IJCRR - 7(24), December, 2015
Pages: 01-05
Date of Publication: 20-Dec-2015
Print Article
Download XML Download PDF
A STUDY OF MORPHOLOGY OF THE PROXIMAL PART OF VENTRAL BRANCHES OF ABDOMINAL AORTA IN CADAVERS
Author: Kruti Bharatkumar Tapiyawala, M. Natarajan
Category: Healthcare
Abstract:Objective: Majority of studies in the past about ventral branches of abdominal aorta mainly focused on the branching pattern.
The cadaveric data on the vertebral level of origin of the ventral branches of abdominal aorta is less. Hence the study aimed at
the morphology of proximal part of ventral branches of abdominal aorta.
Objectives:
1. To determine the vertebral level of origin of coeliac trunk
2. To determine the vertebral level of origin of superior mesenteric artery
3. To determine the vertebral level of origin of inferior mesenteric artery
Materials and Methods: Fifty embalmed cadavers were dissected. The vertebral level of origin of ventral branches were determined
and variations were noted.
Results:
1. In 38% cases, the vertebral level of origin of coeliac trunk was found to be located at the level of intervertebral disc (IVD)
T12-L1.
2. In 24% cases, the vertebral level of origin of superior mesenteric artery was found to be located at the level of intervertebral
disc (IVD) T12-L1 and upper 1/3rd of L1.
3. In 22% cases, the vertebral level of origin of inferior mesenteric artery was found to be located at the level of intervertebral
disc (IVD) L3-L4.
Conclusion: In conclusion, the present study provides a comprehensive data about the abdominal aorta and the proximal part
of its ventral branches which will help in interpretation of radiographs and during surgery of different types of abdominal pathology
in Indian population. Awareness of these variations can prevent potential intra-operative and post- operative complications.
Keywords: Ventral branches, Coeliac trunk, Superior mesenteric artery, Inferior mesenteric artery
Full Text:
INTRODUCTION
Anatomical variations involving the visceral arteries are common. Though variations in coeliac trunk are usually asymptomatic, they may become important in patients undergoing diagnostic angiography for gastrointestinal bleeding or prior to an operative procedure. Close relation of short coeliacomesenteric trunk with median arcuate ligament and the tight tendinous ring around the aortic opening can cause compression of the trunk. This may lead to postprandial periumbilical pain. Surgical intervention in such a case may be associated with the risk of ligating the wrong vessel or severing an essential organ sustaining artery, danger of ischaemia, gangrene, leakage and bleeding from the site of repair.1 Prior knowledge of aortic variations is required to successfully accomplish aortic replacement with implantation of the coeliac trunk, mesenteric arteries and renal arteries.2 In the radiation therapy of upper gastrointestinal malignancies, treatment of lymph nodes in the region of the coeliac axis and superior mesenteric axis is often mandated.3
Evaluation of arteries branching from the abdominal aortathe level of their divergence, presence of atypical variants of a common origin of arteries plays an important role in the diagnostics of many abdominal disorders.4 Variations in morphology of the aorta and its branches are of considerable interest as vessel geometry not only determines flow dynamics, but is also crucial in the pathogenesis of vascular diseases, e.g., atherosclerosis and aneurysm formation.5 Anatomic variants of the coeliac trunk is essential to successfully accomplish surgical, oncologic, or interventional procedures including lymphadenectomy around hepato-splenomesenteric trunk, aortic replacement with reimplantation of the trunk, or chemoembolization of liver malignancies, all of which can potentially create significant morbidity because of the large visceral territory supplied by a single vessel.6
MATERIALS AND METHODS:
Fifty formalin-fixed cadavers in the department of anatomy were used for the study. This study was conducted over a period of two years. All the cadavers were ranging between the age group of 18-65 years at the time of death. None of the abdomen showed any evidence of previous surgery. After meticulous dissection satisfactory exposure of the ventral branches of abdominal aorta was done. Counting of vertebra was done from below upward, by identifying the sacral promontory first and labelling the vertebra immediately above that as fifth lumbar vertebra (L5) and so on and so forth. This counting of vertebra was also confirmed by identifying the 12th rib and tracing it to the 12th vertebra. Length of each vertebral body was measured. Each vertebra was divided into upper, middle and lower third. The study protocol was prepared in the form of a proforma. The parameters determined were:
1. To determine the vertebral level of origin of coeliac trunk
2. To determine the vertebral level of origin of superior mesenteric artery
3. To determine the vertebral level of origin of inferior mesenteric artery Any variation in the site of origin of the ventral branches were also observed.
RESULTS
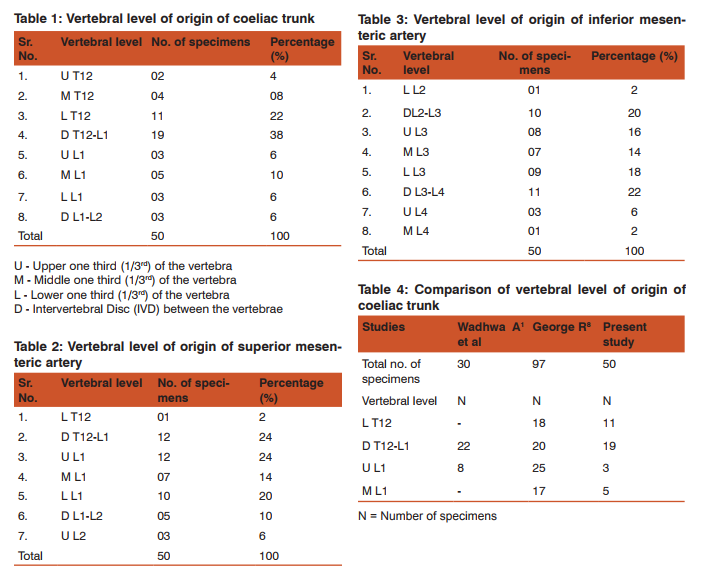
VERTEBRAL LEVEL OF ORIGIN OF COELIAC TRUNK (Table-1)
The vertebral level of origin of coeliac trunk was found to be located between upper 1/3rd of T12 to IVD L1-L2. In 19 cases, it was located at the level of IVD T12-L1.
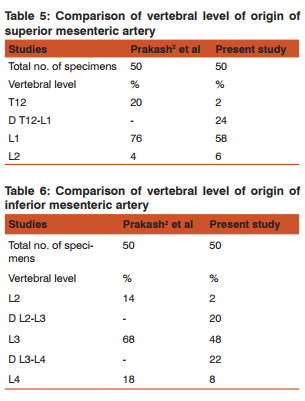
VERTEBRAL LEVEL OF ORIGIN OF SUPERIOR MESENTERIC ARTERY (Table-2)
The vertebral level of origin of superior mesenteric artery was found to be located between lower 1/3rd of T12 to upper 1/3rd of L2. In 12 cases, it was located at the level of IVD T12-L1 and upper 1/3rd of L1.
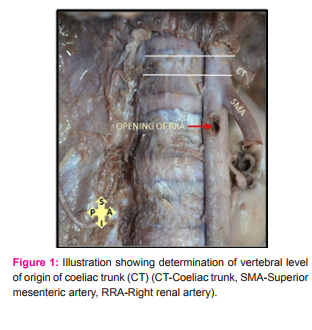
VERTEBRAL LEVEL OF ORIGIN OF INFERIOR MESENTERIC ARTERY (Table-3)
The vertebral level of origin of inferior mesenteric artery was found to be located between lower 1/3rd of L2 to middle 1/3rd of L4. In 11 cases, it was located at the level of IVD L3-L4
DISCUSSION
1. VERTEBRAL LEVEL OF ORIGIN OF COELIAC TRUNK (Table-4)
Pant P7 et al in 2013 dissected 40 cadavers and found that in maximum number of cases i.e. 76.68%, coeliac trunk originated between T12 and L1 vertebra. In 23.04% cases, it originated at the upper 1/3rd of L1 vertebra and in minimum number of cases i.e.5.12% cases, it originated at the level of lower 1/3rd of T12 vertebra. They also noticed absence of coeliac trunk in 2.5% of cases, where branches of coeliac trunk directly originated from aorta. Wadhwa A1 et al in 2011 dissected 30 adult cadavers and found that the coeliac trunk was arising at the level of IVD T12-L1 in 22 cases (73.3%) and upper 1/3rd of L1 vertebra in 8 cases (26.6%). George R8 in 1934 observed the vertebral level of origin of coeliac trunk in 97 cadavers. The author has measured the vertebral levels of origin of the unpaired visceral branches at the center of origin of the each branch. The author found that the coeliac trunk was arising at the level of upper 1/3rd of L1 in 25 cases, at the level of IVD between T12-L1 in 20 cases, at the level of lower 1/3rd of T12 in 18 cases and at the level of middle 1/3rd of L1 in 17 cases. Prakash2 et al in 2011 dissected 50 cadavers found that the coeliac trunk was located most commonly (in 64% of cadavers) at the level of T12. In 36% cases, the coeliac trunk was located at the level of L1. In the present study, the vertebral level of origin of coeliac trunk was at the level of IVD T12-L1 in 38% cases, at the level of T12 in 34% cases and at the level of L1 in 22% cases 2.
VERTEBRAL LEVEL OF ORIGIN OF SUPERIOR MESENTERIC ARTERY (Table-5)
George R8 in 1934 observed the vertebral level of origin of superior mesenteric artery in 97 cadavers. The author found that the superior mesenteric artery was arising at the level of lower 1/3rd of L1 in 29 cases, at the level of IVD between L1- L2 in 21 cases at the level of middle 1/3rd of L1 in 20 cases, at the level of upper 1/3rd of L1 in 17 cases. Prakash2 et al found the vertebral level of origin of superior mesenteric artery at the level of L1 in 76% cases, at the level of T12 in 20% cases. In the present study, the vertebral level of origin of superior mesenteric was found at the level of IVD T12-L1 in 12 cases, at the level of upper 1/3rd of L1 in 12 cases, at the level of lower 1/3rd of L1 in 10 cases, at the level of middle 1/3rd L1 in 7 cases. In 58% cases, it was located the level of L1 and in 24% cases, it was located at the level of IVD T12-L1. 3.
VERTEBRAL LEVEL OF ORIGIN OF INFERIOR MESENTERIC ARTERY (Table-6)
George R8 in 1934 observed the vertebral level of origin of inferior mesenteric artery in 97 cadavers. The author found that the inferior mesenteric artery was arising at the level of middle 1/3rd of L3 in 28 cases, at the level of lower 1/3rd of L3 in 23 cases, at the level of upper 1/3rd of L3 in 20 cases, at the level of IVD between L2-L3 in 15 cases and at the level of IVD L3-L4 in 14 cases. Prakash2 et al found that the vertebral level of origin of inferior mesenteric artery was at the level of L3 in 68% cases, at the level of L4 in 18% cases and at the level of L2 in 14% cases. In the present study, the vertebral level of origin of inferior mesenteric artery was located at the level of IVD L3-L4 in 11 cases, at the level of IVD L2-L3 in 10 cases, at the level of lower 1/3rd of L3 in 9 cases, at the level of upper 1/3rd of L3 in 8 cases and at the level of middle 1/3rdof L3 in 7 cases. In 48% cases, it was located at the level of L3 and in 22% cases, it was located at the level of IVD L3-L4. Probable embryological basis for the different vertebral levels of ventral branches: The ventral splanchnic arteries are originally paired vessels distributed to the capillary plexus in the wall of the yolk sac. After fusion of the dorsal aortae, they merge as unpaired trunks that are distributed to the increasingly defined and lengthening primitive digestive tube. Longitudinal anastomotic channels connect these branches along the dorsal and ventral aspects of the tube, forming dorsal and ventral splanchnic anastomoses. These vessels obviate the need for so many ‘subdiaphragmatic’ ventral splanchnic arteries, and these are reduced to three, the coeliac trunk and the superior and inferior mesenteric arteries. As the viscera supplied descend into the abdomen, their origins migrate caudally by differential growth: the origin of the coeliac artery is transferred from the level of the seventh cervical segment to the level of the 12th thoracic; the superior mesenteric from the second thoracic to the first lumbar; and the inferior mesenteric from the twelfth thoracic to the third lumbar.9 The yolk sac is supplied by a number of paired vessels called omphalomesenteric or vitelline arteries at the end of the fourth week of intrauterine life. The aforementioned vessels gradually fuse in the latter part of the embryonic life and in the dorsal mesentery of the gut they form arteries which in adult life are represented as the coeliac, superior mesenteric, and inferior mesenteric arteries. Defective fusion of the omphalomesenteric arteries during the embryonic stage can be important factor manifesting the variations.2
CONCLUSION
In conclusion, the present study provides a comprehensive data about the abdominal aorta and the proximal part of its ventral branches which will help in interpretation of radiographs and during surgery of different types of abdominal pathology in Indian population. Awareness of these variations can prevent potential intraoperative and post- operative complications.
ACKNOWLEDGEMENTS:
The authors wish to convey her sincere thanks to Dean, Seth G. S. Medical College and K.E.M. Hospital, Mumbai and all staff members from Department of Anatomy, Seth G. S. Medical College, Mumbai. Authors also acknowledge the immense help received from the scholars whose articles are cited and included in references of this manuscript. The authors are also grateful to authors/ editors/ publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.
References:
1. Wadhwa A, Soni S. A composite study of coeliac trunk in 30 adult human cadavers - its clinical implications. Global Journal of Medical research. 2011; 11(1): 34-38.
2. Prakash, Mokhasi V, Rajini T, Shashirekha M. The abdominal aorta and its branches: anatomical variations and clinical implications. Folia Morphol. 2011; 70(4):282-286.
3. Kao GD, Whittington R, Coia L. Anatomy of the coeliac axis and superior mesenteric artery and its significance in radiation therapy. Int J RadiatOncolBiol Phys. 1993; 25(1):131-134.
4. Kornafel O, Baran B, Pawlikowska I, Laszczy?ski P, Guzi?ski M, S?siadek M. Analysis of anatomical variations of the main arteries branching from the abdominal aorta, with 64-detector computed tomography. Polish Journal of Radiology. 2010; 75(2): 38-45.
5. Pennington N, Soames RW. The anterior visceral branches of the abdominal aorta and their relationship to the renal arteries. Surg and Radiol Anat. 2005; 27: 395-403.
6. Sawant S, Kolekar S, Harichandana N. Anatomical Variations in coeliac Trunk and its branches. International Journal of Recent Trends in Science And Technology. 2013; 6(3), 130-133.
7. Pant P, Mukhia R, HarithaKumari N, Mukherjee A. Variant anatomy of the coeliac trunk and its branches. Global Research Analysis. 2013; 2(6), 179-180.
8. George R. Topography of the unpaired visceral branches of the abdominal aorta. Journal of Anatomy. 1934; 69:196-205.
9. Standring S. Embryonic arteries. In Collins P, editor. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 40th ed. Edinburgh, Churchill Livingstone; 2008: 206-207.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





