IJCRR - 13(10), May, 2021
Pages: 36-40
Date of Publication: 19-May-2021
Print Article
Download XML Download PDF
Incidence of Bacterial and Fungal Infections in Otitis Externa Patient36
Author: Bhuvaneshwar GA, Meenakshi M, Deepak Raj K
Category: Healthcare
Abstract:Introduction: Otitis externa is the condition that causes the diffuse inflammation of the external auditory meatal skin which may spread to involve the pinna and the epidermal layer of the tympanic membrane, not extending into the middle ear. Otitis externa can be either acute or chronic Objective: To determine the causative factor of otitis externa and to investigate whether it was bacteria or fungal infection caus�ing the inflammation extensively. Methods: It is a clinico-social, prospective, cohort study conducted at ENT department of Saveetha medical college, India. About 40 patients who were diagnosed with otitis externa were taken in for study. After plotting demographic details, history, symptoms and predisposing factors in excel sheets, three specimens of affected external ear canal were taken in cotton swabs. The first swab was processed for aerobic bacteria in 5% sheep blood and the second one was placed in thioglycolate broth and the last was kept in sabouraud dextrose agar with antibiotics for fungal organisms. Results: Among 40 patients, females were more affected. The common predisposing factors were bathing in waterbodies, head baths and ear trauma. The most common symptom was otalgia. In case of microbiological study, Of the 40 patients, 32 were positive for bacteria and the others were for fungal. Among the bacteria, Staphylococcus aureus (30%) were the most common bacterial agent followed by Pseudomonas Aeruginosa (25%) and others. Conclusion: The management of otitis externa involves prevention, aural toileting and topical antibiotics. Delayed treatment may lead to complications like CSOM, mastoiditis and oth�ers.
Keywords: Otalgia, Otitis externa, Staphylococcus aureus
Full Text:
INTRODUCTION
Otitis externa is the condition that causes the diffuse inflammation of the external auditory meatal skin which may spread to involve the pinna and the epidermal layer of the tympanic membrane, not extending into the middle ear.1 Otitis externa can be either acute or chronic. Inadequately incompletely improperly treated acute otitis externa becomes chronic otitis externa. In some cases, it may occur in the localized form such as furuncles with severe pain and tenderness, which are confined to the hairy cartilaginous part of meatus only. In immunocompromised individuals, the otitis externa manifest as a more aggressive form and is called malignant otitis externa.
Like all skin in the body, the external auditory canal also has normal bacterial flora and a defence mechanism to protect it from bacterial infection. the predisposing factors that break the normal defence mechanism of the ear are common unhealthy day to day activities like swimming in unclean water, trauma from cerumen removal, use of external devices such as hearing aids for a prolonged duration, and cerumen removal with pins or buds, vigorous cleaning. These factors lead to loss of cerumen causes which in turn causes a fall in pH of the ear canal leading to bacterial growth and water retention, this causes the damage of the epithelial lining of the External AuditoryCanal.2 Other factors to include common skin conditions such as eczema and seborrhea, which if picked up earlier, the progression to otitis externa can be prevented.
The most common symptom associated with otitis externa is severe ear pain which is highly distressing to the patient that it interferes with his day to day activities. The usual aetiology of otitis externa is infective mostly bacterial. Staphylococcus, pseudomonas, klebsiella were the commonly isolated organisms from fungal culture. Previous studies have reported an increasing trend in fungal aetiology of otitis externa, due to increased use of topical antibiotics.3
Our study aimed to determine the incidence of bacterial and fungal agents present in the ear swabs taken from the patient’s with otitis externa and to assess the predisposing factors and clinical characteristics of otitis externa in Saveetha medical college
MATERIALS AND METHODS
It is a prospective observational study conducted at save the medical college hospital, Thandalam, Tamilnadu. Institutional review board approval was obtained (IEC Approval Number: SMC/IEC/2020/03/319), and after the individual, informed consent ear swab was taken from 40 consecutive patients diagnosed with otitis externa. This study was conducted for three months and included 40 patients diagnosed with otitis externa. There were 18 males and 22 females with their ages ranging from above 15 to below 70.
Patients with a history of ear pain, itching, Facial pain, Headache and ear discharge of varied types like (white mucous, thick purulent, thin watery with musty odour, greenish-blue and yellowish discharge) were included for the study.
A detailed history was collected from all patients and a complete ENT examination was carried out by an otolaryngologist. Demographic data, history, symptoms and predisposing factors and examination findings were recorded in excel sheets for each patient. the patient was also asked to grade the pain based on the Numerical Rating Scale pain scale. For the detection of the causative agents, three specimens of the affected external canal were obtained with three separate sterile cotton swabs. The cavum of conchae and external meatus were cleaned with seventy per cent isopropanol before attaining the swabs, to avoid infections.
The first swab was processed for aerobic bacteria in 5% sheep blood, chocolate and MacConkey agar. The second swab was placed into an anaerobic thioglycolate broth and the last was placed in Sabouraud dextrose broth with antibiotics for fungal organisms. Aerobic specimens are inoculated within 60 minutes into 5% sheep blood, chocolate and MacConkey agar and examined after 24 to 48 hours. Anaerobic specimens are inoculated within 60 min into thioglycolate broth and plated on anaerobic blood agar which was examined 48/96/120 hours. Fungal cultures were evaluated for isolation of any fungal growth after incubation at 25 to 26 degree for two weeks.
The results are obtained accordingly after inoculation of the swabs. All the data were entered in excel spare sheets and are analyzed by SPSS software and the statistical significance is calculated
RESULT
It is an incidence and socio-clinical study of bacterial and fungal infection in otitis externa patients in Saveetha medical college hospital, Thandalam, Tamilnadu. It is a perspective and observational type of study. The aim is to determine the causative factors of otitis externa and to investigate whether it was bacterial or fungal organisms causing the infection. The demographic details like age, sex, location, causative predisposing factors symptoms and examination findings are taken into consideration.
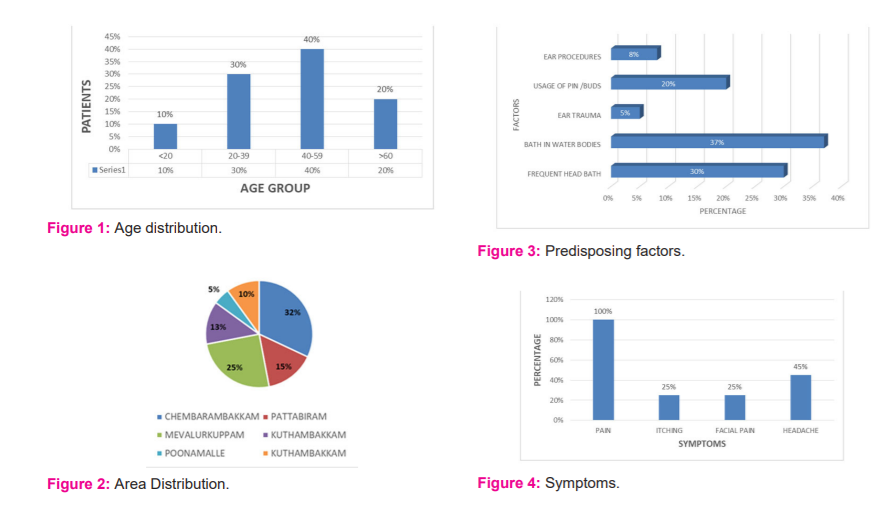
Of the 40 patients taken for the study, the total number of males were 18(45%) and the females were 22(55%). Patients between the age of below 20 to above 60 were enrolled for our study, in which the patients between the age of 40-59 were most affected and the ones below 20 were affected the least (Figure 1)
Among the enrolled 40 patients, most of the affected ones were from Chembarambakkam (13) and the others were from Mevalurkuppam(10), Pattabiram(6), Kuthambakkam (5), Maduravoyal (4) and Poonamalle (2) (Figure 2).
In our study, the most common predisposing factor is bathing in water bodies and staying for a longer time in the swimming pool which has affected about 15 of the 40 patients. While the other causative factors are listed in Figure 3.
On observing the symptoms given by the patients, it was revealed that the most common one was otalgia which was found in almost all the patients. Itching (10), Facial pain (10), and headache (18) were the other common symptoms complained about by the patients. The pain score percentage was also obtained from the patients ranging from mild to severe with most of them being on the moderate scale (Figure 4 and Table 1).
Examination findings are summarized in Figure 5. The polymicrobial nature of otitis externa was reflected in the study, the culture medium showed polymicrobial growth in 15% of swab cultures. fungal agents were found in 5% of swab cultures as polymicrobial and isolated growth in 15% (Figure 6).
Among the bacterial species, the most common causative agent was staphylococcus aureus (30%). While the second most common was Pseudomonas Aeruginosa (25%). These were followed by proteus (10%), Moraxella (7.5%) and Klebsiella (5%), most of them were aerobic facultative bacteria. Among the fungal organisms, the common species found were Candida Albicans which is a predominant etiological agent of otomycosis. The distribution of isolates in culture-positive cases is summarized in the table (Figure 7).
DISCUSSION
Otitis externa is one of the most painful inflammatory condition. In our socio-clinical study, about 40 patients diagnosed with otitis externa were enrolled after the local examination. In our study of 40 patients, 55% (22) of them were female and the other 45% (18) were male. Whereas in the study of Battikhi et al. in Oman, 100 patients among were men consisting of 55.5%.4 Cheong et al, a study in Singapore also found a frequency of 52.7% of male among 91 patients.5 Burgas et al. study reported that 56% of people affected were male.6 All the three studies that were being discussed contradicts the findings of our study. However, the study of Hajjartabar reported that 32.1% of patients taken under the study were women, which is following our study.7 The reason for the increased incidence of otitis externa in females can be due to the humidity affecting the ear condition as most of them were housekeepers.
In our study, the middle-aged individuals ranging from 40 - 59 age were affected more but in the case of Rowland et al. study of the UK revealed that otitis externa were common in all the age groups, which seems to contradict our study.8 The reason for this can be due to lifestyle, environmental factors and the jobs of the patients under the study. The most common predisposing factor according to our study was bathing in waterbodies (37%) and frequent head baths (30%), the reason being excessive moisture that elevates the pH and removes the cerumen. when there is no cerumen PH is altered, since the cerumen secretes lysozymes and maintains pH and also Lipid nature of the cerumen prevents water accumulation and epithelial damage.11-13
In our study of 40 patients, otalgia, itching, facial pain and headache were the common symptoms complained by the patients. Tragal tenderness, external auditory oedema and discharge were the clinical findings obtained from the local examination. The study of Al-Assaf et al. reported that pain and ecthymas were the most common symptoms wherein oedema had a low incidence, which contradicts our study.9 The study of Schaefer et al. have reported inflammation, otalgia and itching were the most frequent symptoms which favour our study.10
In our study, swabs were taken from 40 otitis externa patients in which 80% of the causative agents were bacterial. Among the bacteria, the most common causative organism was Staphylococcus aureus which was responsible for about 30% of patients, followed by pseudomonas Aeruginosa which affected 25% of the patients. The study of Murat Enoz et al.11 in turkey which included 267 patients revealed, 68.16% of them was positive for aerobic facultative bacteria, 1.12% were positive for anaerobic bacteria and 30.71% were fungi. Among the aerobic facultative bacteria, staphylococcus aureus (24.34%) was the commonest causative organism followed by pseudomonas Aeruginosa (11.99%), which seems to be following our study. Nogueira et al. study of 27 otitis externa samples also revealed staph aureus to be the most common causative organism.12 However, in the case of Cheong et al. studies consisting of 91 patients in Iran showed that the most commonly cultured bacteria were Pseudomonas aeruginosa (31.6%) followed by Staphylococcus aureus (20%) which contradicts our studies results.13 In Argentina were also found to contradict our studies with Pseudomonas Aeruginosa as the most common bacteria.10,14
In our study, among the 40 patients, 20% of the causative agents were of fungal origin and was comparatively less than the bacterial origin. The most common causative fungal organism was found to be Candida albicans. Incidences of candida Albicans at a percentage of 2.38%, 1.62% and 1.72%, which was found to be under our study.15-17 Whereas Zaror et al. study of 20 patients revealed that the Aspergillus Niger (35%) was the most common one which seems to contradict our study.18 Another study in Iran also reported that hearing loss, otalgia and discharge were the most common ones. The results of our study and the others were not entirely consistent; however, otalgia was the commonest symptom among all the studies.18,19 Otitis externa usually resolve with topical antibiotics and analgesics within a week but in case of delayed presentation, it may extend into other severe complications like chronic external otitis media, mastoiditis, osteomyelitis and the most common malignant necrotizing otitis externa.19 So, the swimmer’s ear otitis externa is a common condition caused by bacteria and fungal which can be treated easily on early detection.
CONCLUSION
Swimmer’s ear is one of the local names given to the medical condition otitis externa. It is an infection of the external ear canal and is commonly seen in primary health care hospitals. It has a prevalence of 1% and the incidence tends to be higher in hot and humid conditions. Otitis externa is usually a clinical diagnosis. It is based on a detailed history and examination of the ear using an otoscope. The mainstay of management in otitis externa involves prevention, aural toileting, topical antibiotics, simple analgesics and health education. No single topical antibiotics regimen is superior. The choice depends upon the causative organisms (bacteria and fungi), patient and the doctor preference, local sensitivity and adverse reactions of the drug. Steroid drops were beneficial when there is evidence of oedema with inflammation. Aural toileting is the most important single factor in the treatment of otitis externa. All the exudates and debris should be meticulously and gently removed.
DECLARATION
Funding: No funding was received for conducting this study
Conflicts of interest/Competing interests: All authors declare that they have no
Code availability MS excel
Author’s contribution: All authors contributed to the study’s conception and design.
Ethical Clearance: institutional ethical committee clearance was obtained.
Acknowledgement:
I would like to thank the faculty of the Department of Otorhinolaryngology of Saveetha Medical College and Hospital for their constant support and guidance in the completion of the research. I would like to thank all others who were involved directly and indirectly in the study and also the patients who participated in the study.

References:
-
Dhingra PL, Dhingra S. Diseases of ear, nose and throat and head and neck surgery.
-
Enoz M, Sevinc I, Lapena JF. Bacterial and fungal organisms in otitis externa patients without fungal infection risk factors in Erzurum, Turkey. Braz J Otorhinolaryngol. 2009;75(5):721-5.
-
Jackman A, Ward R, April M, Bent J. Topical antibiotic induced otomycosis. Int J Pediatr Otorhinolaryngol 2005;69(6):857-60.
-
Battikhi MN, Ammar SI. Otitis externa infection in Jordan: Clin Microbiol Features Saudi Med J 2004;25(9):1199–203.
-
Cheong CS, Tan LM, Ngo RY. Clinical audit of the microbiology of otorrhoea referred to a tertiary hospital in Singapore. Singapore Med J 2012;53(4):244–8.
-
Sanchez BA, Menaches Guardiola MI, Gras Albert JR, Talavera SJ. Descriptive study of infectious ear disease concerning summer. Acta Otorrinolaringol Esp 2000;51(1):19–24.
-
Hajjartabar M. Pseudomonas aeruginosa isolated from otitis externa associated with recreational waters in some public swimming pools in Tehran. Arch Clin Infect Dis 2010;5(3):142–51.
-
Rowlands S, Devalia H, Smith C, Hubbard R, Dean A. Otitis externa in UK general practice: a survey using the UK General Practice Research Database. Br J Gen Pract 2001;51(468):533–8.
-
Al-Asaaf SM, Farhan MJ. Otitis externa in a localized area at the South of Jordan. Saudi Med J 2000;21(10):928–30.
-
Schaefer P, Baugh RF. Acute otitis externa: an update. Am Fam Physician 2012;86(11):1055–61.
-
Enoz M, Sevinc I, Lapeña JF. Bacterial and fungal organisms in otitis externa patients without fungal infection risk factors in Erzurum, Turkey. Braz J Otorhinolaryngol 2009;75(5):721-5.
-
Nogueira JC, Melo Diniz Mde F, Lima EO, Lima ZN. Identification and antimicrobial susceptibility of acute external otitis microorganisms. Braz J Otorhinolaryngol 2008;74(4):526–30.
-
Cheong C, Tan ML, Ngo RY. Clinical audit of the microbiology of otorrhoea referred to a tertiary hospital in Singapore. Singapore Med J 2012;53(4):244.
-
Amigot SL, Gomez CR, Luque AG, Ebner G. Microbiological study of external otitis in Rosario City, Argentina. Microbiological study of external otitis in Rosario City, Argentina. Mycoses 2003;46(8):312-5.
-
Jadhav VJ, Pal M, Mishra GS. Etiological significance of Candida albicans in otitis externa. Mycopathologia 2003;156(4):313-5.
-
Erkan M, Soyuer U. Otomycosis in Kayseri (Turkey). Rev Iberoam Micol 1991;8:92-94.
-
Jaiswal SK. The fungal pattern of the ear and its sensitivity pattern. Indian J Otolaryngol 1990, 42: 19-22.
-
Zaror L, Fischman O, Suzuki FA, Felipe RG. Otomycosis in São Paulo. Rev Inst Med Trop Sao Paulo 1991;33(3):169-73.
-
Kurnatowski P, Filipiak J. Otitis externa: the analysis of the relationship between particular signs/symptoms and species and genera of identified microorganisms. Wild Parasitol 2008;54(1):37–41.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





