IJCRR - 13(9), May, 2021
Pages: 46-51
Date of Publication: 07-May-2021
Print Article
Download XML Download PDF
Fertility Transitions in Qatar: The Dynamics between Women's Socioeconomic Status and Fertility
Author: Noora Ahmed Lari, Noof Abdulhadi Al-Rakeb
Category: Healthcare
Abstract:Introduction: Qatar society has undergone major socio-economic transformations that have eventually promoted female access to education and career opportunities, which has, in turn, impacted fertility preferences.
Objective: This paper examines the determinants of Qatari women's socioeconomic characteristics on fertility rates and preferences, as well as their policy implications.
Methods: Data from a 2018 fertility survey project with a random sample of 607 Qatari households, collected via personal interviews using a questionnaire programmed into a computer-assisted personal interview system, were examined based on a multi-dimensional model. The data were analyzed using logistic and Poisson regression techniques.
Results: The results demonstrated that the Qatari women's average fertility rate was 3.2, with the women in the 20\?29 age group having the highest fertility rate. An evaluation of the effects of women's educational attainment and employment status revealed no significant factors influencing the age-specific fertility rate of Qatari women. The use of family planning methods was more prevalent in older women who have had more children than younger women.
Conclusion: The paper concludes with practical family-friendly policy implications for higher authorities in response to the declining fertility rate among Qatari women by elucidating the sustainable development goals concerning Qatari national reproductive health.
Keywords: Fertility rates, Women, Education, Employment status, Qatar
Full Text:
INTRODUCTION
The existing literature has presented several factors contributing to the decline in the global total fertility rate and its relevant impact on the number of live births, which has decreased from 4.7 to 2.4. The effect of this decline on demographic transitions, coupled with the prevailing social and economic dynamics of the population, has also been previously discussed.1,2 Unsurprisingly, most of the Gulf Corporation Council (GCC) states have been experiencing high fertility levels, moderate mortality rates, and low contraceptive usage.3,4 It has been posited that Arab Gulf countries will continue to experience exponential population growth in the coming years. In June 2020, it was estimated that the total population in Qatar is 2.7 million,4but the current percentage of Qatari nationals only accounts for approximately 20% of the total national population.5,6 It is expected that the population in Qatar will reach 3.2 million by 2030.7
Nevertheless, Qatari nationals are expected to experience declining fertility rates, reduced number of mortality rates and increased life expectancy over the coming years.3,8 Between 2013 and 2017, the total fertility rate of Qatari women significantly declined, dropping from 3.30 births per woman to 2.94 in 2017.9 Given such projections, the Qatari authorities have considered infertility a national priority, and provided several initiatives to promote the fertility rate among its nationals while working on the reduction of expatriate recruitments as a means to address the imbalance in demographic transitions.10
Traditionally, Qatari society was based on patriarchal behaviours and gender roles, and women were not involved in making marriage decisions, resulting in a substantial number of them getting married off early to potential suitors.11 Although these traditions have not been fully overcome, it is imperative to underscore the fact that much progress has been made towards achieving gender parity and women empowerment in the Arab Gulf region. During the last 20 years, Qatar has undergone major social and economic transformations that have eventually culminated in increased industrialization and high rates of economic growth. This led to a shift toward a sedentary lifestyle that resulted in the promotion of female access to education and career opportunities for women in the labour market.6 Consequently, women have outnumbered their male counterparts in higher education, representing 34% of the total workforce of Qatar.12-14
Due to the aforementioned measures, as well as high rates of economic growth and higher rates of female literacy, declining total fertility rates continue to be recorded.15 The ripple effect is a delayed age of first marriage for women, with others preferring to practice celibacy, and declined fertility and reproduction. For instance, a study observed that uneducated and unemployed women are more likely to have more children compared to their educated counterparts.16 Eventually, this dynamic influences fertility levels in the sense that education becomes a predictive factor about the desired ideal family size, number of marriage years, frequency of contraceptive usage, and level of household income, which directly or indirectly affect fertility and reproduction.17
These dynamics demonstrate that women are increasingly becoming engaged with employment rather than establishing a family. In other words, they are progressively moving “away from home,” leaving limited opportunities for reproduction and shifting their fertility preferences. This is the premise of this paper, which will assess the determinants of Qatari women’s socioeconomic characteristics and fertility rates and their policy implications. This research is guided by the following research question: How and to what extent do women’s socioeconomic characteristics, such as age, level of education, employment status, and income level, contribute to declining fertility rates? Based on the results obtained from this research, it is expected that the practical recommendations will be able to address the implications of women’s fertility decline and raise the quality of family–work policies as a means to provide the possibility of a better reconciliation between childbearing and career responsibilities.
MATERIALS AND METHODS
This paper utilized a national survey on a representative sample consisting of 607 Qatari women conducted by the Social and Economic Survey Research Institute in 2019. The data were collected via personal interviews with a questionnaire programmed into a computer-assisted personal interview (CAI) system (BLAISE). The data were analyzed using the Statistical Software Package (STATA). Means with their corresponding standard deviations (SDs) were calculated for the continuous variables and proportions for the categorical variables. Potential variables (age, marital status, educational level, employment status, and the number of children) were incorporated in the univariate model, and their corresponding p-values were recorded. The model used these variables, which have been categorized as social and demographic variables that are likely to affect women’s fertility rates. All variables in which the p-value was less than 0.05 were considered for the Poisson and regression analysis.
Sample Characteristics
A total of 607 Qatari women were selected and interviewed. The age group from 33–40 years old constituted the largest percentage (36%), followed by the 41–49 years and 25–32 years’ age groups with a ratio of about one third each, and, finally, the younger age group from 18–24 years (the lowest percentage in the sample, 8%). The sample included Qatari women who were married or previously married. Most of the women who participated in the study were married (88%). The percentage of divorced women was 7%, that of widows was 3%, and that of separated women was 2%. The results indicated that 96% of the sample married once and a small percentage married twice (4%). The percentage of pregnant women who participated in the survey was 14% of the total sample. Table 1 presents the sample characteristics.
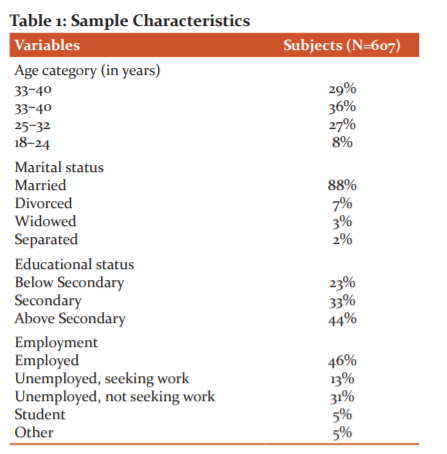
In terms of educational level and employment status, the percentage of Qatari women who achieved a higher education level than secondary constituted the largest percentage in the sample (41%), followed by those with an education lower than the secondary level (32%), and, finally, those with a high school diploma, who constituted about a quarter of the sample (26%). The percentage of employed Qatari women was 46%, those who were unemployed constituted about a third (31%), female students constituted 5%, and the retired women 2%. The percentage of Qatari women working in the professional jobs category comprised the largest percentage (38%), followed by the women working in the office jobs category with 23%, and, finally, 16% in the senior employees’ category (legislators, senior management employees, directors).
RESULTS
Total Fertility Rate
The data were analyzed statistically using fertility equations, as well as Poisson and logistic regression analysis. In this sample, the total fertility rate of Qatari women was three births per woman on average. The Age-Specific Fertility Rate (ASFR) was calculated using the equation below:17
Age-Specific Fertility Rate = the number of live births per woman at a specific age/number of women at that specific age
Sociodemographic Factors Associated with Fertility
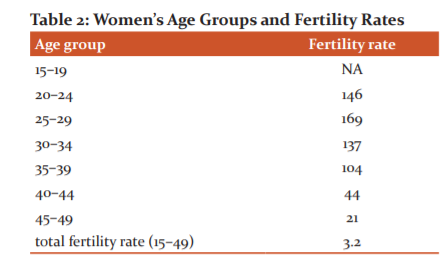
Table 2 depicts the fertility rate according to the women’s age groups. Based on the sample characteristics, the women in the 20–29 age group had the highest fertility rate, after which it declined in the older groups. Meanwhile, the percentage of women who have not given birth was 12%, with the majority coming from the age group 18–24 years.
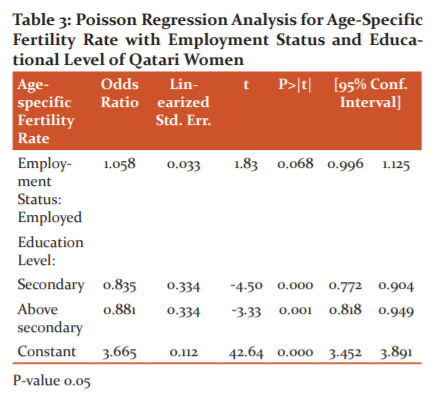
Poisson regression analysis was performed to measure the associations between the age-specific fertility rate and women’s educational level, employment status, and income level. The results revealed that the age-specific fertility rate decreased as the educational level of Qatari women increased (above secondary), which means that there is no relationship between age-specific fertility rate and women’s educational level. No associations were found between age-specific fertility rate and women’s employment status (Table 3).
Also, logistic regression analysis was performed to measure the desire of non-pregnant women (the sample consisted of 86% non-pregnant women during the time of the survey) to have another child relative to their employment status and educational level. The findings in Table 4 indicate that the women with a higher educational level (above secondary) had a greater desire to bear a child compared to the women with lower than secondary level education. This supports the findings in Table 1, as the women with a higher educational level (above secondary) desired to have one or more children since their age-specific fertility rate is low.

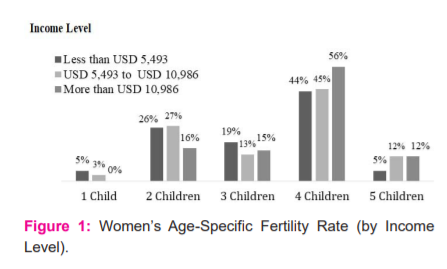
On the other hand, when Poisson regression analysis was performed, a direct relationship between women’s fertility rate and level of income was found. The age-specific fertility rate for high-income Qatari women was higher than that for low-income women because the age-specific fertility rate increased as the women’s income increased (Figure 1).
Family Planning Methods
To assess their fertility preferences, the prevalence of contraceptive usage was measured among the respondents, and a positive association was found between women’s access to employment and their level of income. The respondents were asked about their “intention to use family planning methods to postpone or prevent pregnancy shortly.” Almost 48% reported that they are currently using a contraceptive method as a means to postpone or prevent pregnancy (i.e., during the survey period).
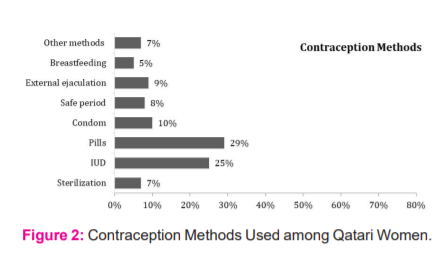
As depicted in Figure 2, pills constitute the most widely used method for postponing or preventing pregnancy among Qatari women (29%), followed by IUD (25%), condom (10%), safe period (8%), and breastfeeding (5%). A study conducted to measure the prevalence of contraceptive use among Qatari women also found that IUD and pills are among the most common contraceptive methods used by Qatari women .18
More than half of the employed women in full- or part-time jobs indicated that they were using contraceptive methods (53%) compared to 43% of the women who were not employed. In terms of the type of employment, the Qatari women who had administrative jobs (secretary, administrative assistant) tended to use contraceptive methods of postponement or contraception more than those with professional jobs (engineer, doctor, lawyer, teacher, accountant, and journalist). Figure 3 demonstrates that the use of postponement methods was more prevalent among older women than in the younger age groups. It was expected that the older women would have more children compared to the younger age group. This indicated that there was a significant association between the women’s age and the number of living children and the current use of contraceptive methods.

DISCUSSION
In the changing socio-economic dynamics, women have gone beyond regressive social constructs, such as being constrained to domestic chores and blindly following male orders.20,21 Several cross-country studies have stated that the dimensions of women’s education and empowerment compel women to have fewer children to raise their quality of life, as opposed to traditional times when childbearing was considered the norm in society.19,22,23 This is in line with the postulations of the theory of demographic transition, which argue that the main cause of fertility decline is the changing status of women (through access to employment and education, their assumption of important positions in society and decision-making, etc.), amongst other major developments.24
Since changes in social norms have taken place in Qatari society, where childbearing was once considered the norm, the country has been grappling with the issue of declining total fertility rates.15,25 One study found that Qatari women’s desire to have children decreases as they become increasingly empowered with expanded access to employment and education opportunities.13 This study contradicts our results, as we found that women’s reproductive preferences have not changed due to their educational level and that they are not associated with fertility differentials or decline. Rather, our analysis revealed that Qatari women with low age-specific fertility rate and higher education desire to have more children. These findings are consistent with the results of previous studies carried out in other Arab Gulf states, such as Oman and the UAE.17,26On the other hand, it indicated that the participation of women in the workforce leads to a decline in their fertility due to several reasons, including the inability to achieve the required balance between childcare and work duties, thereby leading to a delay in reproductive age.26,27
The results primarily demonstrated that an increase in the age of first marriage and prevention or delay in childbearing through the prevalent use of contraceptive methods by women have emerged as consequences. For instance, it was demonstrated that almost half of the non-pregnant women use contraceptives to postpone or prevent pregnancy (during the survey period), and more than half of those who work are currently using contraceptive means (53%) compared to 43% of those who do not work. Consistent with previous studies, Algur et. al.26, indicated that in terms of family planning preferences, females’ respondents were in favour of the use of contraceptives and birth control methods more than males’ respondents. The high level of usage of contraceptive methods among married working women is ascribed to the lack of family-friendly policies that contribute to balancing family responsibilities, parenting, childcare, and work duties. Several studies have indicated that employed women tend to use contraceptive methods to delay their pregnancy to a later time.28-31
Based on the results, it was also determined that age is a predictive factor for the decreased fertility in Qatari women.3,32 In fact, our empirical findings revealed that age may directly contribute to reduced fertility rates for women, as the use of postponement methods of contraception is more prevalent among older women who have given birth to many children compared to the younger age group. It follows that there is a strong positive correlation between old age and quality of life with the increased necessity for long-term care needs. The fact that the older generation has a higher dependency ratio means that the ageing population will be less willing to conceive and procreate.3 The Qatari authorities have increased the implementation of interventions to improve access to healthcare services and provided improvements in overall sanitation as a means to help reduce the mortality rates among older generations.10
CONCLUSION
Similar to most other Arab Gulf countries, Qatar has undergone major social and economic transformations, both of which have significantly influenced the level of fertility and birth rates in the country. This paper has presented the key socioeconomic determinants influencing fertility rates among Qatari women (e.g., education, employment, age, etc.). In light of research results and to increase the total fertility rate, several initiatives have been adopted in Qatar to encourage procreation, facilitate the establishment of families, mitigate child mortality rates, and increase live births while reducing or possibly averting stillbirths.
The following policy recommendations are considered as partial solutions to the existing ones: providing family-friendly initiatives to encourage working Qatari married women to increase their family sizes, such as subsidized childcare support and services, and strengthening the provision of paid maternity leave. Moreover, sufficient incentives in the workplace that would motivate Qatari women to have children, such as part-time jobs, flexible working hours, work-from-home options, and nursing rooms for children in the workplace should be implemented. The authorities should also regulate and promote the provision of high-quality family planning services, including the use of contraceptives. Finally, governmental plans for enhancing health services and addressing fertility-related issues can ensure an increase in the total fertility rate.
ACKNOWLEDGMENTS: The authors acknowledge the immense help received from the scholars whose articles are cited and included in the references of this manuscript. The authors are also grateful to the authors, editors, and publishers of all the articles, journals, and books that have been reviewed and discussed in this article.
Conflict of Interest: The authors declare that they have no conflict of interest to report.
Source of Funding: This publication was made possible by Program grant # NPRP9-190-5-022 from the Qatar National Research Fund (a member of the Qatar Foundation). The findings herein reflect the views of the authors alone and are solely the responsibility of the authors.
Compliance with Ethical Standards
All procedures performed in studies involving human participants were following the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The research protocol was approved by the institutional review board of the Qatar University, QU-IRB 597-EA/16, under which the Social and Economic Research Institute (SESRI) operates.
References:
-
Skakkebaek NE, Jørgensen N, Andersson A, Juul A, Main KM, Jensen TK, et al. Populations, Decreasing Fertility, and Reproductive Health. Lancet 2019;393(10180):1500–1501.
-
Mullay CJL. Population and Fertility by Age and Sex for 195 Countries and Territories, 1950–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2018;392:1995–2051.
-
Khan HTA, Hussein S, Deane J. Nexus Between Demographic Change and Elderly Care Need in the Gulf Cooperation Council (GCC) Countries: Some Policy Implications. Ageing Int 2017;42(4):466–487.
-
Planning and Statistics Authority. Population Statistics: Quarterly Bulletin (Second Quarter). Planning and Statistics Authority, 2020. https://www.psa.gov.qa/en/statistics1/Pages/Overview.aspx
-
Slaiby W. New Population Policy Seeks a Balanced Demographic Growth. Qatar Tribune. 2017. http://www.qatar-tribune.com/news-details/id/93490
-
Al–Thani MH, Sadoun E, Al-Thani A, Khalifa SA, Sayegh S, Badawi A. Change in the Structures, Dynamics and Disease-related Mortality Rates of the Population of Qatari Nationals: 2007–2011. J Epidemiol Global Health 2014;4(4):277–287.
-
United Nations. The World Population Prospects: The 2017 Revision. United Nations. 2017. https://esa.un.org/PopPolicy/cprofile_report.aspx
-
Araya D, Marber P. Higher Education in the Global Age: Policy, Practice and Promise in Emerging Societies. London: Routledge. 2013. https://www.routledge.com/
-
Planning and Statistics Authority. The Population Policy of the State of Qatar 2017-2022. Permanent Population Committee, Planning and Statistics Authority. 2017https://www.ppc.gov.qa/en/PopulationPolicy/NewPopulationPolicy/Pages/default.aspx
-
Planning and Statistics Authority. Births and Deaths in the State of Qatar 2017 – Presentation and Analysis. Planning and Statistics Authority. 2018. https://www.psa.gov.qa/en/statistics/Statistical%20Releases/Population/BirthsDeaths/2017/Birth_death_2017_AR.pdf
-
Alharahsheh MM, Mohieddin ST, Almeer FK. Marrying Out: Trends and Patterns of Mixed Marriage amongst Qataris. Int J Soc Sci Studies 2015;3(6):211–225.
-
Klasen S. What Explains Uneven Female Labor Force Participation Levels and Trends in Developing Countries? World Bank Res Observer 2019;34(2):161–197.
-
Khraif RM, Salam AA, Al-Mutairi A, Elsegaey I, Jumaah, A. Education’s Impact on Fertility: The Case of King Saud University Women, Riyadh. Middle East Fert Soc J 2017;22(2):125–131.
-
Young KE. Women’s Labour Force Participation Across the GCC. The Arab Gulf States Institute in Washington. Washington, DC. 2016. https://agsiw.org/wp-content/uploads/2016/12/Young_Womens-Labor_ONLINE-2.pdf
-
Zauner G, Girardi G. Potential Causes of Male and Female Infertility in Qatar.
J Reprod Immunol 2020;103173(141).
-
Kim J. Female Education and its Impact on Fertility: The Relationship is More Complex than One May Think. World of Labor 2016;228:1–10.
-
Al-Awad M, Chartouni C. Explaining the Decline in Fertility among Citizens of the GCC Countries: The Case of the UAE. Educ Busi Soc Contemp Middle Eastern Issues, 2014;7(2/3), 82–97.
-
Arbab AA, Bener A, Abdulmalik M. Prevalence, Awareness and Determinants of Contraceptive Use in Qatari Women. Eastern Mediterranean Health J 2011;17(1), 11–18.
-
Atake EH, Ali PG. Women’s Empowerment and Fertility Preferences in High Fertility Countries in Sub-Saharan Africa. BMC Women’s Health, 2019;19(1):54.
-
Yaya S, Uthman OA, Ekholuenetale M, Bishwajit G. Women Empowerment as an Enabling Factor of Contraceptive Use in Sub-Saharan Africa: A Multilevel Analysis of Cross-sectional Surveys of 32 Countries. Reprod Health 2018;15(1):214.
-
Blackstone SR. Women’s Empowerment, Household Status and Contraception Use in Ghana. J Biosoc Sci 2017;49(4):423–434.
-
Hameed W, Azmat SK, Ali M, Sheikh MI, Abbas G, Temmerman M, et al. Women’s Empowerment and Contraceptive Use: The Role of Independent Versus Couples’ Decision-Making, From A Lower Middle Income Country Perspective. PLoS One 2014;9(8):104633.
-
Upadhyay UD, Karasek D. Women’s Empowerment and Ideal Family Size: An Examination of DHS Empowerment Measures in Sub-Saharan Africa. Int Perspect Sexu Reprod Health 2012;38(2):78–89.
-
Brujin BJ. Fertility: Theories, Frameworks, Models, Concepts. In G Caselli, J. Vallin, GJ Wunsch(Eds.), Demography: Analysis and Synthesis. 2006:pp. 549–569). New York, Academic Press.
-
Winckler O. How Many Qatari Nationals Are There? Middle East Quarterly 2015;22(2).
-
Dorvlo AS, Bakheit CS, Al-Riyami A, Morsi M, Al-Adawi S. A Study of
Fertility Patterns of Ever Married Women in Oman. Sultan Qaboos Uni Med J 2006;6(2):33.
-
Algur VS, Kazi SA, Yadavannavar MC. Family Planning Practices among Rural Health Training Center Beneficiaries. Int J Curr Res Rev 2013;5(1):64-68.
-
James-Hawkins L Peters C, Van der Ende K, Bardin L, Yount KM. Women’s Agency and its Relationship to Current Contraceptive Use in Lower and Middle-income Countries: A Systematic Review of the Literature. Glob Public Health 2018;13(7):843–858.
-
Prata N, Fraser A, Huchko MJ, Gipson JD, Withers M, Lewis S, et al. Women’s Empowerment and Family Planning: A Review of the Literature. J Biosoc Sci 2017;49(6), 713–743.
-
Wyatt KD, Anderson RT, Creedon D, Montori VM, Bachman J, Erwin P, et al. Women’s Values in Contraceptive Choice: A Systematic Review of Relevant Attributes Included in Decision Aids. BMC Women’s Health 2014;14(1):28.
-
Sueyoshi S, Al-Khozahe HO, Ohtsuka R. ffects of Reproduction Norms on
Contraception Practice among Muslim Women in Amman, Jordan. Eur J Contrac Reprod Health Care 2006;11(2):38–45.
-
Sharma R, Biedenharn KR, Fedor JM, Agarwal A. Lifestyle Factors and Reproductive Health: Taking Control of Your Fertility. Reprod Biol Endocrinol 2013;11(66).
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





