IJCRR - 7(24), December, 2015
Pages: 30-38
Date of Publication: 20-Dec-2015
Print Article
Download XML Download PDF
OCCUPATIONAL HAZARDS AMONG PRACTICING DENTISTS IN CHENNAI- A SURVEY REPORT
Author: Kalpana Gokul, Abirami, BalaSundaram
Category: Healthcare
Abstract:Aims: This paper reports the survey results of the prevalence of occupational hazards among the practicing dentists in Chennai.
Settings and Design: A Descriptive Epidemiological study.
Methods and Material: A survey was conducted by using a self-administered questionnaire from two hundred and fifty practicing dental surgeons. Only practicing dentists were included in the study and non practitioners were excluded.
Statistical analysis used: The statistical analyses were performed with use of SPSS version 20.0 package. Results were considered significant for \"p\" values of ?0.05.
Results: Among all the occupational hazards experienced, lower back pain was the highest (57%), followed by neck pain (52.8%), head ache (38.4%) and frequent respiratory illness (22.4%). Among the preventive measures practiced, least employed were regular physical exercises (40.8%), engaging in sports activity (20%) and use of simple or compound loupes (20.4%). Among all the infection control protocols, least followed one was wearing protective eye goggles (67.6%).
Conclusions: There was high level of awareness of exposure to occupational hazards among the dental surgeons. However, the practical steps to prevent them were not followed and hence, needs to be reinforced. Lower back pain was the highest hazard experienced. Increased awareness must be created about complications of musculoskeletal deformities. Its prevention by regular physical exercise should be emphasized and the importance of regular monitoring of muscle health through EMG analysis could give an early insight into the muscle fatigue leading to musculoskeletal deformities.
Keywords: Occupational hazards, Dentistry, Musculoskeletal deformities
Full Text:
INTRODUCTION
Although dentistry is among the least hazardous of all the professions, many risks remain in dental practice which continues to challenge this status. These include per cutaneous exposure incidents; exposure to infectious diseases by bio aerosols; exposure to radiation, noise and dental materials; musculoskeletal disorders ; dermatitis ; eye injuries; vibration induced neuropathy and psychological problems.[1] BernadinoRamazzini, is referred to as the father of occupational medicine, recognized the role of occupation in the dynamics of health and diseases. [2] The practice of dentistry exposes dental professionals to a variety of work-related hazards. These include:
• Working long hours at a high level of concentration
• Working in a sedentary state
• Working with anxious patients
• Exposure to microbial aerosols
• Exposure to various chemicals used in clinical dental practice
The source of these hazards is the work environment which can include physical, chemical, biological aspects. [2]
Physical Hazards:
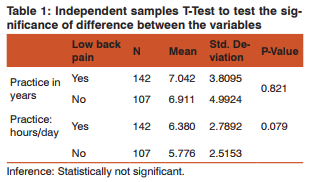
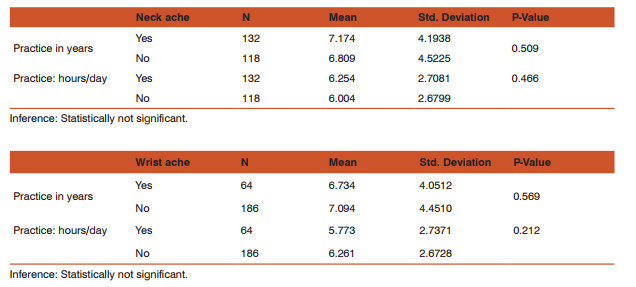
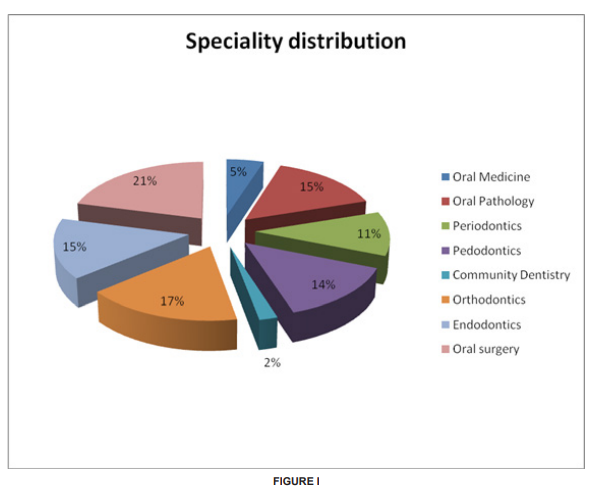
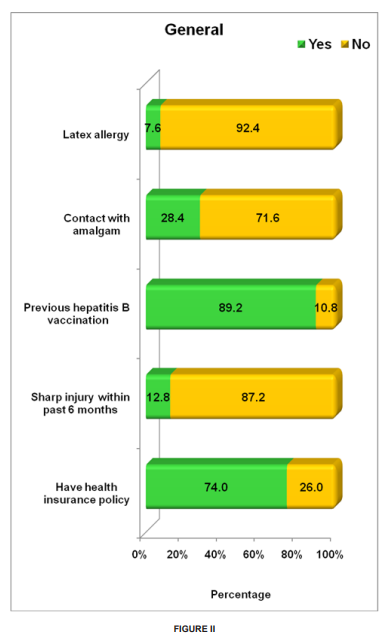
The sources of physical injury can include debris from the oral cavity striking the eyes, cuts from sharp instruments, or puncture wounds from needles or other sharp instruments. Such injuries can result in the transmission of serious infec tious disease to the clinician. Needle stick injuries and cuts from sharp objects and instruments (percutaneous injuries) have been reported during surgical procedures mostly associated with suturing. [3] Eye injuries may occur from projectiles such as bits of calculus during scaling procedures and splatters from body fluids (bacterial and viral aerosols) while using high-speed hand pieces. Another potential source of eye injury is the intense dental curing light. Users of dental curing lights should be advised to employ protective eye- wear during use. [4][5] The need to work in a fixed working position using a continuous repetitive motion can predispose the clinician to wrist ache, lower backache, and neck ache.[6] The most common injuries reportedly experienced by the dentists are musculoskeletal in nature.[7] Chemical Hazards: Many biomaterials and auxiliary products used in dentistry are chemically reactive. [8] Hazardous chemical agents used in clinical dentistry include mercury, powdered natural rubber latex, disinfectants, and nitrous oxide. By far the most important and most dangerous of these agents is mercury.[9] Its use in dental amalgam has the potential for continuous occupational exposure of a dental practitioner to mercurial vapour which can be absorbed via the skin and the lungs.[10] The active component in the mercurial vapour has a particular affinity for brain tissue. Mercury poisoning can be characterized by tumors of the face, arms, or legs and can also be associated with progressive, tremulous illegible handwriting and slurred speech. The exposure risks for mercury can be minimized by careful handling procedures. The continued use of powdered NRL gloves and disinfectants has predisposed clinician to hand dermatitis, contact dermatitis, contact urticaria, and allergic dermatitis.[11] The most serious potential hazard associated with the continued use of powdered NRL gloves in dental practice is latex sensitization caused by exposure to aerosolized NRL protein. This can result in dermatitis on the hands. This occurs with such frequency that it is now recognized as an occupational hazard in dentistry, and many dental offices have had to stop using latex materials such as gloves and rubber dams. [12] In recent studies, the frequency of occupational related dermatitis varied from 21% to 43% depending on the prevailing material used in the various specialties. [13] Transient irritative reactions of the eyes and air- ways have been observed mostly associated with exposure to volatiles from resin based materials, x-ray chemicals, and cleansers. These include procaine, soaps, eugenol, iodine, formalin, phenol, and other disinfectants. [8] Retrospective surveys of dental and medical personnel have linked occupational exposure to nitrous oxide with a number of health problems and reproductive derangements.[14][15] Thus, adequate pollution control mechanisms in accordance with the Federation DentaireInternationale (FDI) should be adopted.[14][15] Biological (Cross-Infection) Hazards: Dentistry is unique in that clinician is in direct contact with traumatized tissues, saliva, and blood on a daily basis. [16] There is high risk of exposure to Hepatitis B virus (HBV), HIV infection, and other types of communicable infections. [16] A study reported that the carrier rate HBV in the general population is 0.5%, while dentists have a carrier rate of approximately 1.6%. Several of the common viral agents that can cause hepatitis have been detected in body fluids including saliva and blood. The viruses most commonly implicated include hepatitis A virus (HAV), HBV, and hepatitis C. [17][18] This study was aimed at assessing the level of awareness of occupational hazards among practicing dentists in Chennai. This was done by identifying hazards and estimating their prevalence rate. Materials and Methods: The study population consisted of two hundred and fifty practicing dentists at Chennai. Data was obtained through the use of questionnaires that included questions on, awareness to occupational hazards, safety measures practiced, and experience of occupational hazard experienced in Dental practice. The questionnaire was pilot tested in a sample size of twenty subjects for validity and repeatability. Data was analyzed using frequency tables to display the responses. Where necessary, cross tabulations were carried out to determine the significant difference between variables. Chi-square test and independent sample T test was used to test the significance of difference between different variables. Results: A total of two hundred and fifty dental practitioners participated in the study (Figure-I). The mean number of practice in years among the dental practitioners was seven years. The number of practice hours per day range from one to thirteen hrs among the practitioners. Majority (57.2%) practiced around six days in a week. Table-I describes that based on the number of years in practice or number of practice hrs per day, there was no statistically significant difference in the presence of lower back pain, wrist pain or neck pain among the dentists. Figure-I show distributions of the post graduate practitioners. Figure-II shows majority (89.2%) have had previous hepatitis B vaccination and around 74% have taken insurance policy. 28.4% reported contact with amalgam, 12.8% reported sharp injury in the past six months and only 7.6% reported latex allergy.
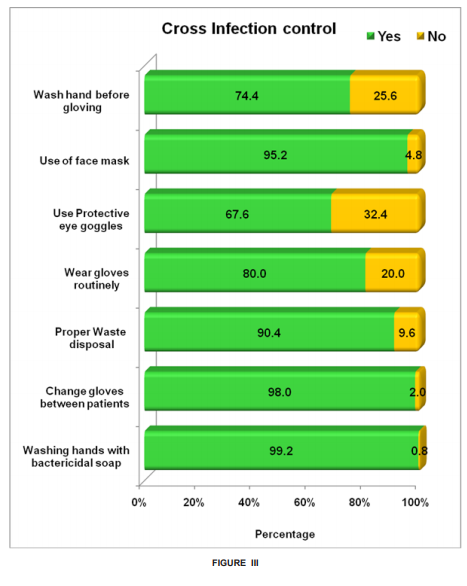
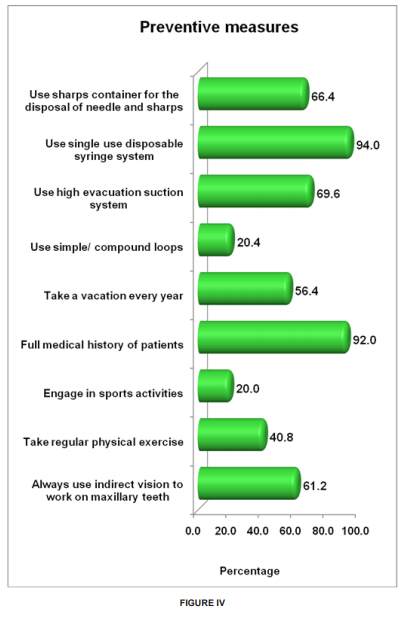
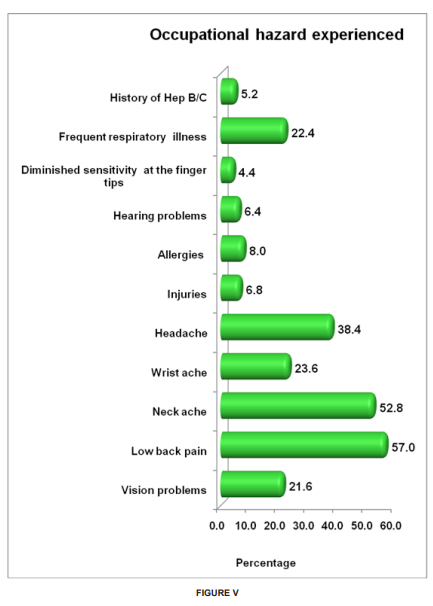
Figure-III shows the practice of cross infection control among practitioners. Among the cross infection control mechanisms employed, wearing protective eye glasses was least employed (67.6%). Only 74.4% washed their hands before gloving. Figure-IV shows preventive measures undertaken by the practitioners in their day today practice. Least preventive measure practiced was engaging in any kind of sports activity (20%). Only 20.4% reported to use loupes during practice. Only 40.8 % dentists practiced regular physical exercises. Only 56.4% of the practitioners went on yearly vacations. 61.2% dentists used indirect vision for working on maxillary teeth. Figure-V shows the prevalence of different occupational hazards. 57% experienced lower back pain, which was the most experienced hazard. 52.8% experienced neck pain, 38.4 % reported head ache, 23.6% reported wrist pain, 22.4 % reported frequent respiratory illness and 21.6% reported vision problems. Only 5.2% reported history of hepatitis B/C. The analyses were performed with use of SPSS version 20.0 package. The data was analysed using frequency tables to suggest the responses of dentists. The significance of differences between variables was tested by the cross tabulations. Results were considered significant for “p” values of ≤0.05.
DISCUSSION
Education is one of the important strategies for the prevention of occupational injuries and diseases. The role of one’s occupation as an important factor in maintaining personal health needs to be constantly emphasized so practitioners understand any possible negative health implications of their jobs and how to minimize them. In our survey on two hundred and fifty practicing dentists, backache was observed as being highest (57%) followed by neck ache (52.8%) and head ache (38.4%). About 28.4% reported contact with amalgam. Negligence in handling amalgam has to be avoided and safety handling protocols according to the FDI/WHO guidelines will have to be followed. [9][19] Although the majority of the participants were aware they were at risk for exposure to injuries from sharps, and hepatitis B infection, not all of them were vaccinated against Hepatitis B infection. Importance of vaccination properly against Hepatitis B infection has to be emphasised because of the risk of body fluid borne infection [20][21]; this is corroborated by the fact that about 12.8% experienced an injury by a sharp object in the past six months. Awareness about the HIV policy and the post expositional prophylaxis should also be increased. [21] Only 74% had health insurance policy. Cessation of practice due to health issues will have to be anticipated and accordingly the clinician’s health has to be insured to protect them from severe financial loss. Cross infection control habits among the staff could be rated very well because most of the clinicians appeared to have followed all the protocols except the use of protective eye goggles while attending to patients.[4][5][22] The use of protective eyewear is an important means of preventing occupational injury related to the use of dental curing lights and high-speed rotary instruments. Injury from splatters and projectiles including calculus and flying debris during cavity preparation is a common cause of damage to the eyes, and the use of protective eyewear should be emphasized. [4][5][22] The most pernicious occupational hazards are not those where the effects appear immediately, as in accidents, but rather those that run an insidious course over a period of years.[23]Musculoskeletal disorders represent an important occupational health issue in dentistry that surfaces after prolonged period of practice.[23][24][25] As clinicians adapt to the work- place and routine functions over a long period of time, they are exposed to potential hazards like musculoskeletal deformities. [23][24] Clinician’s safety may be severely jeopardized if adequate safety measures are not taken. [2] 57.8% reported lower back ache which scored the highest among all the occupational hazards experienced followed by neck pain and head ache. The postures in which dentists sit require over half of the body’s muscles to work to hold the body motionless while resisting gravity. The static forces resulting from these postures have been shown to be more taxing than dynamic forces [26]. Therefore, when the supporting muscles begin to reflect fatigue, a process of pain and discomfort begins and could very well lead to musculoskeletal injury. An article by Valachi and Valachi cited a flowchart of muscle activity and pain leading to a musculoskeletal disorder: Prolonged Static Posture→ Muscle Fatigue and Muscle Imbalance→ Muscle Ischemia/Necrosis, Trigger Points and Muscle Substitution→ Pain→ Protective Muscle Contraction→ Nerve Compression, Spinal Disk Degeneration→ Musculoskeletal Disorder. Muscle imbalances could result from an awkward posture while working on patients [27]. Electromyography (EMG) is the study of muscle function through analysis of electrical signals emanated during muscular contractions [28]. These signals represent the electrical activity associated with contracting muscles and, therefore, can be affected by anatomical and physiological muscle properties. EMG analysis could give an insight into the developing muscle fatigue progressing towards more complicated nerve compression. Hence, we felt that probably preventing the development of musculoskeletal disorders is the best choice by following simple regular physical exercises, engaging in some sports activity and regular check up with EMG. If muscle fatigue, which is experienced at initial stages, can be diagnosed, appropriate treatment can be taken. This might prevent the clinician from taking painful decisions like cessation of practice or reduction of clinical practice. Conclusion: Health risks in dentistry may arise as new technologies and materials are being developed. Our effort has been to assess the prevalence of occupational hazard among the clinicians in Chennai. Musculoskeletal disorders seems to be the highest experienced according to our study. Prevention of musculoskeletal disorders is very much a possibility by simple protocols mentioned in our discussion. However, further research is needed to explore the impact of musculoskeletal disorders in this particular occupational group, especially in relation to cessation or reduction of clinical practice.
References:
1. Gambhir RS, Singh G, Sharma S, Brar R, Kakar H. Occupational health hazards in current dental profession – a review. Open Occup Health Saf J. 2011; 3: 57-64.
2. Asuzu MC. Occupational health: A Summary, introduction, and outline of principle. Ibadan. Afrika-Links Books, 1994: 1-11.
3. Al-Khatib IA, Ishtayeh M, Barghouty H, Akkawi B. Dentists’ perceptions of occupational hazards and preventive measuresin East Jerusalem. East Mediterr Health J 2006; 12: 153-60.
4. Eriksen P, Moscato PM, Franks JK, et. al. Optical hazard evaluation of dental curing lights. Community Dent Oral Epidemiol. 1987 Aug; 15(4):197-201.
5. Palenik CJ. Eye protection in dental laboratories. J Dent Technol. 1997 Sep; 14(7):22-6.
6. Caballero AJ, Palencia IP, Cardenas SD. Ergonomic factors that cause the presence of pain muscle in students of dentistry. Med Oral Patol Oral Cir Bucal 2010; 15: e906-11.
7. Pargali N, Jowkar N. Prevalence of musculoskeletal pain among dentists in Shiraz, Southern Iran. International J Occup Environ Med 2010; 1: 69-74.
8. Hensten-Pettersen A, Jacobsen N. The role of biomaterials as occupational hazards in dentistry. Int.Dent J. 1990 Jun; 40(3):159- 66.
9. Al-Khatib IA, Darwish R. Assessment of waste amalgam management in dental clinics in Ramallah and Al-Bireh cities in Palestine. Int J Environ Health Res. 2004; 14:179–83.
10. Kostyniak PJ. Mercury as a potential hazard for the dental practitioner. N Y State Dent J. 1998 Apr; 64(4):40-3.
11. Field EA. The use of powdered gloves in dental practice: a cause for concern? J Dent. 1997 May-Jul;25(3-4):209-14
12. Saary MJ, Kanani A, Alghadeer H, Holness DL, Tarlo SM. Changes in rates of natural rubber latex sensitivity among dental school students and staff members after changes in latex gloves. J Allergy ClinImmunol. 2002; 109:131–5.
13. Babich S, Burakott RP. Occupational hazards of dentistry. A review of literature from 1990. N Y State .Dent J. 1997 Oct; 63(8):26-31. Review.
14. Yagiela JA. Health hazards and nitrous oxide: a time for reappraisal. AnesthProg. 1991 ; 38(1):1-11.
15. Henderson KA, Matthews IP. Environmental monitoring of nitrous oxide during dental anaesthesia.Br Dent J. 2000; 188:617– 9.
16. Ayatollahi J, Sharifi MR, Sabzi F, Zare AR. Blood level antiHBS due to HB vaccine in health care personnel of ShahidSadoughi Hospital-Yazd. Iranian Journal of Obstetrics, Gyneocology and Infertility. 2004; 7:48–51.
17. Ayatollahi J. Needle-stick injuries in a general hospital: Continuing risk and under reporting. Ann Iranian Med. 2006; 3:47–50.
18. Younai FS. Health care-associated transmission of hepatitis B and C viruses in dental care (Dentistry) Clin Liver Dis. 2010; 14:93–104.
19. Szymanska J. Occupational hazards of dentistry. Ann Agric Environ Med. 1999; 6:13–9.
20. De Almeida OP, Scully C, Jorges J. Hepatitis B vaccination and infection control in Brazilian dental practice, 1990. Community Dent Oral Epidemiol. 1991 Aug; 19(4):225-7.
21. Updated U.S. Public Health Service. Updated U.S. public health service guidelines for the management of occupational exposures to HBV, HCV and HIV and recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2001; 50:1–52.
22. Miller C. Make eye protection a priority to prevent contamination and injury. RDH. 1995; 15:40–2.
23. Szymanska J. Disorders of the musculoskeletal system among dentists from the aspect of ergonomics and prophylaxis. Ann Agric Environ Med. 2002; 9:169–73.
24. Hayes MJ, Cockrell D, Smith DR. A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009; 7:159–65.
25. Ratzon, N.Z., Yaros, T., Mizlik, A. and Kanner, T. Musculoskeletal symptoms among dentists in relation to work posture. Work; A Journal of Prevention, Assessment and Rehabilitation.2000; 15 (3), 153-158.
26. Valachi B, Valachi K. Mechanisms leading to musculoskeletal disorders in dentistry. J Am Dent Assoc.2003; 134:1344–50.
27. Sandoval, AE. “Electrodiagnostics for low back pain.” Physical medicine and rehabilitation clinics of North America. 2010; 21 (4): 767–76.
28. Leggat PA, Smith DR. Musculoskeletal disorders self-reported by dentists in Queensland, Australia. Aust Dent J. 2006; 51(4): 324-7.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





