IJCRR - 7(24), December, 2015
Pages: 39-42
Date of Publication: 20-Dec-2015
Print Article
Download XML Download PDF
MORPHOMETRIC ANALYSIS OF EXTENSOR GROOVE OF LOWER END OF RADIUS
Author: K.C. Shanthi
Category: Healthcare
Abstract:Background: The tendons of Abductor pollicis longus and Extensor pollicis brevis pass through the first compartment of the extensor retinaculum. These tendons pass with their own synovial sheaths and sometimes they share a common synovial sheath which can be septate. Constant friction between these tendons in a living person results in tenosynovitis.
Aim: This study aimed to document the relationship between the tendons and the bone and variations in the tendon or the bone could produce any significant contribution to the outcome of disease. Materials and Methods: 100 radius bones of both sides were sourced for the study to measure the length, breadth and depth of the extensor groove using a Vernier caliper and the same were documented. Results: The mean length, breadth and the depth of the grooves were more on the right side than the left side. In a significant percentage, the ridge was absent. Conclusion: The morphometric data will provide an insight for corrective surgeries in tenosynovitis and for corticosteroid injections in cases of tenosynovitis.
Keywords: Groove, Ridge, Tenosynovitis, Radius, Extensor retinaculum, Tendons
Full Text:
INTRODUCTION
Pain around the wrist joint is a common complaint in elderly people. This pain can be due to various causes including trauma around the wrist. This pain can also be perennial which is accentuated by metabolic disorders also. A common cause of this pain is De Quervain’s tenosynovitis whose aetiopathology is very unclear. It is encountered in everyday clinical practice1 . This condition limits the activities of daily living in an individual. This condition is brought about by repetitive and sustained tension on the tendons of the first dorsal compartment4 . The treatment of this condition is initially by analgesics to relieve the pain and if it fails, it is followed by surgery. It is hypothesized that this condition is due to compression of tendons of Abductor Pollicis longus and Extensor Pollicis Brevis when they pass through the first compartment of the extensor retinaculum of the wrist. These tendons are covered by their own synovial sheaths when they are passing. However in rare instances, both these tendons might share the same synovial sheath6 . Constant friction between the tendons, their synovial sheaths and their opposing bone contributes to tenosynovitis. Awareness of this condition will make the treatment of De Quervain’s tenosynovitis more effective2 . Anatomically these tendons are lodged in a groove which is separated by a bony ridge, dividing the compartment into two paths (Fig-1). The depth and length of these paths of the tendons determines the rate of friction of the tendons when these muscles are put into movement. If the canals that house these tendons are deep the movement is usually smooth and if the groove is shallow the chances of compression of the tendons is all the more a possibility. In some instances the canals may not be present at all (Fig-2). Textbooks describe that the two tendons of Abductor Pollicis Longus and Extensor Pollicis Brevis pass through the first compartment of the extensor retinaculum and they may possess separate or single synovial sheaths. Sometimes there exist two separated compartments for the abductor pollicis longus and extensor pollicis brevis tendons3 Frequently the tendon of Abductor Pollicis longus may be duplicated.
Tenosynovitis of the tendons is due to palpable thickening of the synovial sheaths which also causes painful extension of the thumb. Though numerous studies have been done on the extensor retinaculum to determine the position of the tendons of Abductor Pollicis Longus and Extensor Pollicis Brevis and its accessory slips, no morphometric analysis has been done to elicit the dimensions of the first groove of the extensor retinaculum.
MATERIALS AND METHODS
This study was performed in the Department of Anatomy, VMKV Medical College, Salem. 100 radius bones were sourced for the study. Sex was not determined for the bones. Among the bones 50 bones belonged to the right side and 50 bones belonged to the left side. A hand lens was used for closer observation. A divider and measuring scale was used to morphometrically analyze the bones. The following parameters were measured 1) Presence or Absence of bony ridge 2) Length of the bony ridge 3) Length of the Lister’s tubercle 4) Length of the bony canals 5) Breadth of the bony canals
METHODOLOGY
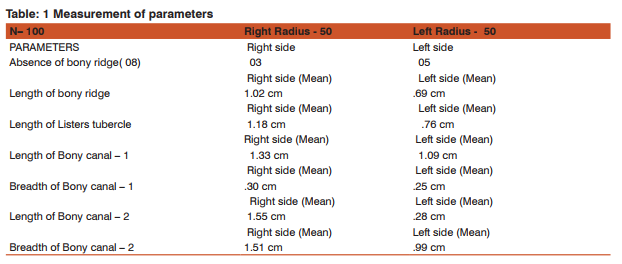
Using a hand lens the bones were observed for presence or absence of bony ridges. Out of the 100 bones, 08 bones exhibited no ridge. The length of the Lister’s tubercle (L1) was measured from the tip of the inferior border (Point A) to the uppermost tip of the tubercle (Point B). The length of the bony ridge (L2) was measured from its lower end (Point C) to its upper end (Point D). Length of the bony canal 1(l1) was measured from the tip of the inferior border (Point E) to the tip of the uppermost end (Point F). Length of the bony canal 2 (l2) was measured from the tip of the inferior border (Point G) to the tip of the uppermost end (Point H) (Fig – 3). The breadth of the bony canals was measured as the maximum width from a midpoint of the length of each bony canal (B1, B2) (Fig – 4). The first canal is present between the listers tubercle and the bony ridge. The second canal is present between bony ridge and the palmar tubercle. Statistical Analysis The resultant measurements were statistically analyzed using SPSS software version 17.
RESULTS
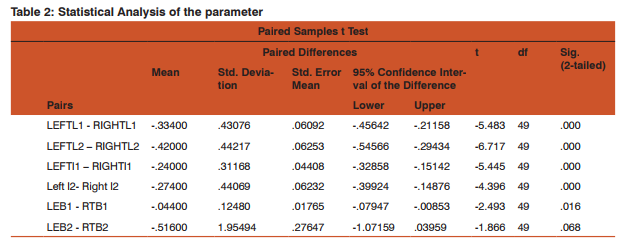
Among the 100 radii examined, 08 bones did not have bony ridge with the left radius being predominantly higher than the right radius. The mean length of the bony ridge of the right side was more than the mean length of the left radii. The mean length of the listers tubercle of the right side was more than the left side. The mean length and breadth of the first bony canal on the right side was more than the left side. The mean length and breadth of the second bony canal on the right side was more than the left side. The parametric measurements of the right and left radii are given in Table -1. The resultant parameters were statistically analyzed through a paired sample’t’ test which is depicted in Table 2.
DISCUSSION
The bony ridge was absent in about 8% of the bones. This absence of bony ridge does not separate the tendons of Abductor Pollicis longus and Extensor Pollicis Brevis. It can be assumed that there may or may not be a separate synovial sheath which can contribute to the friction between the tendons. The length, breadth of the ridge as well as bony canals measurements were significantly higher on the right side than the left side. This can be due to the fact that the bones could be belonging to the right handed individuals predominantly than left handed persons. In a study conducted in the year 2012 states that specific geometrical parameters of the styloid process of the radius need to be measured and compared between different types and sides of the body5 which has been done in the present study. The deep canals on the right side may due to the usage of the limb resulting in constant wear and tear of the tendons during the movements of the wrist. In some of the bones both the canals were deeply grooved indicating that the movements of the tendons had produced them. The friction between the tendons in the absence of a groove or ridge will cause difficulty in activities of daily living in an affected person. Normal movements of the wrist will be impeded. Also movements of the tendons within their respective synovial sheaths might produce pain and multiple compartments may also predispose to De Quervain’s Tenosynovitis7 . When the synovial sheath is shared, it results in tenosynovitis.
CONCLUSION
Knowledge of the ridge and its morphometry and its variations will be useful for practicing surgeons in performing surgeries to release the tendons from their synovial sheaths in cases of entrapment. Direction of the needle within the septate tendon sheaths while giving corticosteroid injections in cases of tenosynovitis is of prime importance and variations of the ridge and the bony canal can point a right path for the drug to be injected.

ACKNOWLEDGEMENTS
The authors sincerely wish to thank the management, administrators and the Professor and Head of the department of Anatomy of Vinayaka Missions Kirupananda Variyar Medical College, Salem for their whole hearted support and permissions to utilize their resources and conduct this study. The authors acknowledge the great help received from the scholars whose articles cited and included in references of this manuscript. The authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed. Authors are grateful to IJCRR editorial board members and IJCRR team of reviewers who have helped to bring quality to this manuscript.
References:
1. Green D. Operative Hand Surgery. 5th edition. Churchill Livingstone: Elsevier, New York; 2005: 2150.
2. Manoj M Kulkarni, A Ashok, Are Indians more prone for De Quervain’s tendinitis in Indian Journal of Basic and Applied Medical Research: June 2014: Vol.-3, Issue-3, pages 212-215.
3. Jamal Gousheh et al; Division of the First Dorsal Compartment of the Hand into Two separated canals: Rule or Exception? In Archives of Iranian Medicine, Vol-12, Number 1, 2009: 52-54.
4. Asif Iliyas et al; de quervain Tenosynovitis of the wrist In Journal of the American Academy of Orthopaedic Surgeons, Vol-15, Number 12, December 2007: 757-764.
5. Liang Xiao et al; Variations in the extensor grooves of the radial styloid process in Chinese population In Surgical and Radiologic Anatomy, Springer-Verlag 201210.1007/s00276-012-0995-y.
6. Susan Standring in Gray’s Anatomy: 40th edition: Churchill Livingstone: Elsevier, London; 2008: pages 879 – 880.
7. Soubhagya R. Nayak et al; Variations and Clinical Significance of Extensor Pollicis Brevis: A study in South Indian Cadavers; Chang Gung Med J 2009; 32: 600-4.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





