IJCRR - 13(7), April, 2021
Pages: 34-39
Date of Publication: 12-Apr-2021
Print Article
Download XML Download PDF
Estimation of Fluoride Levels in Drinking Water and its Association with Acquired Hypothyroidism in Children - A Prospective Observational Study
Author: Srinivasan Purusothaman, Lal DV, Radha Kumar
Category: Healthcare
Abstract:Introduction: The thyroid hormone is essential for growth and development in children. Acquired hypothyroidism is sporadic in occurrence and commonly occurs due to autoimmune Hashimoto's thyroiditis. Fluoride can interfere with the normal functioning of the thyroid gland by competing with iodine for uptake and lead to delayed development, degeneration as well as impairment of brain function. Objective: The study aimed to assess fluoride levels in drinking water and their association with acquired hypothyroidism. Methods: A prospective observational study was conducted in which children were screened for symptoms of acquired hypothy�roidism and underwent thyroid function tests. The children with elevated thyroid-stimulating hormone (TSH) levels were included in the study and the fluoride content of drinking water was measured. Results: Out of 153 children who underwent thyroid profile, 45 children were diagnosed with acquired hypothyroidism based on elevated TSH level. The commonest clinical presentation in the study population was fatigue (57%), dry hair (42 %) and consti�pation (31%). The mean TSH level was 31.21(mIu/L) and the mean fluoride content in drinking water was 0.462, the minimum and the maximum level were 0. 10 mg/l and 1. 20 mg/l respectively. Conclusion: In our study, the majority of children (58 %) were consuming pipeline water from panchayat or municipal source. The mean fluoride content in drinking water of children with acquired hypothyroidism was normal (0.462 ppm) and only 3 children consumed water with high fluoride content (> 1ppm). Children with low FT3 and low FT4 had normal fluoride levels in drinking water. There was no statistically significant correlation between FT3 ((R=0.23: P=0. 12) and FT4 ((R=0.21: P=0. 17) levels with fluoride levels in the drinking water. More studies with a large sample size have to be conducted to assess for any positive cor�relation between high fluoride and thyroid dysfunction.
Keywords: Acquired hypothyroidism, Drinking water, Fluoride levels, Thyroid-stimulating hormone, Groundwater, Iodine deficiency
Full Text:
INTRODUCTION
Fluorosis and Iodine Deficiency Disorders (IDD) are endemic disorders in India and co-occur in certain parts of the country.1 Endemic fluorosis resulting from high fluoride concentration in groundwater is a public health problem in India as it is located in the geographical fluoride belt extending from Turkey to China and Japan through Iraq, Iran and Afghanistan.2,3 Previous studies reveal that 15 States in India are endemic for fluorosis with fluoride level in drinking water >1.5 mg/l, leading to dental, skeletal and non-skeletal fluorosis.1,4,5 Among those affected, 6 million are children below the age of 14 years.5
Fluoride is naturally present in low concentration (0.01–0.3 ppm) in surface rain or river water. Fluoride levels in groundwater (well water) concentrations can vary, depending on the mineral composition of the local ground and in some locations, the drinking water contains dangerously high levels of fluoride leading to serious health problems.2,3 Fluoride can interfere with the function of the thyroid gland and lead to delayed development in children as well as impairment of brain function.6-8 Since fluoride is more electronegative than iodine, it easily displaces iodine, thereby affecting the functioning of the thyroid gland. Fluoride has been known to produce biochemical changes within the body of an individual, which included deranged thyroid hormonal levels. A negative feedback mechanism regulates the production of thyroid hormones in the body by releasing TSH from the anterior pituitary gland following a drop of T3 levels in circulation. TSH stimulates the thyroid gland which in turn accelerates the production of the thyroid hormone T4, now considered a “pro-hormone”. Most the circulating T3 arises from peripheral deiodination of T4 and not from thyroid secretion. The process of deiodination is catalysed by the enzyme iodothyronine deiodinases and fluoride is known to interfere with the activity of the deiodinases enzyme.
In optimally fluorinated parts of the world, the daily dietary intake of fluoride is 0.05 mg/kg/day whereas the dietary intake of fluoride is much lower in children from developing countries. The upper limit of fluoride concentration by the World Health Organization (WHO) in drinking water at 1.5 mg/litre. The maximum daily limit of fluoride intake as per Bureau of Indian Standards is 1.0 mg/l and the “lesser the better”.6 Whenever the intake of fluoride is higher than the optimum level, it can lead to dental and skeletal fluorosis.
Since there are only a few population studies in children that examine the association of thyroid disease with fluoride intake in water, our study was performed to determine if acquired hypothyroidism in the children is related to consuming water with excess fluoride content.
MATERIAL AND METHODS
Study design: Hospital-based prospective study
Period of study: June 2016 to May 2017
Study area: Department of Paediatrics, Saveetha Medical College Hospital, Chennai.
Study sample: All children with clinical symptoms and signs of acquired hypothyroidism in the age group 5 to 15 years who presented to the Paediatric outpatient department were enrolled in the study. A sample of 45 children during the study period diagnosed with acquired hypothyroidism was included in the study. Symptoms of hypothyroidism which were included were poor physical growth, poor concentration, poor scholastic performance, fatigue, weak muscles, depression, dry and itchy skin, unusual hair loss, dry hair, cracking nails, infrequent bowel movements or hard stools, unexplained weight gain, swelling at the front of the neck, difficulty in tolerating cold and menstrual disturbances in adolescent girls.
Inclusion criteria: All children aged 5 years to 15 years presenting with clinical features of acquired hypothyroidism.
Exclusion criteria: Children diagnosed with congenital hypothyroidism, unwillingness to participate in study and children with any pre-existing or severe concurrent severe comorbid illness.
Procedure: After obtaining a detailed history, general examination, anthropometry and examination of the neck was done. Informed written consent about the study was obtained from the parents or guardian. Blood samples were taken for estimation of thyroid profile. Only those children who were confirmed as the case of acquired hypothyroidism were included in the study. Information about the usual source of drinking water was collected. Participants were asked about the primary source of drinking water at their current residence whether municipal water supply, groundwater, bottled water, reverse osmosis water (RO) treated or others and for how long they have been consuming the water.RO is a water purification process that uses a partially permeable membrane to remove ions, unwanted molecules and larger particles from drinking water. For those children who were confirmed as overt hypothyroidism (based on the abnormal thyroid profile), the drinking water samples (minimum 50 ml, maximum 200 ml in a Special plastic bottle provided for the sample analysis) was collected on a follow-up visit and sent to Ekdant Enviro services Pvt limited, Chennai which is a NABH accredited lab to estimate the fluoride levels. Test to detect fluoride level was performed upon the water samples as per the World Health Organisation recommendation. Correlation between the fluoride levels in water and hypothyroidism.
Sample size and sampling technique: Prevalence of acquired hypothyroidism in school children is around 3-4%, and assuming 5% precision and 95% confidence interval, statistically significant sample size came out to be 39. Hence 45 children between 5-15 years were recruited by Consecutive sampling. The study was conducted over one year. International Business Machines (IBM) SPSS version 22 was used for statistical analysis.
Statistical methods: The primary outcome variables were: Free T3, Free T4, TSH.Primary explanatory variable: Fluoride content in drinking water.Secondary explanatory variable: Age, gender, family history of disorders, height and weight.
Inferential statistics: Quantitative outcome-The mean values were compared with the quantitative outcome and categorical variables. The differences between mean levels of FT3, FT4, TSH with mean fluoride levels with 95% confidence intervals were assessed. Statistical significance was done using an Independent sample t-test/ ANOVA. The association of variables Pearson correlation coefficient and the data was represented in a scatter diagram. Linear regression analysis was done. The regression coefficient, along with its 95% Confidence Intervals ( CI )and P values is presented. Categorical outcome - The association between explanatory variables and categorical outcomes was assessed by cross-tabulation and comparison of percentages. Odds ratio along with 95% CI are presented and the Chi square test was used to test statistical significance. P-value > 0.05 was considered statistically insignificant whereas P-value ≤ 0.05 was considered statistically significant.
RESULTS
The total number of children who presented with clinical features of acquired hypothyroidism were 156 out of which 3 parents refused consent for blood sampling. A thyroid profile was performed for the remaining 153 children and 45 children had elevated TSH levels while 108 children had normal TSH levels. The 45 children with elevated TSH were included in the study.
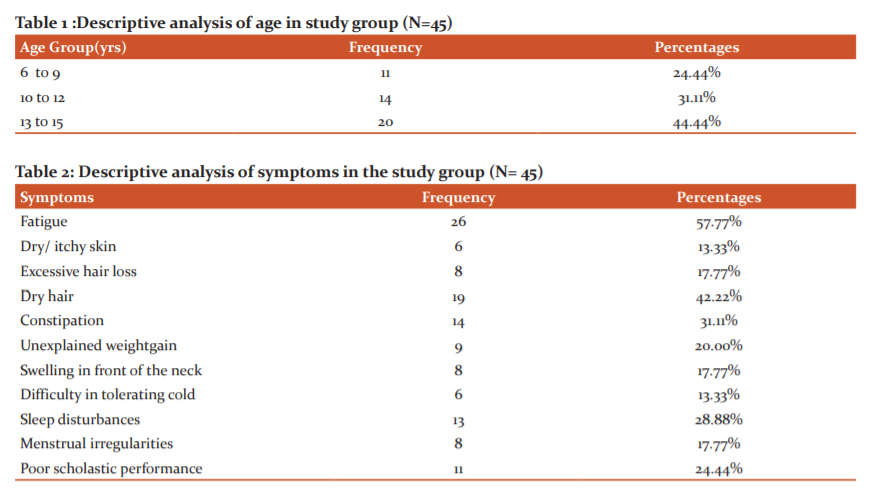
Out of the total of 45 children who were analysed, the mean age was 11.51 years with a minimum age of 6 years and maximum of 15 years of age in the study (95% CI 10.74 - 12.28). 24.44% of children were between the age group of 6 to 9 years whereas children in the age group of 10 to 12 years and 13 to 15 years was 31.11% and 44.44% respectively. In the study, 75.56% were girls and 24.44% were boys (Table 1).
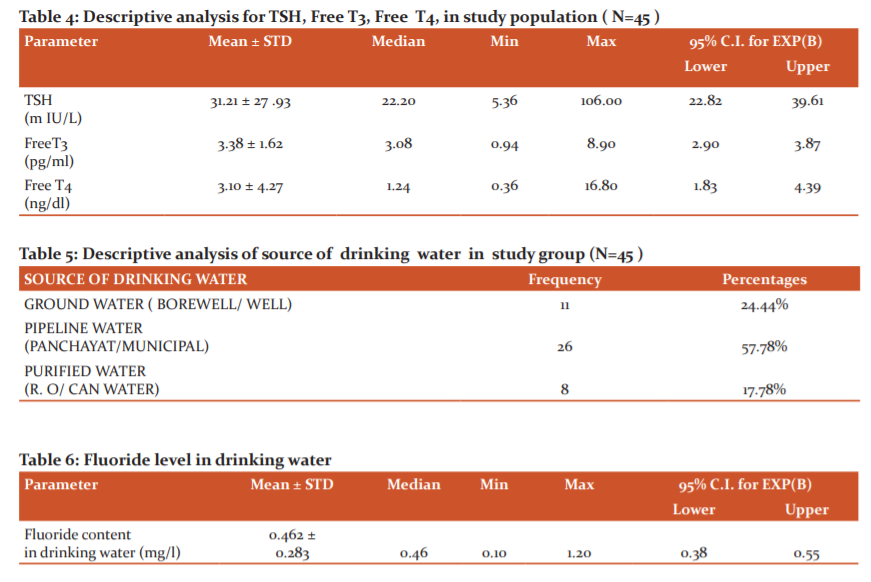
Among the study population, 57.77% of children had symptoms of fatigue. Dry and itchy skin was present in 13.33%whereas 17.7 % complained of excessive hair loss and 42.2 % had dry hair. The proportion of constipation, unexplained weight gain, swelling in front of the neck, difficulty in tolerating cold, sleep disturbances, menstrual irregularities history of poor scholastic performance were 31.11%, 20%, 17 .77 %, 13.33%, 28. 88%, 17.77%, 24.44% respectively. In the study population, 33.33% had a positive family history of thyroid disorder. As seen in Table 3, among the study population, 71.11% of children had age-appropriate weight ( 5 to - 95th centile) as per the CDC growth chart. 10 (22.22 %) children and 3 ( 6.66%) children had weight for age less than < 5th centile (undernourished) and weight for age > 95 the centile as per CDC growth chart respectively. The mean TSH of the study population was 31.21 with a minimum of 5.36 and a maximum of 106 (95% CI 22.82 - 39. 61 ) as seen in table 4. The mean Free T3 was 3.38 with a minimum of 0.94 and a maximum of 8.90 (95% CI 2.90 – 3.87 ). The mean Free T4 was 3.10 with a minimum of 0.36 and a maximum of 16.80 (95 % CI 1.83 – 4. 39) (Table 2).
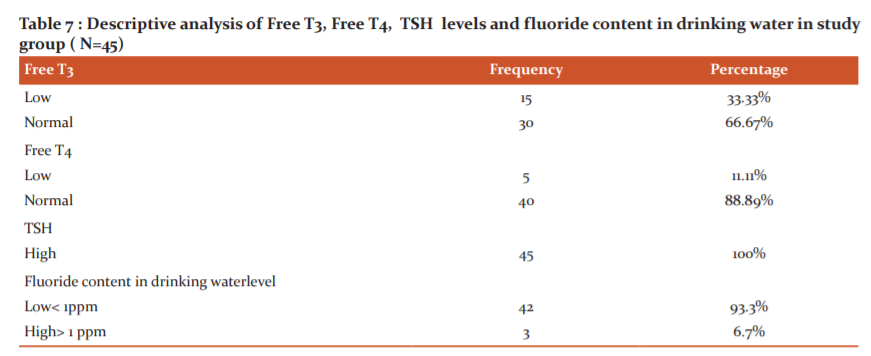
Among the study population, the majority of them were consuming pipeline water ( panchayat / municipal) 57.78% while groundwater (bore well/ well) and purified water (R.O/ can water) was consumed by 24 .44 % and 17.78% respectively as seen in table 5. The mean fluoride content in drinking water was 0.462, the minimum and the maximum levels were 0. 10 mg/l and 1. 20 mg/l respectively as seen in table 6. Most of the patients were consuming a permissible range of fluoride levels in drinking water. In the study all children had high TSH level as seen in table 7. 15 children (33.33 %) had low values and 30 children (60.67%) had normal levels of Free T3; whereas FT4 measurements showed low and normal values in 5 ( 11.11%) and 40 (88. 89%) children respectively. The Fluoride content in drinking water was low in 42 children (93.3 %) and high in 3 children (6.7%). Ethical clearance number:0Z8/08/2016/KEC/SU.
DISCUSSION
Iodine is an important microelement required by the body for neural development and neuronal functioning. Consumption of drinking water with high Fluoride levels for long periods can lead to acquired hypothyroidism since iodine gets easily displaced by fluoride. Fluoride can inhibit TSH release from the pituitary gland, thereby reducing thyroid hormone release.4
In our study, the mean age of presentation of acquired hypothyroidism was 11.51 years. The majority of the participants were females (75.56%). A similar male to female ratio of 1:3 was reported by Shah NA et al in their study of 50 children.9 Contrastingly, the proportion of females in the study by Peckham et al was equal (49.9%) to that of males.7 In our study goitre was present in 17.77% of cases, fatigue in 57.77%, cold intolerance in 13. 33%, short stature in 20. 00% and constipation by 31.11 %. In contrast, the study by de Vries et al showed that goitre was present in 77. 2% of cases, fatigue in 21.6%, cold intolerance in 6.9 %, and constipation in 5.9% of cases.10 In a study by Al-Agha AE et al the commonest clinical presentations were short stature (32 .5 %), fatigability ( 12.1%), constipation (9.8%), cold intolerance (5. 3 %), goitre ( 2.6%) and menstrual irregularities 7.9%.11
Among the study population, 24.44% of patients consumed groundwater from either bore well or well. The proportion of pipeline water (panchayat/ municipal) was 57 .78 % and the proportion of purified water (RO/ can water) was 17.78%. In our study, the mean Fluoride content in drinking water was 0.462ppm the minimum level was 0.10ppm and the maximum level was 1.20 ppm in the study population. The recommended level of fluoride in drinking water in India is 0.5 to 0. 8 mg/l.7 In their study, Singh N et al reported a higher concentration of fluoride in drinking water of both cases (1. 6 - 5.5ppm) and controls (0. 98 -1ppm) with acquired hypothyroidism.12 Therefore it is important to test fluoride levels of drinking water in children with acquired hypothyroidism.
In their hospital-based study of 275 patients, Sachdeva et al. categorised the patients into 3 groups based on the source of drinking water.14 They found that the mean fluoride level group A (consuming groundwater), were 2.50±1.27 mg/dl, in group B (municipal water) it was 0.82±0.07 mg/ dl and in group C ( reverse osmosis water) it was 0.76 ±0. 11 mg/ dl. The mean TSH levels were 9.66 ± 4 .02, 7. 48 ± 3 .21 and 8.38 ± 4.28 respectively. The mean FT3 levels were 3. 76 ± 1. 41, 4.13 ± 2. 13 and 4.02 ± 2.30 respectively.
In our study, the mean TSH in the study population was 31.21 m IU/L with a minimum of 5. 36 and a maximum of 106 in the study population ( 95% CI 22.82 - 44.65). The mean Free T3 was 3. 38 with a minimum of 0. 94 and maximum 8 .90 (95% CI 2. 90 – 3.87). The mean Free T4 was 3.10 with a minimum of 0.36 and a maximum of 16. 80 (95% CI 1. 83 – 4.39). In their case-control study, Singh N et al found significantly higher mean TSH levels between the groups ( 3.7+/ - 1. 9), while the mean FT3 levels (3 . 07+/- 1. 1) and mean FT4 levels ( 1.19+/- 0.21) was non-significant.12
Though children with low free T3 levels were consuming relatively higher fluoride content water (0.502 ppm) compared to those with normal free T3 levels having water with a fluoride level of 0.442 ppm, the difference was not statistically significant. 37 Children who consumed water with low fluoride levels had normal FT4 (88 .09 %) and 5 of them had low FT4(11.9%). Out of 3 children who drank water with high Fluoride content, all had a normal level of FT4. In our study, there was a non-significant correlation between the either with FT3 (R=0.23: P=0. 12) levels or FT4 (R=0.21: P=0. 17) levels with fluoride levels in the drinking water. A similar insignificant correlation with the values of FT3 and FT4 was observed by Singh et al.12 Previous evidence suggests that intake of the high level of fluoride can interfere with thyroid gland function with derangements of thyroid hormone levels. 12,13Excess of fluoride in drinking water, especially groundwater has been shown to demonstrate a linear correlation with raised TSH levels, most of which are subclinical. Also, fluorosis is known to compound its detrimental effects in areas previously deficient in their iodine status.14
Susheela et al compared thyroid hormone status of 90 children with dental fluorosis (drinking water fluoride ranging from 1.1 to 14.3 mg/L) and 21 children without dental fluorosis (0.14?0.81 mg/L fluoride in drinking water) in areas where iodine supplementation was considered adequate.15 They reported that 49 (54.4%) children had “well?defined hormonal derangements; findings were borderline in the remaining 41 children. In another study conducted among school children in the Nalgonda district, the prevalence of dental caries was more in below optimal fluoride area followed by areas where fluoride concentration was 5 ppm and above.16
Limitations of the study were that sample size was small, other source of fluoride consumption were not included in the study, fluoride level measurements were not done in serum and body fluids and serum auto-antibodies levels were not measured.
CONCLUSION
In our study, there was no significant correlation between TSH levels, FT3 levels and FT4 levels with fluoride levels in the drinking water. Fluoride levels in the drinking water of most of the study participants were within the permissible range. Only 3 children had fluoride level of more than 1 ppm. Though permissible drinking water fluoride content in India is <1 mg/l, recent studies suggest fluoride level >0.7 mg/l can have an effect on the thyroid gland causing hormone derangement. Acquired hypothyroidism is a common endocrine disorder and few population studies examine the association of this disease with fluoride intake. More studies with a large sample size have to be conducted to assess for any positive correlation between high fluoride and thyroid dysfunction.

ACKNOWLEDGEMENT
The authors acknowledge the immense help received from the scholars whose articles are cited and included in references to this manuscript. The authors are also grateful to authors/editors / publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed
CONFLICT OF INTEREST: NIL
SOURCE OF FUNDING: NIL
References:
-
Hetzel BS PB, Dulberg EM. The iodine deficiency disorders: nature, pathogenesis and epidemiology. World Rev Nutr Diet 1990;62:59–119.
-
Kotecha PS, Bhalani KD, Shah D, Shah VS, Mehta KG. Prevalence of dental fluorosis & dental caries in association with high levels of drinking water fluoride content in a district of Gujarat, India. Indian J Med Res 2012;135(6):873–877.
-
Saravanan S, Vijayarani M, Jayakodi P, Felix A, Nagarajan S. Prevalence of dental fluorosis among primary school children in rural areas of Chidambaram Taluk Cuddalore District, Tamil Nadu. India. Indian J Commun Med 2008;33:146-150.
-
NRC. Fluoride in drinking water: a scientific review of EPA’s standards. Washington DC; 2006.
-
AK S. Fluorosis: Indian scienario: A treatise on fluorosis. New Delhi, India: Fluorosis Research and Rural Development Foundation; 2001
-
Ha H CZ, Liu XM .The influence of fluoride on human embryo. Chin J Ctrl Endem Dis 1989;4:136–137.
-
Peckham S, Lowery D, Spencer S. Are fluoride levels in drinking water associated with hypothyroidism prevalence in England? A large observational study of GP practice data and fluoride levels in drinking water. J Epidemiol Community Health 2015;69(7):619-624 .
-
Newton JN, Young N, Verne J, Morris J. Water fluoridation and hypothyroidism: results of this study need much more cautious interpretation. J Epidemiol Community Health 2015;69(7):617-618.
-
Shah NA MP, Bhalodia JN, Desai NJ. Evaluation of thyroid diseases by hormonal analysis in pediatric age group. Natl J Med Res 2013;3(4):367-70.
-
de Vries L, Bulvik S, Phillip M. Chronic autoimmune thyroiditis in children and adolescents: At presentation and during long-term follow-up. Arch Dis Child 2009;94:33-37.
-
Al-Agha AE, Alshugair RM, Aljunedi WA, Badakhan BA. Clinical Presentation of Acquired Hypothyroidism and Associated Disorders in Children and Adolescents at King Abdul- Aziz University Hospital in a Western Region of Saudi Arabia. J Pat Care 2016;2:3.
-
Singh N VK, Verma P, Sidhu GK, Sachdeva S. A comparative study of fluoride ingestion levels, serum thyroid hormone & TSH level derangements, dental fluorosis status among school children from endemic and non-endemic fluorosis areas. Springerplus 2014;3:7.
-
Xiang Q CL, Liang Y, Wu M. Fluoride and thyroid function in children in two villages in China. J Toxicol Environ Health Sci 2009;1:54–59.
-
Sachdeva S, Ahmed J, Singh B. Thyroid dysfunction associated with excess fluoride intakes: Scope for primary prevention. Thyroid Res Pract 2015;12(2).
-
Susheela AK, Bhatnagar M, Vig K, Mondal NK.Excess fluoride ingestion and thyroid hormone derangements in children living in Delhi. Fluoride 2005;38:98-108.
-
Desai VC, Manjula M, Reddy RE, Shaik H. Prevalence of dental caries at different levels of fluoride ion concentrations among the school children in Nalgonda district. Int J Curr Res Rev 2013;5(5):135-139.
|
 IJCRR
IJCRR 





 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License





