shoulder joint abducted to 90 degrees) and anterior side (shoulder flexion in 90 degrees) and with closed eyes. The participants then progressed to standing on the foam. The next sets of exercises were walking, semi tandem and tandem walking with their comfortable speed for a 4 m distance, walking with changing the directions, varying the speed and with alternating hand motions. The participants performed normal walking and progressed to tandem walking on the foam, combined with alternating hand movement 7. Further during walking the participants were trained to do secondary task performance like holding a cup of water and walking, receiving and returning the cup of water, walking while talking to a person, walking with tossing and catching the ball 5. Transferring from one chair to another on the side and in front was also practised by the participants with and without the use of the arms. The participants were able to effectively perform the challenging dual-task exercises after 8-12 sessions. So, they were made to focus and practice with the difficult level of dual-task exercises. A rest period of 2-3 mins was given after 15-20 mins of exercises.
The PRT group received resisted exercise for the key muscles of both the lower limb. The targeted muscles for strengthening were Hip flexors, extensors, abductors, knee flexors and extensors, ankle dorsi -flexors and plantar flexors 8. The external load was given through weight cuffs tied above the ankle joint, except for the ankle plantar and dorsi flexors it was secured around the foot. In the first week of training, participants were trained at 30 % of their 1RM and gradually increased to reach 80 % of the 1RM by the final week, as tolerated by the participants. 1RM was reassessed every 2 weeks. The PRE program consisted of 1 set of 8-10 repetitions for each muscle group during each session, with 3 sessions per week for a total of 8 weeks 9. A rest period of 1min was allowed between each set of training. The participants were instructed to not hold the breath while performing exercises. The lifting and lowering of the weight during every repetition facilitated concentric and eccentric muscle action. The participants of the PRT group had slight muscle discomfort and soreness during the initial sessions and they were treated symptomatically.
Statistical analysis
The statistical analysis was done using SPSS statistics version 26. Baseline homogeneity for outcome measures was established by an independent t-test. POMA scale was analyzed using a non-parametric test. Independent t-test was used for between-group analysis and paired t-test used for between-group analysis with 95% confidence level with a significance level of p<0.05. The pre-test data for total POMA scores and its sub-domains balance and gait did not show a significant difference in both the groups.
RESULTS
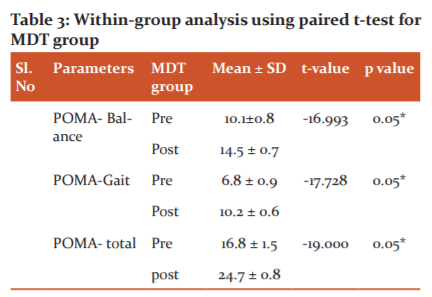
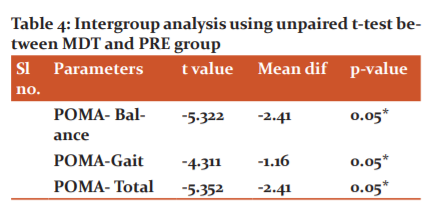
Among the total number of 24 participants, there were 12 males & 11 females. Demographic details are shown in (Table 1). The samples were homogenous in both groups. The intragroup analysis showed significant improvements in the POMA total scores and POMA-balance and POMA–gait in PRE group (Table 2) and in the MDT group (Table 3). The motor dual-task training showed slightly more significant improvements in balance and gait compared to the PRE group. (Table 4).

DISCUSSION
Muscle weakness in the lower extremity is a distinguished and hazardous factor resulting in falls.8 Studies have shown a strong relationship between lower limb muscle strength and balance. Various groups of muscles in the lower extremity contribute to the maintenance of static and dynamic balance. The changes in the muscle morphology significantly reduce the force production and torque-time production which in turn affects the functional performance. Flexors of both knee and ankle are the key muscles for balance and postural control.9,10 Several studies have demonstrated that, with progressive and sufficient external stimulus, the elderly show similar or greater strength gains compared to young adults11.
In this study, the positive effect of PRT on balance measures may be attributed to targeted strength training of the key muscles like flexors, extensors and abductors of the hip, flexors and extensors of the knee, dorsi flexors and plantar flexors of the ankle in a structured and progressive manner required to maintain balance. Inability to target the key muscles and exercise intensity variability observed in few studies may have resulted in poor performance for balance and gait.12,13 In addition, the effects on the balance due to strength gain could also be due to neural adaptations. During the early phase of strength training, the gain is mainly due to neural rather than structural adaptations. Neural adaptations such as the increment of motor neuron firing rate increased neurotransmitter release at the neuromuscular junction, re-sensitization of sensory receptors for improved proprioception14 may have adequately contributed to improved balance in the PRE group.
Resistance training appeared to be effective in improving strength in older people, but there was statistical heterogeneity in the effects. In addition, PRE appeared to be less effective in older adults with functional limitation than older adults without functional limitations. Data pooled from 17 studies with 996 participants showed a small but non-significant benefit for balance. Few studies analyzed the effect of PRE on balance and showed improved muscle strength and not the balance parameters. The strong predictor for balance and stability which is Chair rise time and gait speed did not improve with PRT.3
Motor training including balance and strength training are known to improve dual-task performance in older adults.15 The existing dual-task training studies combining motor and cognitive tasks reported improvement in cognitive performance under dual-task conditions. However, they differ in their outcomes due to their training design, protocol and methodology. Studies reported significant improvement in balance components and marked heel strike with improved foot rolling movements16, decreased step width, increased step length & more stabilized gait pattern, smooth weight shifts during walking with dual-task training.16 The results of the present study are similar to the previous studies reporting improvements in balance, improved walking ability and gait patterns with proprioceptive-balance motor dual-task training.6
The performance of dual task improved balance with decreased postural sway and improved postural stability17.Studies explained the reasons behind improvement of balance and postural control with dual task training as the ability to augment external focus of attention and concentration on the result of the movement than the internal focus of attention, concentration on the movement itself.18. Studies on chronic stroke subjects examined the effect of a dual-task program on the gait performance and found that gait parameters significantly improved of the motor dual-task training.19 Studies involving dual-task performance of balance-related tasks also indicate improvements following dual-task training in both healthy older adults and those with chronic stroke.19,20 Balance training under single-task conditions and dual-task conditions with fixed priority instructions (equal attention to posture and cognitive tasks) or variable priority instructions (attention switched between posture and cognitive task) showed improved gait speed under dual-task conditions with dual task training.21
Following the premise that fallers are not able to prioritize gait performance.22 The motor dual-task program intends to introduce the task switching from a cognitive task to a walking task and hence improves the allocation of resources for motor performance in dual-task conditions. Exercises with progressively increased difficulty levels assist the participants to learn, execute, and transfer these strategies during the training sessions, also considered essential for falls prevention.7 Elderly individuals demonstrate impairment in higher cognitive task performance during motor tasks. Enhancing dual-task training knowledge is highly essential, as most activities of daily living involve the performance of more than one task at a time.
The results of the present study demonstrate significant improvement in balance and gait with motor dual-task exercises and PRE training. However, a statistically significant difference was observed with motor dual-task exercises than PRE in increasing the balance and walking abilities in elderly with impaired balance. The cognitive component associated with motor activity balance training practised by the participants in the present study would have particularly impacted the dual-task interface in the elderly, which is the most essential area of focus in targeting the balance issues and functional performance.
CONCLUSION
Both groups (MDT & PRT groups) showed improvements in balance and mobility performance in elderly participants. However, comparing the two interventions, motor dual-task exercises had significantly higher change scores and hence yielded greater improvements in elderly with impaired balance. Further, the motor dual-task exercises with progressively challenging cognitive and motor (balance) training prescribed in the present study is an important contributing factor for the dual-task performance required during the functional activities.
Acknowledgement: The authors do not have any conflict of interest (financial or other) and there was no funding for this study. The authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
Source of Funding: None
Conflict of Interest: None
References:
1. Mane A. Ageing in India: Some Social Challenges to Elderly Care. J Gerontol Geriatr Res 2016;05(02).
2. Dey S, Nambiar D, Lakshmi JK, Sheikh K.The health of the Elderly in India: Challenges of Access and Affordability. National Research Council. 2012. Ageing in Asia: Findings from New and Emerging Data Initiatives. Washington, DC: The National Academies Press.
3. Liu C-J, Latham NK. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst Rev 2009;2009(3):CD002759.4.
4. Soriano TA, DeCherrie L V., Thomas DC. Falls in the community-dwelling older adult: a review for primary care providers. Clin Interv Aging 2007;2(4):545-554.
5. An HJ, Kim JI, Kim YR, Lee KB, Kim DJ, Yoo KT, et al. The Effect of Various Dual-Task Training Methods with Gait on the Balance and Gait of Patients with Chronic Stroke. J Phys Ther Sci 2014;(26):1287–1291.
6. Shin SS. The Effect of Motor Dual-task Balance Training on Balance and Gait of Elderly Women. J Phys Ther Sci 2014;12:2-4.
7. Wollesen B, Schulz S, Seydel L, Delbaere K. Does dual task training improve walking performance of older adults with concern of falling? BMC Geriatr 2017;17(1):1-9.
8. Trudelle-Jackson EJ, Jackson AW, Morrow JR. Muscle Strength and Postural Stability in Healthy, Older Women: Implications for Fall Prevention. J Phys Act Health 2016;3(3):292-303.
9. Heyn PC, Johnsons AFK. Endurance and Strength Training Outcomes on Cognitively Impaired and cognitively intact older adults: A Meta-Analysis. J Nutr Heal Aging 2008;12(6):401-409.
10. Hess JA, Woollacott M. Effect of high-intensity strength-training on functional measures of balance ability in balance-impaired older adults. J Manipulative Physiol Ther 2005;28(8):582-590.
11. Lang T, Streeper T, Cawthon P, Baldwin K, Taaffe DR, Harris TB. Sarcopenia: Etiology, clinical consequences, intervention, and assessment. Osteoporos Int 2010;21(4):543-559.
12. Bunout D, Barrera G, Avendaño M, de la Maza P, Gattas V, Leiva L, et al. Results of a community-based weight-bearing resistance training programme for healthy Chilean elderly subjects. Age Ageing 2005;34(1):80-3.
13. Vogler CM, Sherrington C, Ogle SJ, Lord SR. Reducing Risk of Falling in Older People Discharged From Hospital: A Randomized Controlled Trial Comparing Seated Exercises, Weight-Bearing Exercises, and Social Visits. Arch Phys Med Rehabil 2009;90(8):1317-1324.
14. Peterson CR. Acute neural adaptations to resistance training performed with low and high rates of muscle activation. Diss Abstr Int Sect B Sci Eng 2009;70(5-B):2746.
15. Hall CD, Echt K V., Wolf SL, Rogers WA. Cognitive and motor mechanisms underlying older adults’ ability to divide attention while walking. Phys Ther 2011;91(7):1039-1050.
16. Perry J, Judith M. Burnfield. Gait Analysis: Normal and Pathological Function. Slack Incorporated, New Jersey, 2010.ISBN: 978- 1556427664,
17. Hyndman D, Ashburn A, Yardley L, Stack E. Interference between balance, gait and cognitive task performance among people with stroke living in the community. Disabil Rehabil 2006;28(13-14):849-856.
18. Gabriele W, Prinz W. Directing Attention to Movement Effects Enhances Learning: A Review. Psychon Bull Rev 2001;8(4):648–60.
19. Yang YR, Wang RY, Chen YC, Kao MJ. Dual-Task Exercise Improves Walking Ability in Chronic Stroke: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2007;88(10):1236-1240.
20. Doumas M, Rapp MA, Krampe RT. Working memory and postural control: Adult age differences in potential for improvement, task priority, and dual tasking. J Gerontol Ser B Psychol Sci Soc Sci 2009;64(2):193-201.
21. Silsupadol P, Shumway-Cook A, Lugade V. Effects of Single-Task Versus Dual-Task Training on Balance Performance in Older Adults: A Double-Blind, Randomized Controlled Trial. Arch Phys Med Rehabil 2009;90(3):381-387.
22. Schaefer S, Schumacher V. The interplay between cognitive and motor functioning in healthy older adults: Findings from dual-task studies and suggestions for intervention. Gerontology 2011;57(3):239-246.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





