IJCRR - 13(10), May, 2021
Pages: 89-94
Date of Publication: 19-May-2021
Print Article
Download XML Download PDF
To Study the Correlation of CRP Levels with Functional Ability in Chronic Obstructive Pulmonary Disease Patients in Tertiary Health Care in Western UP
Author: Singh Yogita, Mittal Santosh, Singh Dhirendra Pratap
Category: Healthcare
Abstract:Introduction: Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases. The chronic airflow limitation that is characteristic of COPD is caused by a mixture of small airways disease (e.g. Obstructive bronchiolitis) and parenchymal destruction (emphysema), the relative contributions of which vary from person to person. 1 Objective: The present study aims to investigate whether an increased concentration of high sensitivity (hs) CRP is related to the degree of lung function impairment, systemic inflammation, body composition, exercise capacity, and quality of life in patients with advanced COPD. Methods: A cross-sectional study was conducted in the Department of Medicine of LLRM Medical College and Associated SVBP Hospital Meerut in 2019-2020. Sixty-one Patients with Chronic Obstructive Pulmonary Disease of age 35 years and above undergoing treatment Meerut were included in this study. Each subject has undergone a thorough workup for history and physical examination to fulfil the inclusion & exclusion criteria, Routine Hematological & Biochemical Investigations were carried out. Results: Mean age of the patients was 56.16 years. Most of the patients were in the age group 56-65 (44.26%). The majority fell in the range of 36-65 years (85.24%). The majority of the patients were males (77.05%). Females were few 14 (22.95%). The hsCRP levels correlated negatively with FEV1 (p-0.000) and 6-minute walking distance (p-0.000). Correlation between hsCRP levels and BMI was also negative though not significant (p-0.32). BODE index and hsCRP levels had a highly significant positive correlation (p-0.000). Conclusion: High sensitivity C-reactive protein levels correlated significantly with functional ability parameters in chronic obstructive pulmonary disease patients. There was a significant correlation with forced expiratory volume in 1 second, exercise capacity assessed by six-minute walking distance test and, Body-mass index, airflow Obstruction, Dyspnea, and Exercise( BODE index). However, the levels did not correlate significantly with body mass index.
Keywords: Chronic Obstructive Pulmonary Disease (COPD), CRP, BODE INDEX, BMI, hsCRP, Forced expiratory volume in 1 second (FEV1).
Full Text:
INTRODUCTION
COPD represents a disease state characterized by poorly reversible airflow limitation that is usually both progressive and associated with an abnormal inflammatory response of the lung. Among the leading causes of death and disability, COPD is the one that is rising most rapidly. COPD is currently the sixth-leading cause of death and the 12th leading cause of morbidity worldwide.2 By the year 2020 COPD is expected to be the third leading cause of death and the fifth leading cause of disability. The World Bank estimates that COPD is responsible for more than 29 million disability-adjusted life years (DALY) and 1 million years of life lost per annum.
Cigarette smoking is the most important risk factor leading to the development of COPD. Smoking accounts for nearly 90% of cases of COPD. Yet, for unknown reasons, only 20% of Cigarette smokers develop COPD. COPD is the major cause of mortality and morbidity in India. In most non-tubercular chest clinics in India, COPD constitutes 25-30 % of the cases. In various studies by Jindal et al and Malik et al. on different populations in north India, its prevalence varied from 1% in urban nonsmokers to 21% in rural smokers.3-6 Disease is equally prevalent in rural and urban India. Males are more affected than females. Traditionally COPD has been viewed as an inflammatory disease of the lungs but several studies have shown that this pulmonary inflammation may also be detected in the systemic circulation. This has been shown by increased circulating concentrations of interleukin-6 and acute phase reactants such as CRP in COPD patients.
As reviewed by Can et al. several systemic inflammatory mediators, like tumour necrosis factor-alpha (TNF), ILs, APPs, CRP, LBP and leukocytes are increased in COPD. CRP increases in systemic inflammation as compared to healthy controls. The Higher Level of CRP in COPD has been scrutinized in the Third National Health and Nutrition Examination Survey.7 Which showed that 41% of patients with moderate COPD (FEV1> 50- 80%pred) had a CRP above 3 mg/l and 6% above 10 mg/l. while as much as 52% of patients with severe COPD (FEV1<50%pred) had CRP above 3 mg/l and 23% above 10 mg/l
Nutritional depletion and weight loss are features of COPD. As many as 25% of COPD patients attending outpatient services may be malnourished, while almost 50% of patients with COPD admitted to the hospital have evidence of malnutrition. This figure increases to 70% in patients with COPD with acute respiratory failure.
The present study aims to investigate whether an increased concentration of high sensitivity (hs) CRP is related to the degree of lung function impairment, systemic inflammation, body composition, exercise capacity, and quality of life in patients with advanced COPD.
MATERIALS AND METHODS
This study was conducted in the Department of Medicine of LLRM Medical College and Associated SVBP Hospital Meerut in 2019-2020. Patients with Chronic Obstructive Pulmonary Disease of age 35 years and above undergoing treatment at the Medicine outpatient department of the LLRM Medical College and Associated SVBP Hospital, Meerut were included in the study. The number of patients included in the study was sixty-one. The study conducted was a cross-sectional study. Informed consent was taken from all the patients. Ethical clearance was obtained to conduct this study (No./SC-1/2021/656).
These patients were subjected to complete history taking and physical examination. Particulars of the patients such as name, age, sex, pack-years of smoking etc. were noted in a Performa. The patients of the study group were examined and various required investigations were done. A required regime of inhaled and oral bronchodilators, as well as inhaled steroids, were given during the study. Systemic steroids were not used.
Procedure
Every Patient was interviewed and proper detailed history was taken regarding chronic obstructive pulmonary disease and as well as the duration of disease and personal history including smoking and alcohol consumption. Each subject has undergone a thorough workup for history and physical examination to fulfil the inclusion & exclusion criteria, Routine Hematological & Biochemical Investigations were carried out. All patients had Chestx-ray-PA view &ECG. The following parameters were measured at the time of enrollment into the study:
-
Spirometry
-
BMI
-
Six-minute walking distance test
-
Bode Index
-
CRP Levels
Inclusion criteria
-
Patients having COPD with advanced disease (forced expiratory volume in 1 second (FEV1)< 70% predicted)
-
Patients having no exacerbation of COPD for at least 2 months.
-
Patients having an age of more than 35 years.
Exclusion criteria
-
Infections (ruled out by history and examination)
-
Myocardial infarction within the past 6 months
-
Angina
-
Congestive heart failure
-
Ventilator dependency
-
Malignancy
-
Cirrhosis
-
End-stage renal disease
-
Rheumatoid arthritis
-
Orthopaedic condition precluding performance of walking or cardiopulmonary exercise tests
Investigations done in all cases:
RESULTS
The study was conducted at the Department of Medicine at LLRM Medical College &SVBP Hospital, Meerut U.P. in 2019-2020. Patients with Chronic Obstructive Pulmonary Disease of age 35 years and above undergoing treatment at the Medicine outpatient department of the SVBP Hospital were included in the study. The number of patients included in the study was sixty-one. These patients were subjected to complete history taking and physical examination. Particulars of the patients such as name, age, sex, pack-years of smoking etc. were noted in a Performa. The following parameters were measured at the time of enrollment into the study:
-
Spirometry
-
Body mass index
-
6- min walking distance test
-
BODE index
-
CRP levels by hsCRP ELISA method.
Demographic characteristics
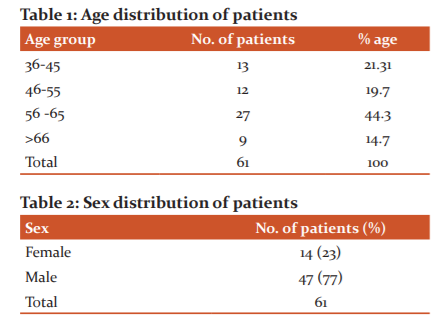
The age distribution is shown in Table 1. The minimum age was 36 years and the maximum was 81 years. The mean age of the patients was 56.16 years. Most of the patients were in the age group 56-65 (44.26%). Sex distribution is as shown in Table 2. Majority of the patients were males (77). Females were 14 (23). More than 50% of patients had BMI >21 kg / m2 at the enrollment into the study.

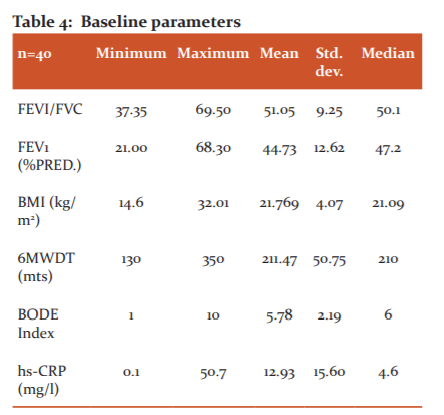
All the patients had FEVI/FVC ratio <70%. The mean was 51.05 and the median was 50.1. The mean FEV1 of the patients was 44.73±12.62 with a range from 21 to 68.3. The mean distance walked in 6 minutes was 211.47±50.75 with a range from 130 to 350 m. BODE index mean was 5.78±2.19 with a range from 1 to 10 and median was 6. Values of hsCRP were highly variable with a mean of 12.93±15.60 and range from 0 to 50.7 (Table 4).
The hsCRP levels were correlated with baseline functional ability parameters of patients using Pearson correlation. The hsCRP levels correlated negatively with FEV1 and correlation was highly significant (p<0.001). Correlation between hsCRP levels and BMI was also negative though not significant (p<0.37). 6-minute walking distance was also negatively correlating with hsCRP levels with a significant p value= 0.005. BODE index and hsCRP levels had a highly significant positive correlation with a p-value <0.0001.

DISCUSSION
The study was conducted at the Department of Medicine at LLRM Medical College &SVBP Hospital, Meerut U.P. in 2019-2020. Patients with Chronic Obstructive Pulmonary Disease age 35 years and above undergoing treatment at the Medicine outpatient department of the SVBP Hospital were included in the study. The number of patients included in the study was 61. The study conducted was a cross-sectional study. Informed consent was taken from all the patients.
These patients were subjected to complete history taking and physical examination. Particulars of the patients such as name, age, sex, pack-years of smoking etc. were noted in a Performa.Age distribution of COPD patients. The mean age of patients in the study was 56.16+10.44 years. The maximum number of patients was in the 36-65 years of age group (85.24%). Studies that were done on COPD patients in the west shows a higher mean age of patients. A study by Pauwels on COPD patients in Europe showed that approximately half of the patients were in the 60-69 age group.8 DA Redelmeier et al. in their study had a mean age of 67 years in stable COPD patients.9 Another study by Pride et al showed that the majority of COPD patients were more than 65 years of age in the United Kingdom.10
These results show that the mean age of the COPD patients in our study was less than the mean age of COPD patients in western literature. This may be explained based on the genetic makeup of the Indian population, environmental factors, poor living conditions or smoking habits. However, the exact cause is still unknown.
Sex distribution of COPD patients
The majority of the patients in the study were males (77%). The ratio of male to female was 3.35:1. As studied by Jindal et al, the majority of the patients with COPD are male in India.11 This may be due to the smoking habit being more common in males. Recent epidemiological data have shown that there is an increasing trend in the prevalence of COPD in females.
BMI of patients
In this study, 50.8% of patients had BMI>21 kg/m2and 49.2% had BMI < 21 kg/m2. The results from the Honolulu Heart Program had indicated that in elderly Japanese-American men, age-adjusted mortality was highest in those with both BMI < 21 kg/m2 and FEV1 predicted < 70%.12 Chailleuxetal found that lower body mass index (BMI) was an independent negative determinant of survival in patients with COPD.13
In another study by Landboetalon subjects from the Copenhagen City Heart Study, it was concluded that low BMI is an independent risk factor for mortality in subjects with COPD and that the association is strongest in subjects with severe COPD. Gray-Donald et al. reported that in patients with severe COPD, low body weight, a potentially modifiable factor, was associated with respiratory mortality.
In our study, BMI had a negative correlation with hsCRP levels though the correlation was not significant (p<0.37). Previously, Schools et al have also found a similar negative correlation. However, in a study by de Torres et al., A positive though non-significant correlation was found between BMI and hsCRP levels. C-reactive protein being the marker of systemic inflammation causes a significant decrease in weight and therefore BMI. However, further prospective studies are required to demonstrate the exact correlation.14
Forced expiratory volume in 1 second (FEV1)
The FEV1 is essential for the diagnosis and quantification of the respiratory impairment resulting from COPD. In addition, the rate of decline in FEV1 is a good marker of disease progression and mortality. In our study, the majority of the patients had moderate to severe airway obstruction (83.6%). The baseline FEV1 correlated negatively with hsCRP levels significantly (p<0.001). The prevalence of increased CRP in COPD has been examined in the Third National Health and Nutrition Examination Survey (NHANES III), which showed that there is a significant negative correlation between CRP levels and FEV1.7, 15
COPD patients, with slightly elevated CRP levels, have not yet been characterized nor have there been studies to explore a potential role of CRP as a marker for local or systemic impairments. Although a smaller study did not find a correlation between CRP and lung function in patients with mild to severe COPD. CRP seems to increase with the increasing severity of COPD. In this study, a more impaired postbronchodilator FEV1 and reversibility were also found in patients with elevated systemic CRP. Higher the airway inflammation in COPD patients, lower the reversibility suggestions recommend multiple inflammations driven airflow restrictions. Therefore there should be more future studies explored for the same.
6-Min Walking Dsistance
This is a test of functional exercise capacity, measured by the distance covered (in feet) during 6-min walking with standardized encouragement. The 6-min walking distance test is frequently used to assess functional capacity in chronic disorders because of its simplicity. 6MWD Test was very useful in treating the disability and of course risk attached to it in other chronic diseases including congestive heart failure and pulmonary hypertension.
Indeed, the distance walked in six minutes has been accepted as a good outcome measure after interventions such as pulmonary rehabilitation. D.ARedelmeier studied individuals with stable COPD (n = 112) and estimated the smallest difference in 6MW distances that was associated with a noticeable difference in patients' subjective comparison ratings of their walking ability16. They found that the 6MW was significantly corrected with patients' ratings of their walking ability relative to other patients (r = 0.59, 95% confidence interval [CI]: 0.54 to 0.63). They also suggested that differences in functional status can be statistically significant but below the threshold at which patients notice Ma difference in themselves relative to others; an awareness of the smallest difference in walking distance that is noticeable to patients may help clinicians interpret the effectiveness of symptomatic treatments for COPD.
The mean 6-minute walking distance in our study was 211.48 meters and the correlation between hsCRP levels and 6MWD was negative and highly significant (p<0.005). It has also been observed previously that CRP levels inversely correlated with 6MWD. Koechlin et al found that CRP levels inversely correlated with endurance time17. Broekhuizen et al also found that CRP increases in patients with poor exercise capacity. On the other hand others propose that "myopathy" is an independent process that contributes to the systemic inflammatory load of the disease.
Body index
The BODE index is a simple grading system for COPD, devised by Celliet al and they validated its use by showing that it is a better predictor of the risk of death from any cause and from respiratory causes than is the FEV1 alone. The BODE index is useful because it includes one domain that quantifies the degree of pulmonary impairment (FEV1), one that captures the patient's perception of symptoms (the Modified Medical Research Council dyspnea scale), and two independent domains (the distance walked in six minutes and the body-mass index) that express the systemic consequences of COPD.
More importantly, prospective observational studies of patients with COPD have found that the degree of dyspnea and health-status scores are more accurate predictors of the risk of death than is the FEV1. Thus, although the FEV1 is important to obtain and essential in the staging of disease in any patient with COPD, other variables provide useful information that can improve the comprehensibility of the evaluation of patients with COPD. Each variable should correlate independently with the prognosis of COPD, should be easily measurable, and should serve as a surrogate for other potentially important variables. In the BODE index, there are two descriptors of systemic involvement in COPD: the body-mass index and the distance walked in six minutes. Both are simply obtained and independently predict the risk of death.
The Global Initiative for Chronic Obstructive Lung Disease and the American Thoracic Society recommend, that a patient's perception of dyspnea be included in any new staging system for COPD. Dyspnea represents the most disabling symptom of COPD; the degree of dyspnea provides information regarding the patient's perception of illness and can be measured. The Modified Medical Research Council dyspnea scale is simple to administer. The BODE index combines the four variables using a simple scale.
Values of the BODE index vary from 0 to 10. In our study, the mean was 5.79+2.192 and it correlated positively with hs CRP levels significantly (p<0.001). Hence BODE index is a better predictor of COPD severity as compare to FEV1 and also it is easy to calculate too. Although the BODE index is a predictor of the risk of death, we do not know whether it will be a useful indicator of the outcome in clinical trials, the degree of utilization of health care resources, or the clinical response to therapy.
High Sensitivity C-Reactive Protein
The hsCRP is the systemic inflammatory marker that has extensively been studied in cardiovascular disorders. Recently it is being used as a marker in COPD and as an etiological factor of systemic effects of COPD. In our study, the values of hsCRP were highly variable and ranged from 0.1 to 50.7 mg/1. The mean value of hsCRP was 12.93 mg/1 which in itself is significant as compared to the previous studies. The Higher Level of CRP in COPD has been scrutinized in the Third National Health and Nutrition Examination Survey, which showed that 41% of patients with moderate COPD (FEV1> 50- 80%) had a CRP above 3 mg/1 and 6% above 10 mg/1, while as much as 52% of. Patients with severe COPD (FEV1<50%pred) had CRP above 3 mg/1 and 23% above 10 mg/1.This survey showed that there are higher levels of CRP with increasing severity of COPD.
In our study also, there is a significant negative correlation with FEV1 (p<0.001). The hsCRP levels had already been correlated with various functional ability parameters in different studies but the results are still not well defined. In a study by Broekhuizenetal, they analyzed 102 patients with COPD admitted to an inpatient pulmonary rehabilitation centre; most patients had severe to very severe COPD and nearly one third were on systemic corticosteroids They showed that raised CRP levels were associated not only with diminished muscle strength but also with reduced exercise endurance, workload, 6-minute walk distance, and poor health status and quality of life, all of which are important clinical endpoints.
The study by Pinto-Plata and colleagues takes these findings one step further19. In this study, they have seen that CRP levels were inversely related to the distance covered in the 6-minute walk test independent of many other factors like sex, smoking, age. In this study, 60% of COPD Patients had inhaled corticosteroids at the time of examination but still, CRP levels were on average about 40% lower than of corticosteroid non-user.
In our study, hsCRP levels correlated negatively with FEV1, BMI and 6MWDT and all the correlations were significant except BMI. The hsCRP levels correlated positively with the BODE index, the valuable tool of functional ability. CRP seems to be a marker for impairments in exercise capacity and distress due to respiratory symptoms as shown in this study, routine hsCRP analysis could prove itself to be of major clinical importance in COPD. CRP can be used routinely in clinical practice to risk-stratify COPD patients. In those who have elevated levels, physicians should consider aggressive therapies (e.g. smoking cessation programs and other lifestyle interventions and possibly some pharmacologic agents) to reduce the risk of morbidity and mortality in such patients. Further research is needed to assess the value of CRP as a biomarker for measuring the progress of the disease and for the effects of treatment of COPD. Limitations of the study
-
The sample size was small therefore statistical power of the study was low.
-
Patients were on standard treatment of chronic obstructive pulmonary disease so many were receiving inhaled steroids and their effect on hsCRP levels is not well established.
CONCLUSIONS AND RECOMMENDATIONS
The chronic obstructive disease occurs at a younger age in the Indian population as compared to the west. High sensitivity C-reactive protein levels correlated significantly with functional ability parameters in chronic obstructive pulmonary disease patients. There was a significant correlation with forced expiratory volume in 1 second, exercise capacity assessed by six-minute walking distance test and BODE index. However, the levels did not correlate significantly with body mass index. Large scale longitudinal prospective studies are required to further elaborate the results.
Acknowledgement- Dr Mittal Santosh- Statistical analysis, Dr Singh Dhirendra Pratap - Technical assistance.
Source of Support: None
Conflict of Interest: None
Contribution of each author: Dr Singh Yogita and Dr Mittal Santosh – Compilation of data, review of the literature and writing the final draft of the manuscript, Dr Singh Dhirendra Pratap- Data analysis and outcome assessment. All authors equally contributed to the data analysis and drafting of the manuscript.
References:
-
Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis management and prevention of Chronic Obstructive Pulmonary disease. Updated 2017. Global Initiative for Chronic Obstructive Lung Disease, 2019
-
World Health Organization. World health statistics 2008. Geneva: BMJ Publishing Group, 2008.
-
Jindal SK. A field study on follow up at 10 years of the prevalence of COPD and PEFR. Ind J Med Res B 1993;98:20-6.
-
Malik SK. Profile of chronic bronchitis in North India- The PGI experience (1972-1985). Lung India 1986;4:89.
-
Jindal SK, Malik SK. Tobacco smoking and non-neoplastic respiratory disease(Proceedings of the UICC workshop "Tobacco or health".) In: Tobacco, and health: the Indian scene. Sanghavi LD, Notani P, eds. Tata Memorial. Centre, Bombay: 1983;p30.
-
Malik SK, Bchcra D, Jindal SK. Reverse smoking and COPD. Br J Dis Chest 1983;77:199.
-
Mannino DM, Gagnon RC, Petty TL, Lydick E. Obstructive lung disease and low lung function in adults in the United States: data from the National Health andNutrition Examination Survey, 1988-1994. Arch Intern Med 2000;160:1683-89.
-
Romain Pauwels. COPD: The Scope of the Problem in Europe. Chest 2000;117:332-5
-
Redelmeier DA, Bayoumi AM, Goldstein RS. Interpreting small differences in functional status: the six-minute walk test in chronic lung disease patients. Am J Respir Grit Care Med 1997;155:1278-82.
-
Pride NB, Soriano JB. Chronic obstructive pulmonary disease in the United Kingdom: trends in mortality, morbidity and smoking. Curr Opin Pulmon Med 2002;8:95-101.
-
Goris AHC, Schols AM, Weling-Sheeoers CAP. Tissue depletion about physical function and quality of life in patients with severe COPD. Am J Respir Crit Care Med 1997;155:A498.
-
Chailleux E, Fauroux B, Binet F. Predictors of survival in patients receiving domiciliary oxygen therapy or mechanical ventilation: a 10-year analysis of ANTADIR Observatory. Chest 1996;109:741-9.
-
de Torres JP, Cordoba-Lanus E, Lopez-Aguilar C. C-reactive protein levels and clinically important predictive outcomes in stable COPD patients. Eur Respir J 2006; 27:902-7.
-
Mannino DM, Ford ES, Redd SC. Obstructive and restrictive lung disease and markers of inflammation: data from the Third National Health and Nutrition Examination. Am J Med 2003;114(9):758-62.
-
Koechlin C, Couillard A, Cristol JP. Does systemic inflammation trigger local exercise-induced oxidative stress in COPD? Eur Respir J 2004;23(4):538-44.
-
Broekhuizen R, WoutersEF, Creutzberg EC. Raised CRP levels mark metabolic and functional impairment in advanced COPD. Thorax 2006;61:17-22.
BPinto-Plata VM, Mullerova H, Toso JF. C-reactive protein in patients with COPD, control smokers, and non-smokers. Thorax 2006;61:23-8.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





