IJCRR - 13(9), May, 2021
Pages: 59-62
Date of Publication: 07-May-2021
Print Article
Download XML Download PDF
A Study of Skin Infections Following Percutaneous K Wire Fixation of Distal Radius Fractures in Elderly
Author: S Panakkal Ajay, V Rajiv Shwetha, Kumar K V Aneesh
Category: Healthcare
Abstract:Introduction: Lower end radius fractures are one of the most common fractures that we deal with in the Department. Almost one-third of the cases in here are these. Elderly patients are more commonly involved in these fractures. The mode of treatment depends upon many factors. But the commonest employed is the K-Wire fixation. But we found that in the elderly population the rate of infections was higher. So this study puts in a sincere effort to find the pattern in the above-mentioned cases.
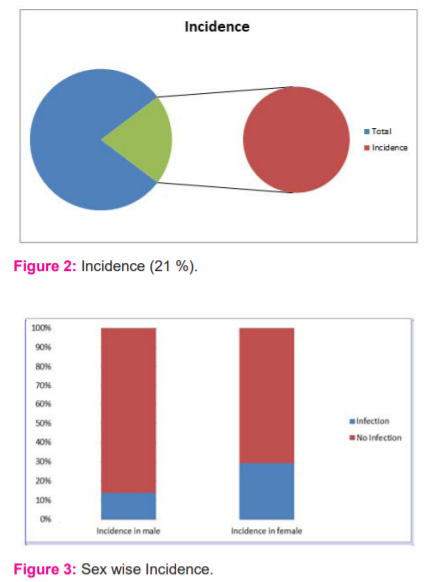
Objectives: To find the incidence of skin infections following the percutaneous k wire fixation of distal radius fractures in the elderly.
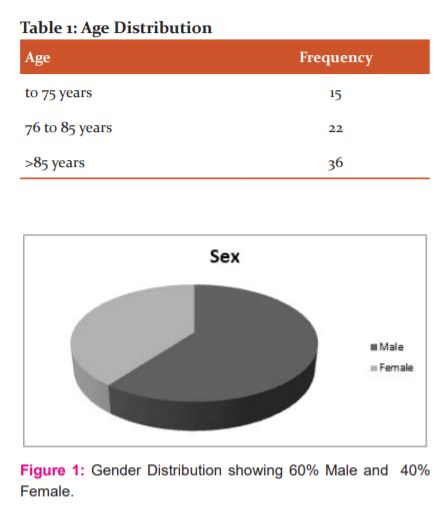
Methods: Seventy-three patients were taken as the sample size for the study. Out of these forty one were male and the rest were females. A careful history of the subjects was taken. Co-morbidities and other conditions if any were noted.
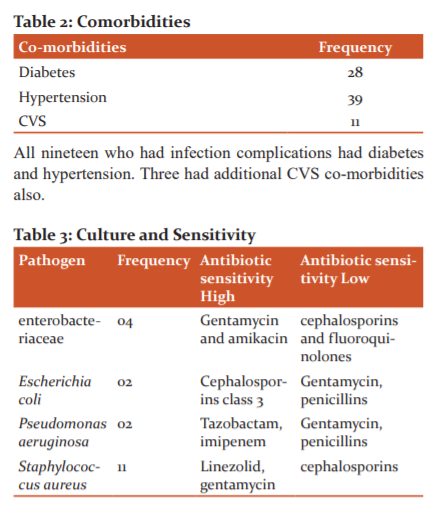
Results: Staph aureus was found to be the most common pathogen which was involved. And the incidence was more observed in females.
Conclusion: With proper and timely management we can save the patient from unnecessary complications. But one has to be vigilant and know these facts.
Keywords: Skin infections, K-wire fixation, Elderly, Complications, Radius, Fracture
Full Text:
INTRODUCTION
Around 15 to 2000 % of all fractures admitted in the Orthopedic ward are of the distal end of the radius.1 The treatment depends on age and several other demographic factors. The treatment includes both conservative and surgical options.2 For a very long time the conservative treatment has been used but many studies indicate the fact that it would be associated with collapse and would not be the choice of treatment in the elderly. So the open reduction and fixation is the choice of treatment especially in the elderly.1,3
Usually, the treatment is very safe and a very less number of cases is reported to have complications.4 There are many types of surgery followed by the operating surgeons in different geographical locations and the complications depend on the surgery and also the operating surgeon.5 Also the complications depend upon the patient's age, lifestyle, associated co-morbid conditions and other factors. Many studies have pointed out the fact that the increase in age and non-compliance with treatment leads to an increased number of complications.6 The surgeon should weigh in proper risk factors and then take the action for the best mode of treatment. This study puts in a sincere effort to identify the incidence of skin infections following the percutaneous k wire fixation of distal radius fractures in the elderly. This study also tries to find the culture and sensitivity pattern and also the management and outcomes of such cases.
MATERIALS AND METHODS
This study was done in the Department of Orthopaedics in collaboration with the Department of Dermatology in Malabar Medical College, Calicut, India. This study was done from August 2018 to July 2020.
Inclusion Criteria: Patients above 65 years.
Exclusion criteria:
-
The patients who were on immunosuppressant therapy
-
Patients who were on chemotherapy
-
Patients who were on radiotherapy.
-
Open fractures and patients with polytrauma.
Procedure
Seventy-three patients were taken as the sample size for the study. Out of these forty one were male and the rest were females. A careful history of the subjects was taken. Co-morbidities and other conditions if any were noted. A pre-Anaesthetic evaluation was done. Pre-surgical prophylactic antibiotics were started and then taking all anti-septic precautions the patients were operated on. Post-operative prophylactic antibiotics were continued.
The patients were followed up after a week and then after three weeks. The inspection of the surgical site was conducted and no infection was reported. Then a swab was taken and the specimen was transferred to the Department of Microbiology. Culture and sensitivity were done. After the reports, the patients have managed accordingly. In the end, the outcome of the patients was reported.
Results
DISCUSSION
Many studies have reported that the infection rate after k wire fixation is more when compared to the other procedures.7,8 There are a plethora of signs and symptoms that will be displayed by the patients. The commonest symptoms are fever and pain. Then around the surgical site redness, tenderness and even discharge can be noticed. Many studies have pointed out that the infections are very common with K-Wire fixation than in other procedures7,8. According to a study conducted by Esposito et al.9, the infection was reported in around ten per cent which was very much high when compared to that of other procedures.9 Another study conducted by Margaliot Z, et al. reported that the infection rate was found to be around 0.8 per cent when treated with internal fixation. All these statistics have to be considered when the treatment plan is considered for a particular patient. One common practice is to leave the K- wire outside the skin. Such practise should not be considered and followed as many studies have reported that the K wire has to be kept under the skin to minimize the chances of infection.12
Any of the invasive techniques will be associated with the risk of having infections. Egol et al. 11 in their study tried to differentiate the rate of infections using chlorhexidine and hydrogen peroxide-based dressings compared to that of other common dressings but did not find any difference between the two. They also observed that the rate of infections at the site increased with age. A contaminated wound is known to be associated with more chances of infections. So this has to be kept in mind before the line of treatment opted.12 Even though in our country the prophylactic antibiotics have been used extensively some studies have indicated that the use of prophylactic antibiotics will be of no much difference.13
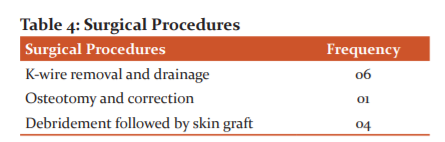
If the infection is there then the next management lines should depend on the extent of infection. Mild to moderate does not need the removal of the K wire. 14,15. Corrective osteotomy, removal of the K wire and debridement may be needed if the infection would be extensive.16
CONCLUSION
This study is a result of a sincere effort to find the frequency of skin infections following percutaneous k wire fixation of distal radius fractures in the elderly. The number of incident cases increased as the patient's age increased. The incidence was observed more in females. All the patients had co-morbidities. Staph aureus was found to be the most common pathogen involved. All the cases were found to be effectively treated as no mortality was found.
ACKNOWLEDGEMENT: We thank the Department of dermatology for the immense help that they have shown.
Conflict of Interest: Nil
Authors Contribution:
-
-
-
-
Dr S Panakkal Ajay: Lead investigator
-
Dr V Rajiv Shwetha: Lead investigator
-
Dr Kumar K V Aneesh: Lead investigator, compiling and statistics.
References:
-
Ilyas AM, Jupiter JB. Distal radius fractures, classification of treatment and indications for surgery. Orthop Clin North Am 2007;38(2):167–73.
-
Davis DI, Baratz M. Soft Tissue Complications of Distal Radius Fractures. Hand Clin 2010;26(2):229.
-
Schneppendahl J, Windolf J, Kaufmann RA. Distal radius fractures: current concepts. J Hand Surg Am 2012;37(8):1718–25.
-
McKay SD, Assessment of complications of distal radius fractures and development of a complication checklist. J Hand Surg Am 2001;26(5):916–22.
-
Rhee PC, Dennison DG, Kakar S. Avoiding and treating perioperative complications of distal radius fractures. Hand Clin 2012;28(2):185–98.
-
Chung KC, Kotsis SV, Kim HM. Predictors of functional outcomes after surgical treatment of distal radius fractures. J Hand Surg Am 2007;32(1):76–83.
-
Hargreaves DG, Drew SJ, Eckersley R. Kirschner wire pin tract infection rates: a randomized controlled trial between percutaneous and buried wires. J Hand Surg Br 2004;29(4):374–6.
-
Ahlborg HG, Josefsson PO. Pin-tract complications in external fixation of fractures of the distal radius. ActaOrthop Scand 1999;70(2):116–118.
-
Esposito J, External fixation versus open reduction with plate fixation for distal radius fractures: a meta-analysis of randomised controlled trials. Injury 2013;44(4):409–16.
-
Margaliot Z, A meta-analysis of outcomes of external fixation versus plate osteosynthesis for unstable distal radius fractures. J Hand Surg Am 2005;30(6):1185–99.
-
Egol KA, Treatment of external fixation pins about the wrist: a prospective, randomized trial. J Bone Joint Surg Am 2006;88(2):349–54.
-
Glueck DA, Charoglu CP, Lawton JN. Factors associated with infection following open distal radius fractures. Hand 2009;4(3):330–4.
-
Subramanian P, Complications of Kirschner-wire fixation in distal radius fractures. Tech Hand Up Extrem Surg 2012;16(3):120–3.
-
Hargreaves DG, The role of biofilm formation in percutaneous Kirschner-wire fixation of radial fractures. J Hand Surg Br 2002;27(4):365–8.
-
Santy J. A review of pin site wound infection assessment criteria. Int J Orthop Trauma Nurs 2010;14(3):125–131.
-
Turner RG, Faber KJ, Athwal GS. Complications of distal radius fractures. Orthop Clin North Am 2007;38(2):217–28.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





