IJCRR - 13(9), May, 2021
Pages: 40-45
Date of Publication: 07-May-2021
Print Article
Download XML Download PDF
Central Corneal Thickness in Diabetics and its Relation with Severity of Diabetic Retinopathy and Hyperglycemia Assessed by Glycosylated Hemoglobin in Central India
Author: Eva Rani Tirkey, Neha Adlakha, Charudatt Chalisgaonkar, Kailash Khairnar
Category: Healthcare
Abstract:Introduction: Diabetes Mellitus is the leading cause of blindness as a result of complications due to diabetic retinopathy. The metabolic status of the cornea is affected by changes in blood glucose levels. Metabolic stress due to hyperglycemia can alter central corneal thickness.
Objective: To compares central corneal thickness (CCT) in diabetics and non-diabetic controls and evaluates the relation of CCT with glycemic status and severity of diabetic retinopathy.
Methods: 180 subjects(93 diabetics and 87 non-diabetics) attending or referred to the Department of Ophthalmology of a tertiary care hospital were included in the study.CCT was measured in all subjects using an ultrasonic pachymeter.
Results: 93 patients were diabetic(Type 1 four and type 2 eighty-nine) of which 35 patients had no diabetic retinopathy,44 patients had non-proliferative diabetic retinopathy and 14 patients had proliferative diabetic retinopathy. Mean CCT in diabetics(563.11\?m \?11.40\?m)was found to be greater than non-diabetics (529.53\?17.91\?m)and the difference was statistically significant (p< 0.0001). Mean CCT in type 1 and type 2 DM patients was 562\?12.90\?m and 562.59\?9.44\?m respectively. There were 35 diabetic patients with good metabolic control(HbA1C < 7%) who had mean CCT 559.03\?8.32\?m.41 patients with poor metabolic control(HbA1C≥7) had a mean of CCT 565.04\?9.94\?m and the difference was statistically significant. Mean CCT in patients with no diabetic retinopathy, in patients with non-proliferative diabetic retinopathy and proliferative diabetic retinopathy was 558.81 \? 7.67um,563.81 \? 12.32 and 563.43 \? 9.70um respectively and the difference was not statistically significant.
Conclusions: A significant correlation was found between an increase in CCT and diabetes, with the positive correlation between thick cornea and duration of diabetes, indicating that patients with thick corneas are more likely to be found in the advanced stage of the disease. Measuring CCT in diabetic patients should be mandatory in the workup of refractive surgery, for donor tissue evaluation before keratoplasty, glaucoma suspects, contact lens users etc. This may help to identify patients at higher risk of developing severe complications, enabling ophthalmologists to treat their disease more accurately.
Keywords: Central corneal thickness, Complications, Diabetes Mellitus, Glycosylated Hemoglobin, Keratoplasty, Ultrasonic Pachymeter
Full Text:
INTRODUCTION
Diabetes mellitus is a metabolic disease that occurs due to an increased level of blood glucose, which can cause microvascular and macrovascular complications.1Failure of pancreatic beta cells to secrete an adequate amount of insulin can cause hyperglycemia, which influences genetic and environmental factors.2 Hyperglycemia has toxic effects on almost all cells in the body.3 Ocular complications of hyperglycemia are most remarkable in the cornea and retina.
Retinal impairment accounts for the majority of visual loss in diabetic patients Diabetic Retinopathy is the most common cause of blindness for people over the age of 50 years.4 Neovascular glaucoma, refractive changes5 and various corneal pathologies may be also seen. These include dysfunction in the corneal endothelium, desensitization,6 stromal and subbasal nerve abnormalities,7 low endothelial cell density and hexagonality,8 increased corneal autofluorescence,9 recurrent epithelial erosions, epithelial oedema, desensitization and neurotrophic ulcers.
Studies show that the eyes of patients with Diabetes Mellitus have a greater central corneal thickness (CCT) and that there is a positive correlation between CCT and the Grading of Diabetic Retinopathy.10 Control of corneal hydration appears to be compromised in corneas of diabetic patients.11 Corneal morphological evaluation is always very crucial in Ophthalmologists clinical practice. Ophthalmologists rely on corneal parameters such as central corneal thickness, anterior and posterior corneal curvature, anterior chamber depth or endothelial cells counts to make the diagnosis, to follow up or to plan treatment for refractive errors or diseases such as glaucoma, keratoconus, corneal ectasia or cataract.
There are varying reports on central corneal thickness (CCT) changes due to DM.12 To the best of our knowledge, there are only a few published studies on CCT in Diabetes Mellitus.13 In our study, we aimed to measure the difference in the mean CCT between diabetes and age-matched non-diabetic controls. Also, we evaluated the correlation between each of these values and the diabetic duration and hyperglycaemia assessed by HbA1C by measuring CCT using an ultrasonic pachymeter.
MATERIALS AND METHODS
Ethical clearance was obtained from the Institutional Ethical Committee ( Ethical clearance number – 138/ 03.06.2017) and an observational cross-sectional case-control study was designed in our tertiary eye care centre. A total of 180 subjects (93 diabetics and 87 non-diabetics) who gave consent were included in the study. Eyes with corneal pathologies like pterygium, corneal dystrophies, contact lens users, receiving treatment for any topical or systemic diseases, any prior history of ocular surgeries or ocular trauma were excluded from the study. Age, gender, duration of diabetes, HbA1c levels, the status of DR, any medical illness and prescribed medical treatment were recorded. All subjects underwent a complete ophthalmological examination that included visual acuity assessment using the Snellen chart, refraction using auto-refractometer, intraocular pressure measurement using applanation tonometry, slit-lamp biomicroscopy, and fundus examination. Grading of Diabetic Retinopathy was done according to the International clinical disease severity scale for DR. Central corneal thickness of all subjects was measured with an ultrasonic pachymeter.
The diabetic eyes were classified into 3 groups according to the status of DR (group without DR, group with non-proliferative DR [NPDR], and group with proliferative DR [PDR]). Also, they were divided into 2 groups according to DM duration (the group with a duration of fewer than 10 years and group with a duration of ≥10 years) and according to HbA1c value (the group with HbA1c less than 7 % and group with HbA1c more than or equal to 7%).
Statistical Analysis
Data were analyzed using SPSS software for windows. The results were expressed as mean ± SD. An independent sample t-test was performed to compare the means of CCT in diabetic and control groups. The differences among 3 or more groups were analyzed by one way ANOVA. Pearson correlation coefficient was done to find the relationship between corneal thickness and DM duration, HbA1c, and DR status. A value of P ≤ 0.05 was considered statistically significant.
RESULTS
The present cross-sectional study was conducted on 180 consecutive subjects in the Department of Ophthalmology in a tertiary care hospital. In this study 93 patients were diabetic (Type 1 four and type 2 eight nine), of which 35 patients had no diabetic retinopathy, 44 patients had non-proliferative diabetic retinopathy and 14 patients had proliferative diabetic retinopathy. Eighty-seven subjects were non-diabetic controls.
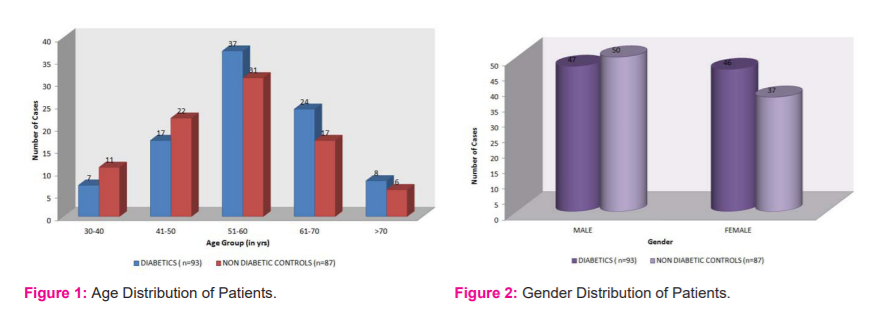
The age of all patients in the present study varied from 30 years to 80 years with a mean age of 55.41±10.94 years. The maximum number of patients in the diabetic group were in the age group of 51–60 years (39.7%) and the mean age of diabetic patients was 55.45±10.79 years, while in the non-diabetic control group it was in the age group of 51-60 years (35.6%) and the mean age of the non-diabetic group was 53.48±10.99 years. No significant difference was found between the mean age of diabetics and non-diabetic controls (p=0.227; Figure 1).
In the diabetic group, 47 (50.53%) were males and 46 (49.46%) were females while in the non-diabetic control group 50 (57.47%) were males and 37 (42.52%) were females. In this study, M: F ratio is 1.16:1 (Figure 2).
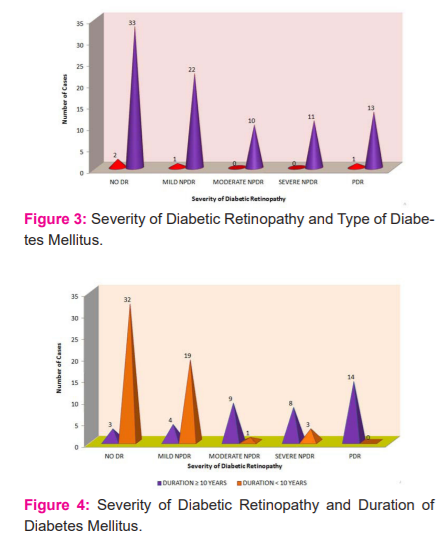
Out of 93 patients of DM, two patients of type 1 DM and 33 patients of type 2 DM had no diabetic retinopathy. One patient of type 1 DM and 22 patients of type 2 DM had mild NPDR. None of the patients of type 1 DM had moderate NPDR, while 10 patients of type 2 DM had moderate NPDR. Eleven patients of type 2 DM had severe NPDR. One patient of type 1 DM and 13 patients of type 2 DM had PDR. No diabetic retinopathy was the most common grade seen in 35 eyes and moderate NPDR was the least common grade found amongst diabetic patients (Figure 3).
Out of 93 patients of DM, three patients of ≥10 years duration of diabetes and 32 patients of <10 years duration of diabetes had NO DR. Four patients of ≥10 years duration of diabetes and 19 patients of <10 years duration of diabetes had mild NPDR. Nine patients of ≥10 years duration of diabetes and 01 patient of <10 years duration of diabetes had moderate NPDR. 8 patients of ≥10 years duration of diabetes and 03 patients of <10 years duration of diabetes had severe NPDR. Fourteen patients of ≥10 years duration of diabetes and no patients of < 10 years duration of diabetes had PDR (Figure 4).
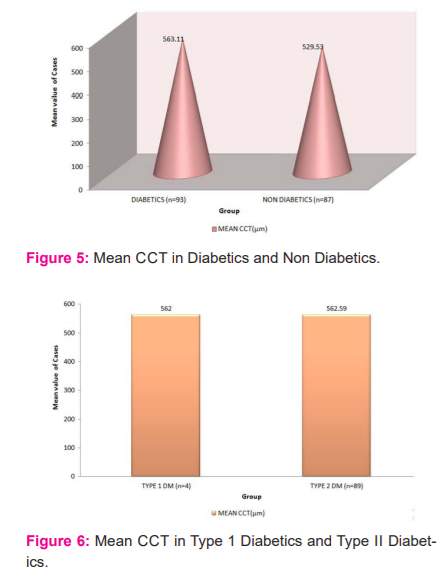
The mean CCT was measured in 93 diabetic patients and it was 563.11µm with a standard deviation of 11.40µm. The mean CCT was measured in 87 Non-diabetic controls and it was 529.53µm with a standard deviation of 17.91µm. The mean CCT in the diabetic group (563.11µm ±11.40µm) was found to be thicker than non-diabetic controls (529.53±17.91µm) and the difference was statistically significant (p<0.0001) using unpaired- t-test (Figure 5).
In our study, we compared mean CCT amongst type 1 and type 2 DM patients. There were four patients with type 1 DM and their mean age was 39.5±9.29 years with a mean duration of diabetes was13.75±12.28 years, while in the type 2 DM group mean age and mean duration of diabetes was 55.63±10.79 years and 8.82±5.49 years respectively. The mean CCT in type 1 and type 2 DM patients was 562±12.90µm and 562.59±9.44µm respectively, and the difference was not statistically significant (p=0.90, Figure 6).
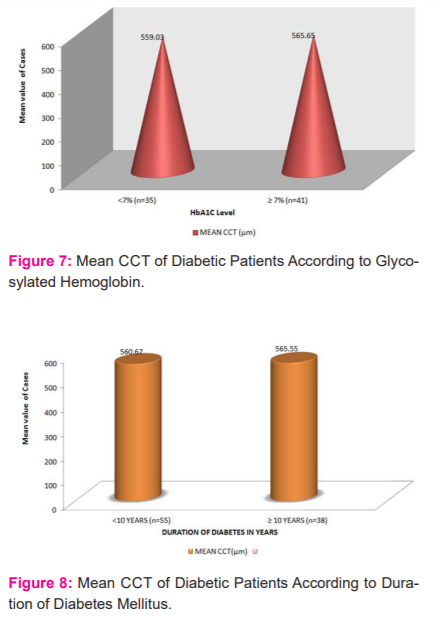
Out of 93 diabetic patients, eighty patients were investigated for glycosylated haemoglobin (HbA1C). There were 35 diabetic patients with good metabolic control (HbA1C <7%) and their mean CCT was 559.03±8.32µm. Forty-one patients with poor metabolic control(HbA1C≥7) had a mean CCT of 565.04±9.94µm. The difference was statistically significant (P=0.026) using an unpaired t-test (Figure 7).
In our study, we compared the mean CCT according to the duration of diabetes. Mean duration of diabetes was 8.82±5.48 years. Out of 93 diabetic patients, fifty-five patients had diabetes of less than 10-year duration and the mean central corneal thickness of these patients was 560.67±7.85µm. Thirty-eight patients had diabetes of more than or equal to 10 years and the mean CCT of these patients was 565.55±11.74µm and the difference between them was statistically significant (P=0.02) using unpaired t-test (Figure 8). The mean CCT between male and female were comparable to each other and no statistical difference was observed (p=0.93, Figure 9).
Diabetic patients (Type 1 and type 2 DM) with or without retinopathy were divided into 3 sub groups
-
Subgroup 1 -: Having no diabetic retinopathy
-
Subgroup 2 -: Having any grade of non-proliferative diabetic retinopathy
-
Subgroup 3 -: Having proliferative diabetic retinopathy.
The mean CCT of the sub-group-2 (563.81±9.12.32µm) was greater than sub-group-1 (558.71±7.67µm) and the difference was not statistically significant (p >0.05) Also, the mean CCT of the sub-group-2 (563.81±12.32µm) was greater than sub-group-3 (563.43±9.70µm) and the difference was not statistically significant (p >0.05). The mean CCT of sub-group-3 (563.43±9.70µm) was greater than sub-group-1 (558.71±7.67µm) and the difference was not statistically significant (p >0.05) using one way ANOVA.
DISCUSSION
Diabetes is one of the world’s largest public health problems. The measurement of central corneal thickness has become a very important ocular parameter due to its importance as an indicator of corneal health status and decisions involving refractive surgeries and estimation of Intraocular Pressure. In glaucoma patients, central corneal thickness measurement is important to determine the true intraocular pressure which may be overestimated in diabetic patients with glaucoma due to increased CCT.
In the present study, the mean age of diabetics and non-diabetic controls was comparable and no statistical difference was found between them (p=0.227). Concerning the mean age of our diabetic patients (55.45±10.79 years), this was similar to Lee et al.14 (57.5±8.5years) and Ozdamar et al.15 (57.3±4.7 years), and contrast to Busted et al.16 (34 years).
The mean CCT between male and female were comparable to each other (Male=539±26.40 and female=539.60±27.96, p=0.92). Our findings were similar to Storr-Paulsen et al..17 They observed mean central corneal thickness were comparable in both the sex (p=0.27).
Most studies like the present cross-sectional study show that the diabetic eye had an increase in CCT (563.11±11.40µm) as compared to non-diabetic controls. (529.53±17.91µm). This difference was statistically significant (p<0.0001). Busted et al.16 and Lee et al.14 reported that the mean CCT of diabetic patients was significantly (p<0.005) thicker than non-diabetic controls in a sample size of 81 insulin-dependent juvenile-onset diabetics and concluded that increased CCT could be due to increased hydration of cornea and endothelial dysfunction. Lee et al.14 and Yasemin Ozdamar et al.15also drawn similar observations. However, in contrast to our study Larsson et al.18 and Schultz et al.19 did not find any increase in CCT in Type1 and Type 2 DM patients when compared to non-diabetic controls. They measured CCT with the specular microscope: therefore, the difference between these studies could be the measuring method. The corneal thickness of diabetic patients increases because the corneal endothelium pump deteriorates due to the reduction of Na+/K+ ATPase activity which in turn causes an increase in stromal hydration and morphological and permeability changes in the cornea.14,16,18
The study by Sahin A20 suggests glaucore can act as a collagen cross-linking agent with the help of advanced glycosylation end products. Increased formation of covalent cross-linking bonds in the corneal stroma may lead to increased corneal thickening and biochemical changes.
In the present study, we found that the mean CCT in subgroups of diabetic retinopathy were comparable, having mean CCT in subgroup 1, 2, and 3 was 558.71±7.67µm, 563.81±9.12.32µm, and 563.43±9.70µm respectively. The difference between them was not statistically significant (p>0.05) using one way ANOVA. A similar conclusion was also drawn by Toygaro et al.20 and Solani D et al. 21
About hyperglycaemia assessed by glycosylated haemoglobin (HbA1C). In the present study, diabetic patients who had HbA1C level ≥7% has thicker mean CCT (565.65±9.94µm) as compared to those diabetic patients who had HbA1c level <7% (559.03±8.32µm) and this difference was statistically significant (p=0.026) using unpaired t-test. Similar conclusions were drawn by Prempal Kaur et al.22 and Mehmet Ozgur ZENZIN et al.23 In contrast to our study, Larsson et al.18 and Brownlee M et al.24 did not found any correlation between HbA1C and CCT.
In the current study, we divided the diabetic patients according to the duration of diabetes into two groups, one with the duration of diabetes less than 10 years and the other had those with duration of diabetes more than or equal to 10 years. The mean CCT in patients with diabetes ≥10 years was thicker than those of less than 10 years duration (565.67±11.74µm v/s 560±7.85µm) and the difference between them was statistically significant (p=0.02).
A similar conclusion was drawn by Lee et al. and Ruchi Dabas et al.25 In contrast to our study, Mehmet Ozgur et al.24 by using Orbscan II topography system measured CCT and found thicker mean CCT in patients who had diabetes of more than or equal to 10 years (565.78±39µm) as compared to those who had diabetes of fewer than 10 years (561.45±36.20 µm) but the difference was not statistically significant (p=0.522). The possible difference may be due to the application of different measuring method of CCT. Busted et al.16 also reported no significant relationship between the central corneal thickness of diabetes and the diabetic duration. This difference is probably because the mean age of their subjects (34 years) was lower than that (55.±10.79 years) of our diabetic subjects. The possible explanation of thicker cornea in those who had more than 10 year of diabetes compared to less than 10-year duration is that as the duration of diabetes increases, there is a decrease in the ability of corneal endothelial pump to compensate for excess turnover of corneal hydration.
In the present study, we compared mean central corneal thickness amongst Type 1 and Type 2 DM patients. There were four patients of Type 1 DM and their mean age was 39.5±9.29 years with mean duration of diabetes were 13.75±12.28 years, while in Type 2 diabetic group mean age and mean duration of diabetes was 55.631 ±10.789 and 8.817±5.49 years respectively.
The mean values were comparable in type 1 and type 2DM patients (562±12.9035µm and 562.593±9.43552µm respectively) and the difference was not statistically significant (p=0.90).
A similar conclusion was drawn by Schultz et al.19 who found mean CCT was comparable in both Type 1 (540µm) and Type 2 DM patients (530-540µm). Larsson et al.18 also observed similar result with no significant difference in mean CCT values when they were compared between Type 1 and Type 2 DM patients. Yasser et al.26, in their cross-sectional study on 160 subjects from different age groups were studied. They compared mean CCT in 42 patients of Type 1 and 38 Patients of type 2 DM and observed no significant difference (p=0.77).
CONCLUSION
The present study suggests that diabetes mellitus patients show thick cornea as one of the unnoticed indicators of duration of disease and level of hyperglycemia. Thus consideration of the corneal thickness in patients of DM is very important for obtaining accurate IOP measurement and planning and performing refractive surgery.
ACKNOWLEDGEMENTS: Authors acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
CONFLICT OF INTEREST- NIL
SOURCE OF FUNDING- NIL
References:
-
Singleton JR, Smith AG, Russell JW, Fledman EL. Microvascular complications of impaired glucose tolerance. Diabetes 2003;52:2867-2873.
-
Rother K. Diabetes Treatment - Bridging the Divide. NEJM 2007;356:1499-1501.
-
Lutty GA. Effects of diabetes on the eye. Invest Ophth Vis Sci 2013; 54:81-87.
-
Price FW Jr, Koller DL, Price MO. Central corneal pachymetry in patients undergoing laser in situ keratomileuses. Ophthalmology 1999;106:2216–2220.
-
Ginter E, Simko V. Global prevalence and future of diabetes mellitus. Adv Exp Med Biol 2012;771:35-41.
-
Abdullah N, Attia J, Oldmeadow C. The architecture of risk for type 2 diabetes: understanding Asia in the context of global findings. Int J End 2014;2014:593982.
-
Al Houssien AO, Al Houssien RO, Al-Hawass A. Magnitude of diabetes and hypertension among patients with Dry Eye Syndrome at a tertiary hospital of Riyadh, Saudi Arabia - a case series. Sau J Ophth 2017;31(2):91-94.
-
Sayin N, Kara N, Pekel G. Ocular complications of diabetes mellitus. World J Diabetes 2015;6(1):92-108.
-
Taylor-Phillips S, Mistry H, Leslie. Extending the diabetic retinopathy screening interval beyond 1 year: a systematic review. Bri J Ophth 2016;100(1):105-114.
-
Weston BC, Bourne WM, Polse KA, Hodge DO. Corneal hydration control in diabetes mellitus. Invest Ophthalmol Vis Sci 1995;36:586–595.
-
Saini JS, Mittal S. In vivo assessment of corneal endothelial function in diabetes mellitus. Arch Ophth 1996;114:649–665.
-
Roszkowska AM, Tringali CG, Colosi P, Squeri CA, Ferreri G. Corneal endothelium evaluation in type I and type II diabetes mellitus. Ophthalmology 1999;213:258-261.
-
Akinci A, Bulus D, Aycan Z, Oner O. Central corneal thickness in children with diabetes. J Refract Surg 2009;25:1041-1044.
-
Lee JS, Oum BS, Choi HY, Lee JE, Cho BM. Differences in corneal thickness and corneal endothelium related to duration in diabetes. Eye 2006;20:315–318.
-
Ozdamar Y, Cankaya B, Ozalp S, Acaroglu G, Karakaya J, Ozkan SS. Is there a correlation between diabetes mellitus and central corneal thickness. J Glaucoma 2010;19:613-616
-
N Busted T Olsen O Schmitz, Clinical observations on the corneal thickness and the corneal endothelium in diabetes mellitus, Br J Ophthalmol. 1981;65:687-90.
-
Storr-Paulsen A, Singh A, Jeppesen H, Norregaard JC, Thulesen J.Corneal endothelial morphology and central thickness in patients with type II diabetes mellitus. Acta Ophthalmol 2014;92:158-160.
-
Larsson LI, Bourne WM, Pach JM, Brubaker RF. Structure and function of the corneal endothelium in diabetes mellitus type I and type II. Arch Ophthalmol 1996;114:9-14
-
Schultz RO, Matsuda M, Yee RW. Corneal endothelial changes in type 1 and type 2. Diabetes mellitus. Am J Ophthalmol 1984;98:401-410
-
Sahin, A. Bayer G. ?Ozge A, Mumcuo T . Corneal biomechanical changes in diabetes mellitus and their influence on intraocular pressure measurements. Investig Ophth Vis Sci 2009;50(10):4597–4604.
-
Toygar O, Sizmaz S, Pelit A, Toygar B, Yaba? Kizilo?lu Ö, Akova Y.. Central corneal thickness in type II diabetes mellitus: is it related to the severity of diabetic retinopathy? Turk J Med Sci 2015;45:651-654.
-
Solani D. Mathebula, Tshegofatso M. Segoti. Is the central corneal thickness of diabetic patients thicker than that of non-diabetic eyes? Afri Vis Eye Health 2015;74:1-5.
-
Prempal Kaur, Baljinderpal Singh, Bhavkaran Singh Bal, Inderjit Kaur, Vishal Brar. Central Corneal Thickness in Type 2 Diabetic Patients and its Correlation with Duration, Hba1c Levels And Severity of Retinopathy. J Den Med Sci 2016;15:91-4.
-
Zengin MO, Ozbek Z, Arikan G, Durak I, Saatci SA. Does central corneal thickness correlate with haemoglobin A1c level and disease severity in diabetes type II? Turk J Med Sci 2010;40:675-680.
-
Brownlee M. The path biology of diabetic complications. Diabetes 2005;54:1615–1625.
-
Dabas R, Sethi S, Garg M, Aggarwal R, Lamba S, Bhattacharjee A, et al. Central Corneal Thickness (CCT) in Diabetic Subjects and its Correlation with Disease Duration and Severity. Ann Int Med Den Res 2017;3:4-6.
-
Abdulghani YS, Ali TO. Correlation between central corneal thickness and diabetes in Sudanese patients. Nat J Med Res 2013;3:309-311.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





