IJCRR - 13(10), May, 2021
Pages: 125-132
Date of Publication: 19-May-2021
Print Article
Download XML Download PDF
Correlation of HbA1c with Solid Organ Tumours in the Non-Diabetic Individuals - A Cross-Sectional Study
Author: Chodavarapu Dheeraj, Girish M
Category: Healthcare
Abstract:Introduction: Diabetes is described by unending hyperglycemia and causes long haul difficulties like retinopathy, neuropathy, and nephropathy. Most of the cancers in diabetes are associated with high blood glucose levels. An increase in glucose uptake can activate oncogenic pathways in cells, so this provides information that another pathway by which hyperglycemia increases cancer incidence risk. Objective: To correlate HbA1c with solid organ tumours in non-diabetic individuals. Methods: A cross-sectional study with convenient sampling. An HbA1c test was done for all the patients who were diagnosed with solid organ tumour at the time of admission and values were noted and HbA1c test was done for age and sex-matched otherwise healthy individuals and the values were noted. We compared the HbA1c values of each case and control. Any case or control with an HbA1c level above 6.5 was excluded from the study. Results: The mean HbA1c among the cases was 5.578 whereas among the controls was 5.303 and the p value is Significant (< 0.001).t-Value-3.597. The near-linear association of HbA1c levels with the risk of several cancers supports the conjecture that it might be possible to use HbA1c as an independent metabolic biomarker for cancer risk in diabetic or non-diabetic persons. Conclusion: It is a known fact that patients with diabetes are at increased risk of cancer but even in non-diabetics if the blood glucose levels are high they are also at increased risk of cancer. The risk is higher with Lung cancer, Colo-rectal cancers, Ovarian tumours and Gall bladder tumours. On the contrary patients with prostate cancer had lower HbA1c levels.
Keywords: HbA1c, Solid organ, Tumours, Non-diabetic, Correlation, HbA1c
Full Text:
INTRODUCTION
Diabetes is described by unending hyperglycemia and causes long haul difficulties like retinopathy, neuropathy, and nephropathy.1,2 It for the most part quickens full scale and miniaturized scale vascular changes. Due to way of life changes (i.e., eating increasingly and practising less), diabetes has turned into a worldwide pestilence. Proficient and compelling aDiabetesinistration is required to deal with this pestilence.3-5 Convenient glucose meters encourage the fleeting a Diabetesinistration of diabetes.6 Long haul forthcoming investigations, prominently the Diabetes Control and Complications Trial (DCCT), the UK planned Diabetes Study Group (UKPDS), and the Epidemiology of Diabetes Interventions and Complications (EDIC) think about, have given clear proof that diabetic intricacies are specifically identified with mean glycemia esteem, as estimated by the HbA1c focus. It is, in any case, not clear whether hyperglycaemia, a sign of diabetes, connects with expanded malignancy hazard autonomous of diabetes.7-10 On the off chance that such affiliation exists, at that point the growth chance in people with glucose levels lower than that required to analyze diabetes may as of now be expanded. The relationship of most tumours and diabetes with constant aggravation and the immediate connection between expanded incendiary flagging and high blood glucose levels in disease models bolster the likelihood that incessant hyperglycaemia may have an essential part in growth chance in people. The expanded creation of endogenous hormones can likewise be by implication connected to hyperglycaemia using hyperinsulinaemia and weight, and, consequently, additionally to diabetes and malignancy hazard. Constant hyperglycaemia in diabetes patients is by all accounts specifically connected with the omnipresent dependence of most tumour cells on high glucose flux. It was discovered that an expansion in glucose take-up can enact oncogenic pathways in breast cells.11 This could conceivably give another pathway by which hyperglycaemia builds tumour frequency hazard. Constant hyperglycaemia might be assessed by estimating glycated haemoglobin (HbA1c) (American Diabetes Association, 2013), a biomarker of the normal blood glucose focus for a drawn-out timeframe. Vitally, HbA1c may likewise be a decent marker of metabolic procedures affecting levels of insulin or insulin-like development factors, essential for growth pathogenesis.12,13 Most investigations centre around the relationship between tumour hazard and diabetes. No meta-investigation has yet been distributed that unites the danger of various kinds of tumours with various HbA1c ranges, including glycaemic levels lower than that related to diabetes. If tumour hazard is brought down at low HbA1c levels, at that point the frequency of malignancy in the diabetic and non-diabetic populaces could be brought down by diminishing glucose levels.14 This could be accomplished by methods for a suitable way of life or helpful intercessions, and by forcing stricter proposals for glycaemic control. However even though Warburg had guessed that the metabolic move to glycolysis is "the source of disease cells", the showing of causative impacts of the expanded glucose take-up and digestion on oncogenesis has evaded the field up until now.
Conversely, the possibility that glucose level itself can trigger intra-and intercellular flagging is acknowledged and considered generally in the fields of endocrinology and diabetes. Glucose flagging is known to be connected to physiological and obsessive occasions, for example, control of hormone emission and insulin opposition. In the present we aimed to study the association of HbA1c levels with solid organ tumours in non-diabetic individuals. We have assessed the correlation between HbA1c levels and occurrence of solid organ tumours in non-diabetic individuals and compared the risk of solid organ tumours in Normal individuals versus Prediabetics with HbA1c levels.
MATERIALS AND METHODS
This is a Cross-sectional study done at Tertiary care hospitals attached to KASTURBA MEDICAL COLLEGE (Manipal Academy of Higher education), Mangalore has done between September 2016 to September 2018. Non-diabetic patients with solid organ tumours admitted to the hospital. Otherwise, Age and Sex matched healthy individuals from the community were taken as the control group for the study.
It was a Convenient sampling and the sample size was taken With a 95% confidence level and 90% power concerning the previous study6 by assuming the same proportion the sample size comes to be 160.By adding 10% error for the sample size and taking cases and controls as 1:1 ratio my sample size increases to 180 (cases: 90 and control: 90)
n = 2(Zα+Zβ) × σ2
d2
Zα =1.96 (95% confidence interval)
Zβ =1.28 (90% power)
σ =standard deviation
d = mean difference from the previous study
Ethical Clearance number: IEC KMC MLR 09-16/199
Procedure
All Solid-organ tumour patients admitted to hospitals attached to Kasturba Medical College, Mangalore who satisfied inclusion/exclusion criteria were included in the study. The data collection included demographic details, detailed medical history, history regarding the present event, the details of the medications received by the patients with the details of steroids and other hyperglycemia causing agents used, physical examination findings etc. The details regarding comorbid conditions were recorded and any change in the intervention and clinical status was recorded. An HbA1c test was done for all the patients who were diagnosed with solid organ tumour at the time of admission and values were noted and HbA1c test was done for age and sex-matched otherwise healthy individuals and the values were noted. We compared the HbA1c values of each case and control. Any case or control with an HbA1c level above 6.5 was excluded from the study. HbA1c test was done by High-Performance Liquid Chromatography (HPLC) method from the Kasturba Medical College (BIOCHEMISTRY DEPARTMENT)Collected data were coded and entered into SPSS 17.0. Categorical variables are described by frequencies and percentages, and continuous variables by mean±Standarddeviations. Chi-square test, ANOVA test and Paired t-test were used. Figures and tables are used to summarize the results. p <0.05 was taken as significant.
RESULTS
In this study, we enrolled a total 180 study population of which 90 are cases (Solid-organ tumours without Diabetes) and 90 controls (otherwise healthy individuals). All the cases are above 18yrs age with biopsy-proven malignancy. It is a cross-sectional study comparing the HbA1c between the two study groups. The statistical results are as follows (Table 1).
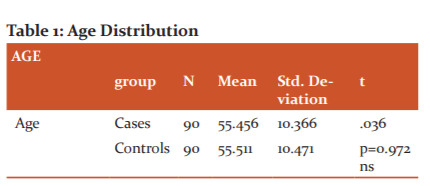
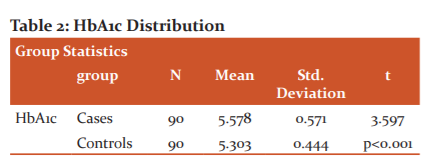
The above table shows the age distribution between the two groups. The mean age among the cases is 55.45 and that of controls is 55.51 and the p-value (0.97) was not significant meaning that Age-wise the study population is evenly distributed among the two groups. The HbA1c test was done using the High-performance liquid chromatography method (HPLC). This is the gold standard method available for the measurement of HbA1c. The mean HbA1c among the cases was 5.578 whereas among the controls was 5.303 and the p value is significant (<0.001)( Table 2).
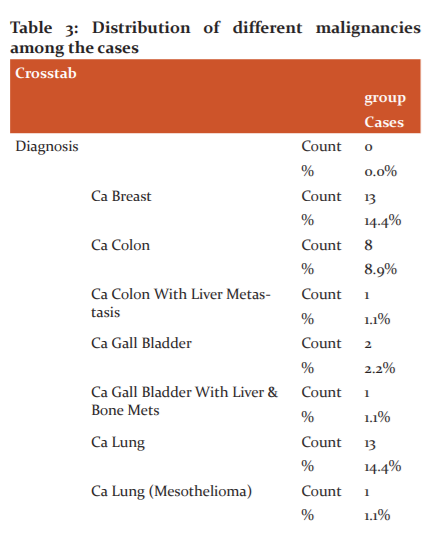
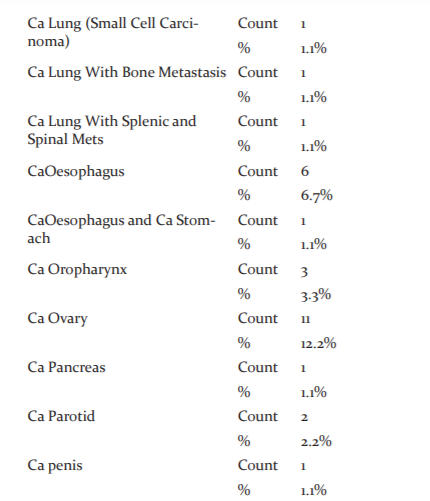
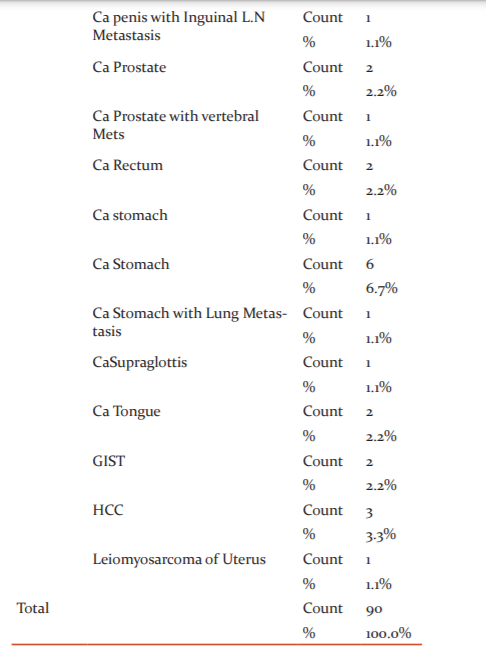
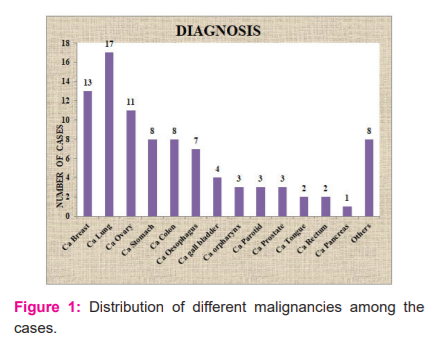
Out of 90 cases studied patients with different malignancies were taken out of which maximum number of Ca Lung (17 cases; 18.8%) patients were seen. The second most common malignancy observed was Ca breast (13 cases; 14.4%) followed by Ca ovary (11 cases; 12.2%) and Ca Colon (9 cases 10%). Few uncommon cases like Leiomyosarcoma of the uterus (1 case;1.1%) and GIST (2 cases;2.2%) were also seen (Table 3 and Figure 1).
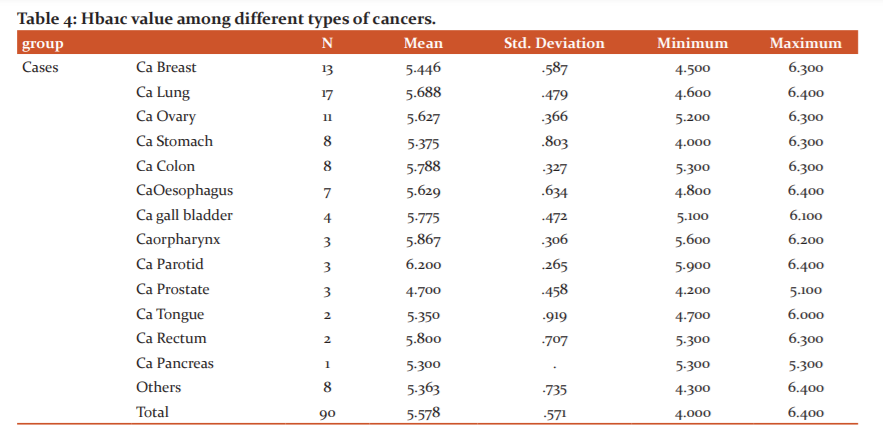
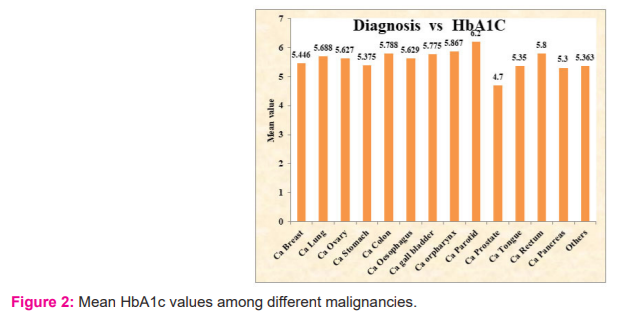
The above Table 4 represents the mean Hba1c value among different types of cancers. If we observe the table Higher Hba1c levels were found in patients with Ca Colon and Rectum, Ca Gallbladder, Ca Lung and Ca ovary. One interesting fact to be observed here is that Ca prostate patients had the lowest levels of HbA1c among the cases. In addition to that when compared with Age and Gender matched controls patients with Ca prostate had lower HbA1c levels which mean patients with Higher HbA1chadlesser chances of having Prostate malignancy (Figure 2).
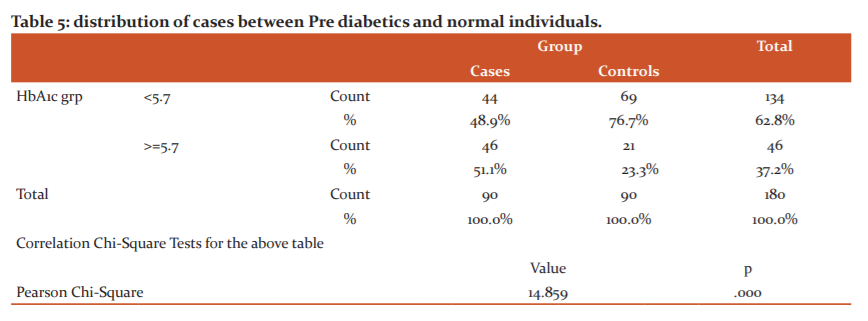
The above Table 5 shows the distribution of cases between Pre diabetics (HbA1c- <5.7) and Normal individuals (HbA1c-5.7 to 6.4). Out of 90 Cases, 46 cases (51.1%) are in the Prediabetes group whereas the remaining 44 cases (48.9%) are in the Normal group (Table 5)
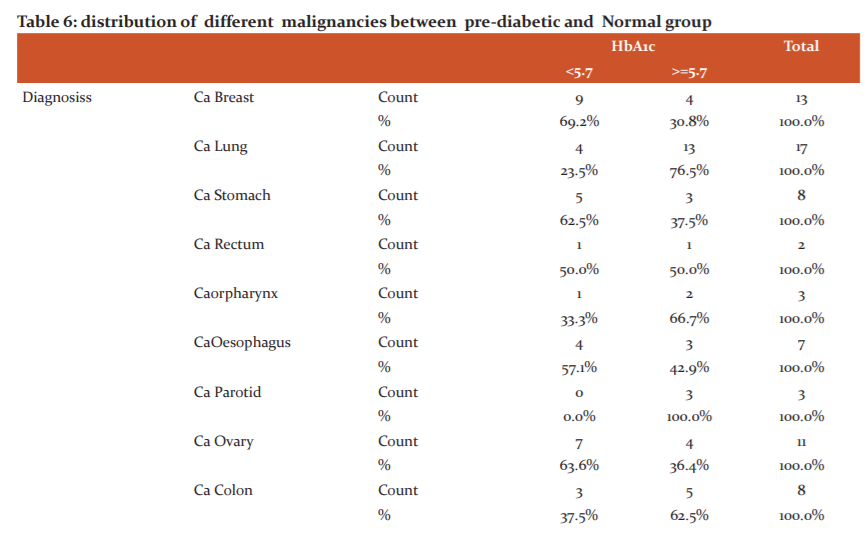
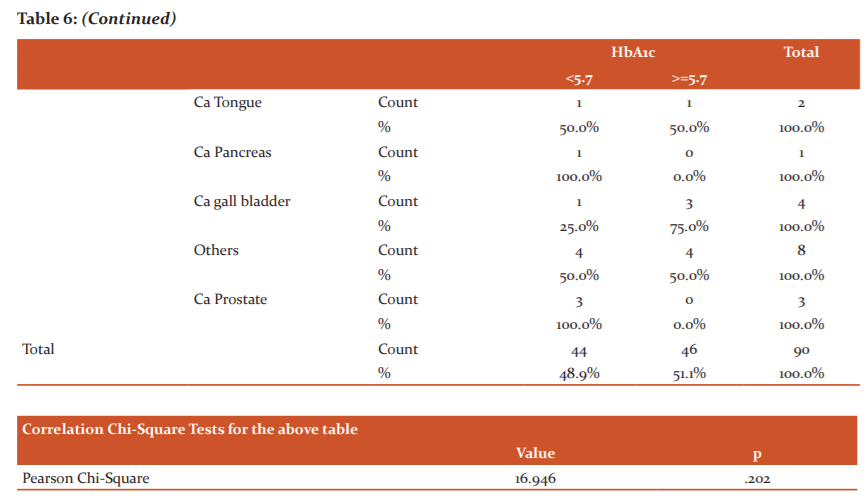
 The Table 6 represents the distribution of different malignancies between the pre-diabetic and Normal group. Out of 90 cases, 46 cases are in the Prediabetic group whereas 44 cases are in the normal group. Out of 17 cases of CaLung 13 cases (76.5%) are in the pre-diabetic group whereas 4 cases (23.5%) are in the non-diabetic group. All 3 cases (100%) of Ca Prostate are in the Non-diabetic group. Surprisingly out of 13 cases of Ca breast 9 cases (69.2%) are in the Normal group whereas 4 cases (30.8%) are in the pre diabetic group. Similarly all 3 cases (100%) of Ca parotid are in Pre diabetic group
The Table 6 represents the distribution of different malignancies between the pre-diabetic and Normal group. Out of 90 cases, 46 cases are in the Prediabetic group whereas 44 cases are in the normal group. Out of 17 cases of CaLung 13 cases (76.5%) are in the pre-diabetic group whereas 4 cases (23.5%) are in the non-diabetic group. All 3 cases (100%) of Ca Prostate are in the Non-diabetic group. Surprisingly out of 13 cases of Ca breast 9 cases (69.2%) are in the Normal group whereas 4 cases (30.8%) are in the pre diabetic group. Similarly all 3 cases (100%) of Ca parotid are in Pre diabetic group
DISCUSSION
Many studies have been done which proved the fact that diabetes and cancer both being one of the most common chronic diseases have a causal association. As we all know that persistently elevated levels of glucose for longer periods is associated with an increased risk of cancer. The explanation for the same being increase in inflammatory processes, elevated levels of insulin-like growth factor, increased metabolism of cancer cells which utilize the elevated glucose in the blood etc. Most of the studies done in this aspect always were concentrated on people having diabetes. Mathers and Loncar 2006 conducted studies on many people and established the pathophysiology underlying the development of pre-diabetes and the global burden of the disease and the associated mortality, especially in the paediatric populations and adolescents.1
Habib and Rojna 2013 conducted studies Diabetes is a high-chance state for a few sicknesses, with disease presently added to the rundown.4 With regards to the detonating diabetes rate, clarifying diabetes and tumour affiliation is a fundamental errand. Given the intricacy of equal collaboration of pathophysiological pathways hidden diabetes, the danger of tumour might be expanded by the number of immediate and roundabout systems. Encourage unthinking investigations are justified to build up organic pathways connecting the two maladies and from that point figure proficient clinical preventive methodologies and general wellbeing arrangements to abstain from covering the weight of the two sicknesses that as of now have a colossal effect on general wellbeing and economy.1
A Meta-Analysis on epidemiological examinations connecting hyperglycemia and hazard for colorectal and pancreatic malignancy the observer just surveyed chance in the most noteworthy contrasted with least classifications of exposure. A cohort study on 25,476 patients with type 2 diabetes was done in Swedish National Diabetes enrol from 1997-1999 and took after until 2009. In this investigation, there was no affiliation found between the HbA1c levels and hazard for all tumours or particular kinds of growth in patients with type 2 diabetes mellitus. In one study done by Donadon et al on Type 2 DM and HCC risk, they observed that DM2 predominance was 31.2% in patients with HCC, 23.2% in cirrhotic patients and 12.6% in controls (P < 0.0001).5 In 86% of study subjects, DM2 had been analyzed for over 1 year before the HCC conclusion. HCC patients with DM2 had a 1.5-2.5-crease expanded danger of liver growth. The HbA1c mean levels were essentially higher in DM2 patients with HCC than in cirrhotic and control DM2 patients. Antidiabetic treatment with metformin was more typical among cirrhotic and control DM2 subjects than among cases with HCC. In both arrangement of multivariate examinations, treatment with metformin altogether decreased the danger of HCC by over 80% contrasted and sulphonylureas and insulin treatment. No huge contrasts were seen between sulphonylureas and insulin treatment. Raised HbA1c levels were emphatically identified with the hazard for HCC in diabetic patients, with a 26%-half increment in the chance for each 1% expansion in HbA1c esteems.15
It is indistinct how DM2 impacts hepatocarcinogenesis. Insulin obstruction (IR) is an essential element of DM2, a confusion described by hyperglycemia related to IR and ensuing hyperinsulinemia. A few reports have proposed that the component hidden the impacts of DM2 and antidiabetic treatments on hepatic carcinogenesis could be identified with IR and hyperinsulinemia. In type-2 DM patients, insulin plasma levels are incessantly expanded by treatments because of both exogenous insulin or insulin secretagogues, for example, sulphonylureas. An overabundance of insulin plasma levels is the proposed instrument fundamental to the settled relationship of type-2 DM and obesity(the alleged diabesity) with a few sorts of strong tumours. In a past report, they found that DM2 in our populace was an autonomous hazard factor for HCC and that it goes before HCC improvement. Also, in male incessant liver sickness (CLD) patients with DM2, the danger of HCC is expanded by insulin or sulphonylurea treatment. We additionally detailed that the relationship between IR and CLD started in the beginning times of liver fibrosis and that DM2 essentially expanded IR in HCC patients. Along these lines, IR together with the resulting hyperinsulinemia appears to assume a noteworthy part in the connection amongst DM2 and hepatocarcinoma.15
Many of the studies done so far in investigating the role of HbA1c and Hyperglycemia as one of the risk factors for cancer included Diabetic patients as their cases. But very few studies were done and very limited data is available on the role of HbA1c and Hyperglycemia in Cancer association in Non-diabetic or Pre-diabetic individuals. One meta-analysis was published by J C de beer and L Liebenberg in 2014 where they analysed the risk of hyperglycemia using HbA1c in association with Solid-organ tumours in Non-diabetic individuals and they assessed the risk in different types of malignancy.1
In our study, we wanted to know whether HbA1c levels had any correlation with Malignancy and we included only Non-diabetic individuals. HbA1c a gold standard and reliable indicator of long term glucose control was used for determining the Glycemic control status of the patients.HbA1c was done by the High-performance liquid chromatography (HPLC) method. We limited our study to patients with Solid-organ tumours (Any Solid tumour) only. Patients with Blood malignancies (Leukaemias and Lymphomas) were excluded from our study. HbA1c is the most often happening part of haemoglobin A1. During the time spent glycation, glucose in the red cells reacts with N-terminal valine of both beta chains to shape an aldimine linkage which experiences revision framing more steady ketamine connect.
American Diabetes Association rules have not just considered it as the essential focus for glycemic control yet additionally included it as an analytic model. At first, it was trusted that HbA1c was just modified by glucose levels; in any case, certain examinations have noticed its height in conditions other than diabetes, for example, hemoglobinopathies, interminable kidney infections, pregnancy, and healthful anaemias.
All the patients with biopsy-proven solid organ tumours who were non-diabetics were included as cases and age and gender-matched otherwise healthy individuals were taken as controls. we enrolled a total of 180 study population of which 90 are cases (Solid-organ tumours without Diabetes) and 90 controls. The mean age among the cases is 55.45 and that of controls is 55.51 and the p-value (0.97).
Out of 90 cases studied patients with different malignancies were taken out of which maximum number of Ca Lung (17 cases; 18.8%) patients were seen. The second most common malignancy observed was Ca breast (13 cases; 14.4%) followed by Ca ovary (11 cases; 12.2%) and Ca Colon (9 cases 10%). Few uncommon cases like Leiomyosarcoma of the uterus (1 case;1.1%) and GIST (2 cases;2.2%) were also seen. The mean HbA1c among the cases was 5.578 whereas among the controls was 5.303 and the p-value is Significant (<0.001). Higher Hba1c levels were found in patients with Ca Colon and Rectum, Ca Gallbladder, Ca Lung and Ca ovary. One interesting fact to be observed here is that Ca prostate patients had the lowest levels of HbA1c among the cases. In addition to that when compared with Age and Gender matched controls patients with Ca prostate had lower HbA1c levels which mean patients with Higher HbA1c had lesser chances of having Prostate malignancy.
There is no significant difference between HbA1c levels between Males and Females (Males-5.582 vs Females-5.573) among the cases. A similar distribution of HbA1c values is observed among the controls (Males-5.449 vs Females-5.418), p-value (0.978) for cases and p-value (0.794) for controls, both being statistically non-significant meaning that HbA1c levels are not influenced much by Gender differences. The distribution of Cases among the age groups, most numbers of cases are seen between 50-60 years age(31 cases;34.4%) followed by 60-70 years (26 cases;28.9%).On the other hand, the Least number of cases are seen between 30-40 and Above 70 years of age (5 cases;5.6%).Now coming to control study population,they are equally matched with Gender and Age and represents similar numbers.Here we chose Gender matched controls with Age variation of +3 to -3.
Out of 90 Cases, 46 cases (51.1%) are in the Prediabetes group whereas the remaining 44 cases (48.9%) are in the Normal group. If we look at the distribution of different malignancies between the pre-diabetic and Normal group. Out of 90 cases, 46 cases are in the Prediabetic group whereas 44 cases are in the normal group. Out of 17 cases of Ca, Lung 13 cases (76.5%) are in the pre-diabetic group whereas 4 cases (23.5%) are in the non-diabetic group. All 3 cases (100%) of Ca Prostate are in the Non-diabetic group. Surprisingly out of 13 cases of Ca breast 9 cases (69.2%) are in the Normal group whereas 4 cases (30.8%) are in the pre diabetic group. Similarly all 3 cases (100%) of Ca parotid are in Pre diabetic group.
CONCLUSION
In our study, it is observed that higher HbA1c levels are associated with an increased risk of cancer independent of diabetes. The risk is higher with Lung cancer, Colo-rectal cancers, Ovarian tumours and Gall bladder tumours. On the contrary patients with prostate cancer had lower HbA1c levels.
LIMITATIONS
Several limitations should be kept in mind.
-
The study population is very small
-
It is a cross-sectional study
-
Many confounding factors like prior usage of steroids and other hyperglycemic drugs can’t be ruled out
-
Other confounding factors like Diet, Alcohol, smoking, occupation etc. were not ruled out
-
Controls who were in the pre-malignant stage, or in early stages of malignancy can be missed
IMPLICATIONS OF THE STUDY
The close direct relationship of HbA1c levels with the danger of a few malignancies bolsters the guess that it may be conceivable to utilize HbA1c as an autonomous metabolic biomarker for malignancy hazard in diabetic or non-diabetic people. Essentially, the examination likewise gives fundamental proof to an effectively expanded malignancy chance in the Normal and pre-diabetic classes for various Malignancies. The occurrence of disease in the diabetic and non-diabetic populaces could, along these lines, conceivably be lessened by diminishing glucose levels. This could be accomplished by methods for the proper way of life or remedial intercessions, and by forcing stricter proposals for glycaemic control. The dangers and focal points of refreshing suggestions for stricter glycaemic control justify critical examination. Signs are that much stricter glycaemic control measures could help decrease the hazard for growth occurrence and mortality in so far as care is taken to guarantee that stricter glycaemic control does not result in hypoglycaemia, which may have different pernicious impacts.
Acknowledgement: I thank Dr Chakrapani to guide me throughout the study.
Conflict of Interest: Nil
Source of Funding: Nil
References:
- Beer JC, Liebenberg L. Does cancer risk increase with HbA1c independent of diabetes. Br J Cancer 2014;110:2361-2368.
- Coussens L, Zitvogel L, Palucka A. Neutralizing Tumor-Promoting Chronic Inflammation: A Magic Bullet. Science 2013;339(6117):286-291.
- Giovannucci E, Harlan D, Archer M, Bergenstal R, Gapstur S, Habel L et al. Diabetes and Cancer: A consensus report. Science 2018;32:256-259.
- Habib S, Rojna M. Diabetes and Risk of Cancer. Int J Oncol 2013;2013:1-16.
- Donadon V, Balbi M, Casarin P, Vario A, Alberti A. Association between hepatocellular carcinoma and type 2 diabetes mellitus in Italy: potential role of insulin. World J Gastroenterol 2008;14(37):5695-700.
- Centres for Disease Control and Prevention (CDC) Prevalence of overweight and obesity among adults with diagnosed diabetes the United States, 1988–1994 and 1999–2002. Morb Mort Weekly Rep 2004;53(45):1066–1068.
- Calle EE, Thun MJ. Obesity and cancer. Oncogene 2004;23(38):6365–6378.
- Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Can 2004;4(8):579–591.
- Kulie T, Slattengren A, Redmer J, Counts H, Eglash A, Schrager S. Obesity and women’s health: an evidence-based review. J Am Board Fam Med 2011;24(1):75–85.
- Eliassen AH, Colditz GA, Rosner B, Willett WC, Hankinson SE. Adult weight change and risk of postmenopausal breast cancer. J Ame Med Assoc 2006;296(2):193–201.
- La Vecchia C, Giordano SH, Hortobagyi GN, Chabner B. Overweight, obesity, diabetes, and risk of breast cancer: interlocking pieces of the puzzle. Oncologist 2011;16(6):726–729.
- Leroith D, Novosyadlyy R, Gallagher EJ, Obesity and Type 2 diabetes are associated with an increased risk of developing cancer and a worse prognosis; epidemiological and mechanistic evidence. Exp Clin Endocrinol Diab 2008;116(supplement 1):S4–S6.
- Ma J, Li H, Giovannucci E, Prediagnostic body-mass index, plasma C-peptide concentration, and prostate cancer-specific mortality in men with prostate cancer: a long-term survival analysis. Lancet Oncol 2008;9(11):1039–1047.
- Schienkiewitz A, Schulze MB, Hoffmann K, Kroke A, Boeing H. Body mass index history and risk of type 2 diabetes: results from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam Study. Am J Clin Nutr 2006;84(2):427–433.
- Abdul-Ghani MA, Sabbah M, Muati B, et al. High frequency of pre-diabetes, undiagnosed diabetes and metabolic syndrome among overweight Arabs in Israel. Isr Med Assoc J 2005;7(3):143–147.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





