IJCRR - 13(8), April, 2021
Pages: 48-53
Date of Publication: 25-Apr-2021
Print Article
Download XML Download PDF
Adjunct Effect of Kinesiotaping on Adhesive Capsulities of Shoulder Joint
Author: Neha Deshmukh, Milind Kahile, Neha Chaudhary, Shweta Panchbhudhe, Vasant Gawande
Category: Healthcare
Abstract:ntroduction: The term adhesive capsulitis of the shoulder, frozen shoulder and Periarthritis shoulder have been used for pa�tients with shoulder pain and mobility deficits. Adhesive Capsulitis is a painful condition of the shoulder that is associated with the loss of Range of Motion of the Glenohumeral joint. The painful restriction of the glenohumeral joint may be active or passive or both. All the sign and symptoms of adhesive capsulitis lead to functional loss in an individual. Various treatment strategies have been proposed to compensate for the functional loss caused due to painful restriction of the affected upper extremities. Kinesiotaping is also a proven therapy to cope with the loss, thus this study aims to find the adjunct effect of kinesiotaping on painful restriction finally affecting the functions. Methodology: A Randomized control trial on 30 diagnosed case of adhesive capsulitis was carried out to find the adjunct effect of KT along with end range mobilization and movement with mobilization technique. The 6-week protocol was implemented on both the groups where an alternated session of treatment was given. Data was collected and was statistically analyzed. Result: The collected data were analyzed using one way repeated measure ANOVA to compare the outcome measures at 3 different time point and Wilcoxon Rank Sum test to compare the mean of outcome measures over the period where pain and functional shows a significant improvement in the initial treatment sessions. Conclusion: KT shows an adjunct effect on pain, range of motion and function when used along with mobilization techniques in patients with adhesive capsulitis of the shoulder joint.
Keywords: Adhesive Capsulitis, Kinesio Taping, End range mobilization, Movement with mobilization
Full Text:
Introduction
The shoulder is a unique anatomical structure with an extraordinary range of motion that allows us to interact with our environment A loss of mobility of this joint will cause significant morbidity. Adhesive capsulitis is a poorly understood musculoskeletal condition that can be disabling both physically and mentally. Although adhesive capsulitis of the shoulder is a self-limiting disorder that resolves in 1-3 years, some studies report range between 20% and 50% of patient with adhesive capsulitis suffers long term ROM deficits that may last up to 10 years1. Current findings report that patients presenting with shoulder dysfunction have an approximately 50 this opportunity of being diabetic. By understanding the knowledge of the high prevalence of shoulder dysfunction among people with diabetes will urge clinical practitioner to screen patients with shoulder pain for diabetes. Early diagnosis and prompt management of diabetes are understood to scale back the danger of musculoskeletal complications. Monitoring for signs of musculoskeletal complications is often a useful component of comprehensive diabetes care. Alarming high prevalence of shoulder dysfunction and the other way around will alert the clinical practitioners for early detection and management to realize better shoulder function. Diabetic care programs must include screening, prevention, ketoacidosis, foot ulcer, pancreatitis and rehabilitation strategies for shoulder dysfunction.2-5 There are various measures to manage the adhesive capsulitis of the shoulder joint such as Steroid injection with or without physical therapy, Physical therapy with interscalene block or local anaesthesia, distension arthrography, closed manipulation arthroscopic release or open release.6,7 But limited researchers are available to support the use of the above treatment. Kinesio taping is gaining popularity these days due to its comfort provided in functional activities. KT was designed to mimic the qualities of human skin. It has roughly the same thickness as the epidermis and can be stretched between 30% - 40% of its resting length longitudinally. KT is considered a safe technique that has minimal side effects, which may facilitate musculoskeletal rehabilitation by reducing the discomfort. It is a unique and non-invasive approach for the treatment of musculoskeletal injuries. KT will assist the body to returns to normal function through its application onto the skin. The primary effect of tape application is usually superficial. The success of KT depends on two factors, firstly the proper evaluation of the patient’s condition and, the proper application of the KT technique. When these two factors are combined, an effective treatment modality can be achieved. Kase et al have proposed several benefits of the application of Kinesio tape. The application of KT provides positional stimulus through the skin, align fascial tissues, create more space by lifting fascia and soft tissue above the area of pain/inflammation, and provides sensory stimulation to assist or limit motion. It also assists in the removal of oedema by directing exudates toward the lymph duct8. There is no high-level evidence to support or refute many of the commonly used treatments for adhesive capsulitis of the shoulder joint. And also there is less evidence to prove the beneficial effect of various treatment regimes on pain and ROM in adhesive capsulitis of the shoulder joint with a combination of the treatment strategies. The use of any treatment regimen alone is limited in the adhesive capsulitis of the shoulder joint. Hence this condition is always treated with a combination of treatment strategies. Also, there is little information available from randomized clinical trials to support the use of a combination of the mobilization techniques and other approaches like KT for treating the adhesive capsulitis of the shoulder joint. The use of KT in treating shoulder impingement was well studied. But there is paucity of recommending the use of KT in treating the adhesive capsulities of the shoulder joint. Adhesive capsulities of shoulder joint have proven adverse effect on person’s quality of life. Although AC affects the physical function of an individual, there are various studies showing its impact on the mental status.6,7,8 Researchers have found that the mental function of subjects with adhesive capsulitis was lower when compared to age-matched controls. The adding effects of physical and mental status adversely affect the quality of life. The scale used in the present study to calculate the effect of adhesive capsulitis on the functional status of the patient is widely considered as a valid measure to observe pain relief, passive motion, and patient’s satisfaction. UCLA [University of California- Los Angeles] scale is precise to effectively follow the progress of individual patients in the clinic setting. Despite its frequent use in research, no studies have evaluated either the reliability or the validity of measurement obtained with the shoulder scale9. Studies also revealed that the UCLA score shows more favourable results when compared with other scales. The salient feature of UCLA is; it is relatively easy to complete and also have objective measures10. Thus in the present study, we aim to find out the effect of Kinesio taping on the function of the individuals diagnosed with adhesive capsulitis of the shoulder joint.
Need for Study:
The hallmark of adhesive capsulitis of the shoulder is a global decreased in ROM and shoulder pain. The pain is often described as a poorly localized and deep ache. The pain may radiate proximally or distally from the shoulder joint and also can radiate towards the scapular distally from the shoulder joint and also can radiate towards the scapular and interscapular region. Weakness is often related to pain or concomitant tendinopathy. All these symptoms lead to hampered and restricted daily activities. This certainly indicates that shoulder dysfunction directly impacts the person's quality of life.
Objective:
To determine the effect of Kinesio taping on pain and function in adhesive capsulitis of shoulder joint.
Procedure:
The ethical clearance was obtained to conduct a randomized control trial on 30 individuals diagnosed with adhesive capsulitis of the shoulder joint from the institutional ethical committee. The institutional physiotherapy OPD was targeted to obtain the individuals for carrying out the study. Simple random sampling by using the lottery method was used to group the individuals. Dependent variables were pain and functions, were as mobilization and Kinesio taping technique were the independent variables. Both genders with age between 40-65yrs were included and history of any shoulder surgery before 12 weeks, healing/ unhealed fracture around the shoulder girdle, healing/ unhealed soft tissue injury around shoulder girdle and presence of malignancy or any infective condition around shoulder girdle were excluded.11
15 individuals in the first group were treated with the mobilization technique.ERM:10-15 repetition of Grade IV mobilization11, MWM: 3 sets of 10 repetitions, with 1 min rest between sets12. The remaining 15 were given Kinesio taping to check the adjunct effect along with mobilization techniques.
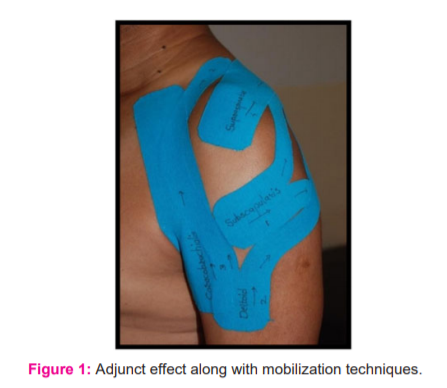
Intervention Duration was 6weeks (3 sessions per week) and the result in a change of function on the UCLA scale was observed during the period and also over the period ( Figure 1).
Results:
A total of 30 subjects with a diagnosis of stage II or III adhesive capsulitis of the shoulder joint were recruited for the study to find the additional effect of Kinesio taping along with ERM and MWM. For the statistical test p < 0.05 was considered as statistically significant. Statistical software STATA version 10.0 was used for statistical analysis. Out of the total 30 subjects, 19 were female and 11 were male. The mean age in group A was 51.13±7.03 and for the group, B was 53.4±5.81 years. In the current study, the continuous variables were pain on VAS, functional score on the UCLA scale. The mean score of these variables was assessed at 3 different time interval, on Day 1, after 3 weeks and after 6weeks of intervention. Both the groups showed a highly significant reduction in pain score when compared at different time interval i.e. after 3rd weeks and after 6th weeks of intervention by using one way repeated measure ANOVA. In Group A at end of the 3rd week, the pain score was 5.26±1.22 and for Group B the pain score was 4.13±1.06. And at the end of the 6th week the pain score in group A was 3.8±1.14 and in Group B was 3.06±0.88. Comparison of pain was done between Group A and Group B over the period by using the Wilcoxon Rank Sum test. After 3 weeks of intervention, the reduction was highly significant in Group B compared to Group A.
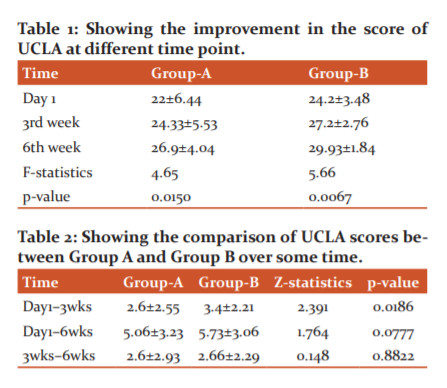
Over day 1 to 3 weeks of intervention the average difference in the pain score of Group A was 1.06±1.04 and Group B was 2.26±1.16. Over day 1 to 6 week’s period, the average difference in the pain score of Group A was 2.53±1.35 and in Group B was 3.33±1.11. And over 3 weeks to 6 weeks period the average difference in pain score of Group A was 1.06±0.73 and Group B was 1.46±1.24. Improvement in functions was also significant with the UCLA score at the different period ( Table 1 and 2).
Discussion:
The purpose of this randomized controlled trial was to know functional activity improvements and efficacy of the Kinesio taping as an adjunct to movement with mobilization and end range mobilization in adhesive capsulitis of the shoulder joint in reducing pain, improving range of motion and the shoulder functional activity.
Diagnosed cases of adhesive capsulitis are associated with painful movement and functional deficit and physical therapy is often the first choice for conservative management. In terms of improving shoulder mobility, the evidence suggests that patient receiving the manual therapy intervention for adhesive capsulitis demonstrated improvement.13
Various physical therapy approaches have been suggested for shoulder musculoskeletal disorder like impingement syndrome, adhesive capsulitis, and rotator cuff injury. This includes manual therapy, electrotherapy, acupuncture, and exercise therapy.
Several disease-specific systematic reviews examining the efficacy of physical therapy negate the effect of electrotherapeutic modalities and support the utilization of manual therapy and exercises13.
Manual therapy mainly emphasizes the use of various kind of mobilization techniques in regaining the range of motion and reducing pain thus improving the functional activity in subjects with adhesive capsulitis of the shoulder joint 14,15.
Both the genders were included in the study and most of the subjects reported with symptoms were in the age group of 50-59 years. A total of 30 subjects were evaluated and treated with a diagnosis of adhesive capsulitis of the shoulder joint.
After the data collection, it was found that the numbers of the female subject were more than their counterparts. The female: male ratio in both groups was 3:1. A sample survey done by various researchers had found that the incidence of adhesive capsulitis is common in females than in males16.
A Majority 70% of the subjects included in the study had dominant shoulder involvement. Overuse of the shoulder is one of the predisposing factors for tendinitis which can progress to adhesive capsulitis.
The current study also shows a significant relationship between diabetes mellitus and the occurrence of adhesive capsulitis of the shoulder joint. In the study, 56.6%subjects were diagnosed with cases of diabetes mellitus. The finding of the present study can be correlated by the study done by Milgrom et al. who found that 29.3% of subjects diagnosed with adhesive capsulitis had Diabetes mellitus.17
In the present randomized controlled trial Group A was treated with End range mobilization (ERM) and Movement with mobilization (MWM). To achieve the primary goal, Group B was given KT in addition to ERM and MWM. At the end of the intervention protocol, both the groups were statistically analyzed.
As the pain was the major complaint of the subjects, pain evaluation at the end of the 6th week showed a significant reduction in both the groups (p< 0.0001) as compared to pre-intervention pain assessment. The reduction of pain was uniform from 0-3 weeks and 3-6 weeks in Group A. Group B showed a sudden reduction in pain in the initial 3 weeks of application of KT as an adjunct to ERM and MWM. Further rate of reduction was gradual which was similar to the reduction in Group A during the 3-6 weeks of intervention. When both groups were compared over the period, Group B showed a significant reduction of pain in the initial 3 weeks of intervention than in Group A and a non-significant difference in pain during later 3-6 weeks of intervention. This reduction of pain in Group B can be attributed to the application of KT.
The effect provided by KT is due to the modulation of pain via pain gate control theory. It has been proposed that KT stimulate the neuromuscular pathway via increased afferent feedback. Under the gate control theory, an increase in afferent stimulus through large-diameter nerve fibres can serve to mitigate the input received from small-diameter nerve fibres conducting nociception6.
In this study, the basic muscle techniques that are inserted to origin was used along with a mechanical correction. Mechanical correction is positional. It does not attempt to keep the tissue or joint in a fixed position. It provides a stimulus perceived by the mechanoreceptor and is used to assist in positioning the muscles, fascial tissue or joint to stimulate the senses. This results in the body’s adaptation to the stimulus. Mechanical correction via KT can also be used as functional support without losing the AROM.18
The studies conducted by Djordjevic and Kamat et al.19 also showed a significant reduction in pain and improvement in ROM with combined MWM and KT. They also discussed that the effects of MWM can be maintained further via taping and self MWM, which may further enhance its potential long-lasting effect. It was also stated that taping can help in maintaining joint position and can increase proprioceptive awareness.
As the original idea of MWM techniques, that is, correcting the positional fault in the malaligned painful joint. The application of KT can sustain the corrected joint position for a longer time.19,20
Another outcome measure in the present study was AROM and PROM. Both the groups showed improvement in the ROM. Group B showed marginally greater improvement, but it was not a statistically significant improvement in an intragroup comparison over the period. Marginal improvement in Group B can be attributed to the relief of pain provided by KT. As proposed by Kaya et al. KT provides continuous pain gating and proprioceptive awareness that improves motor recruitment.21 KT also guides the shoulder through an arc of improved glenohumeral motion, which reduces mechanical irritation of the involved soft tissue structures thus improving both active and passive ROM.
The reduction of pain and improvement in AROM and PROM in both the groups were also ascribed to ERM and MWM.
ERM is the small amplitude rhythmic oscillatory movement given to the joint at its end range. These small amplitude oscillatory movements are used to stimulate the mechanoreceptor that may inhibit the transmission of the nociceptive stimuli at the spinal cord or brain stem level11,21.
This study can be correlated with the research done by Kumar et al. who proposed that mobilization of the shoulder must be added to the supervised exercise program to achieve goals of reducing pain, improving ROM, and function, in adhesive capsulitis.22
Small amplitude gliding movement of the joint is used to cause synovial fluid motion. That causes the nutrients exchange and thus prevents the painful effect of stasis when a joint is painful and motions are restricted.
The malposition of one bony partner concerning its opposing surface may result in limited motion or pain. With MWM correction of the positional faults results in the reduction of pain and improving the range of motion.23
The non-stretch gliding or distraction techniques applied using MWM prevent the restriction effect of immobility which causes pain and dysfunction. It is considered that further improvement in pain reduction can be achieved through the application of pain-free passive overpressure at the end of the range of motion (ROM) during MWM procedures.19,20
It is also suggested that improving function and reducing pain after MWM may be due to the promotion of active movement in this technique, which may engage additional proprioceptive tissue such as the Golgi tendon organ activated by a tendon stretch.6
Joint motion applied using ERM and MWM stimulates biological activity by moving synovial fluid which brings nutrients to the avascular articular cartilage of the joint surface. Extensibility and tensile strength of the articular and periarticular tissues are also maintained by the joint motion.
The results of the current study can be correlated with the study done by Yang et al. and Vermeulen et al. who found ERM and MWM are effective for increasing mobility and reducing pain in subjects with frozen shoulder syndrome. The proposed mechanism by which ERM and MWM increase the range of motion (ROM) is through stretching of the joint capsule and the surrounding tissues.11,12
Normal tissue regeneration and remodelling depends on mechanical stimulation during the repair process. This mechanical environment can be provided by ERM and MWM. This helps in improving
the tissues overall mechanical and physical behaviour such as tensile strength and flexibility. ERM and MWM are used to stretch and elongate the shortened tissues improving the ROM and reducing abnormal stresses on the body.
The reduction of pain and improved ROM in the present study may also be the effect attributed by the superficial healing modality which was given before the manual therapy and KT for 10 min. The application of superficial heat produces local physiological changes which resulted in therapeutic effects like the relief of pain ( pain gate mechanism, reducing muscle spasm)and improvement in ROM (tissue extensibility).
The significant reduction in pain and improved AROM and PROM contributes to improving the functioning of the shoulder joint which was assessed by the UCLA score in the current study. The UCLA score shows significant improvement in both groups. Intergroup comparison between both the groups over the period showed marginally higher improvement Group B in initial 3 weeks of intervention and then the improvement in both the groups was similar.
Functional disability and pain are related to each other and hence, these components of quality of life are in an indirect relationship with sleep disturbance which has a direct relation with pain and functional disability24. Several studies related to shoulder joint were reported.25 Articles on different parameters of related condition were reviewed.28.
The attributed effect of KT along with ERM and MWM which reduces the pain and improve the ROM significantly caused better functioning of the shoulder thus improvement in the UCLA score.25-28
It can be concluded from the present study that the application of KT as an adjunct helped to alleviate pain, improve ROM and functioning of the shoulder joint. But this improvement was seen only in the early part of the intervention i.e. from the initial day to 3 weeks with consistent improvement in both groups from 3 weeks to 6 weeks of intervention.
CONCLUSION:
The study was aimed to know the functional improvement in adhesive capsulitis by using KT as an addition to ERM and MWM which shows a significant improvement after 3rd week of treatment. And KT also serves as a good combination along with manual therapy technique to improve functional activity in patients.
CLINICAL IMPLICATION:
The present study clinically implies that the application of KT along with ERM and MWM can be useful for treating the adhesive capsulitis of the shoulder joint than ERM and MWM only. KT should be added to the intervention regimen while treating the adhesive capsulitis of the shoulder joint. KT may be helpful in subjects where immediate effects on pain, restricted ROM and functioning are required.
Conflict of interest: Nil
Source of funding: Nil
References:
-
Manske R, Prohaska D. Diagnosis and management of adhesive capsulitis. Curr Reviews in Musculoskeletal Med. 2008;1(3-4):180-189. 2.
-
Wani S, Mullerpatan R. Prevalence of shoulder dysfunction among Indian people with type II diabetes. Int J Diab Devp Count. 2015;35(3):386-386.
-
Kamble A, Ambad RS, Padamwar M, Kakade A, Yeola M. To study the effect of oral vitamin d supplements on wound healing in a patient with diabetic foot ulcer and its effect on lipid metabolism. Int J Res Pharm Sci. 2020;11(2):2701-2706.
-
Jameel PZ, Lohiya S, Dongre A, Damke S, Lakhkar BB. Concurrent diabetic ketoacidosis and pancreatitis in Paediatric acute lymphoblastic leukaemia receiving L-asparaginase. BMC Pediatr. 2020;20(1).
-
Sharma S, Tembhare A, Inamdar S, Agarwal HD. Impact of diabetic ketoacidosis in pregnancy. J SAFOG. 2020;12(2):113-115.
-
Panchbudhe SA, Praveen Kumar Y, Choudhary S, Chiwhane A. Role of the physiotherapist to promote physical activity in physical therapy settings: A questionnaire study. Intern J Cur Res Rev. 2020;12(14 Special Issue):50-55.
-
Jungade S. Manual physical therapy as a novel treatment modality for Autism spectrum disorder-A pilot study. J Compl Integr Med. 2020;17(2).
-
Thelen M, Dauber J, Stoneman P. The Clinical Efficacy of Kinesio Tape for Shoulder Pain: A Randomized, Double-Blinded, Clinical Trial. J Orthop Spor Phys Ther. 2008;38(7):389-395.
-
Roddey T, Olson S, Cook K, Gartsman G, Hanten W. Comparison of the University of California–Los Angeles Shoulder Scale and the Simple Shoulder Test With the Shoulder Pain and Disability Index: Single-Administration Reliability and Validity. Phys Ther. 2000;80(8):759-768.
-
Romeo A, Mazzocca A, Hang D, Shott S, Bach B. Shoulder Scoring Scales for the Evaluation of Rotator Cuff Repair. Clin Orthop Rel Res. 2004;427:107-114.
-
Vermeulen H, Obermann W, Burger B, Kok G, Rozing P, van den Ende C. End-Range Mobilization Techniques in Adhesive Capsulities of the Shoulder Joint: A Multiple-Subject Case Report. Physical Ther. 2000;80(12):1204-1213.
-
Yang J, Chang C, Chen S, Wang S, Lin J. Mobilization Techniques in Subjects With Frozen Shoulder Syndrome: Randomized Multiple-Treatment Trial. Phys Ther. 2007;87(10):1307-1315.).
-
Camarinos J, Marinko L. Effectiveness of Manual Physical Therapy for Painful Shoulder Conditions: A Systematic Review. J Manual & Manipulative Ther. 2009;17(4):206-215.
-
Tasto J, Elias D. Adhesive Capsulities. Sports Med Arthroscopy Rev. 2007;15(4):216-221.
-
Harma G, Aseer P, Sai P, Venkatesh N. Effects of positional coracohumeral ligament stretching on the size of calcium deposits in adhesive capsulitis. J Health Sci. 2020.
-
Sheridan M, Hannafin J. Upper Extremity: Emphasis on Frozen Shoulder. Orth Clin North Am. 2006;37(4):531-539.
-
Milgrom C, Milgrom Y, Radeva-Petrova D, Jaber S, Beyth S, Finestone A. The supine apprehension test helps predict the risk of recurrent instability after a first-time anterior shoulder dislocation. J Shoul Elb Surg. 2014;23(12):1838-1842.
-
Colaco C. Frozen shoulder: adhesive capsulitis. Bri Med J. 1981;283(6303):1402-1402.
-
Jordjevic O, Vukicevic D, Katunac L, Jovic S. Mobilization With Movement and Kinesiotaping Compared With a Supervised Exercise Program for Painful Shoulder: Results of a Clinical Trial. J Manipul Phys Ther. 2012;35(6):454-463.
-
Shukla M, Goyal M. Effect of maitland mobilization and conventional physiotherapy exercises in osteoarthritis knee: a comparative study. Int J Physiot Res. 2018;6(6):2952-2956.
-
Kaya E, Zinnuroglu M, Tugcu I. Kinesio taping compared to physical therapy modalities for the treatment of shoulder impingement syndrome. Clin Rheum. 2010;30(2):201-207.
-
Kumar A, Kumar S, Aggarwal A, Kumar R, Das P. Effectiveness of Maitland Techniques in Idiopathic Shoulder Adhesive Capsulities. ISRN Rehabilitation. 2012;2012:1-8.
-
Kamat SD. Efficacy of mobilization with movement and Kinesio taping versus mobilization with movement and conventional exercises in patients with shoulder impingement: a comparative study. MPTh thesis, Rajiv Gandhi Univ Health Sci. 2012;3(1): 123-126.
-
Fernandes M. Correlation between functional disability and quality of life in patients with adhesive capsulitis. Acta Ortop Brasil. 2015;23(2):81-84.
-
Singh R. Singam A. Comparison between Supraclavicular and Interscalene Brachial Plexus Block in Patients Undergoing Shoulder Surgery. J Datta Meghe Inst Med Sci Univ. 14, no. 3 (2019): 175–78.
-
Khobragade S. Naqvi S. Dhankar W, Jungade S. Impact of K-Taping on Sacroiliac Joint Pain in Women after Full-Term Normal Delivery. J Datta Meghe Inst Med Sci Univ 2019;14(4): 352–55.
-
Meshram, P., A. Pawaskar, and A. Kekatpure. “3D CT Scan-Based Study of Glenoid Morphology in Indian Population: Clinical Relevance in Design of Reverse Total Shoulder Arthroplasty. J Clin Orthop Trau. 2020; 11: S604–9.
-
Saoji KK, Gawande V, Dulani R. A Comparative Study of Disability and Pain Assessment by Shoulder Pain and Disability Index (Spadi) Score in Patients of Adhesive Capsulitis Treated by Hydrodilatation with and without Corticosteroids. Int J Curr Res Rev.2020; 12,(14): 35–40.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





